
Abstract
PURPOSE Approximately 50,000 adults die annually from vaccine-preventable diseases in the United States. Most traditional vaccine providers (eg, physician offices) administer vaccinations during standard clinic hours, but community pharmacies offer expanded hours that allow patients to be vaccinated at convenient times. We analyzed the types of vaccines administered and patient populations vaccinated during off-clinic hours in a national community pharmacy, and their implications for vaccination access and convenience.
METHODS We retrospectively reviewed data for all vaccinations given at the Walgreens pharmacy chain between August 2011 and July 2012. The time of vaccination was categorized as occurring during traditional hours (9:00 am–6:00 pm weekdays) or off-clinic hours, consisting of weekday evenings, weekends, and federal holidays. We compared demographic characteristics and types of vaccine. We used a logistic regression model to identify predictors of being vaccinated during off-clinic hours.
RESULTS During the study period, pharmacists administered 6,250,402 vaccinations, of which 30.5% were provided during off-clinic hours: 17.4% were provided on weekends, 10.2% on evenings, and 2.9% on holidays. Patients had significantly higher odds of off-clinic vaccination if they were younger than 65 years of age, were male, resided in an urban area, and did not have any chronic conditions.
CONCLUSIONS A large proportion of adults being vaccinated receive their vaccines during evening, weekend, and holiday hours at the pharmacy, when traditional vaccine providers are likely unavailable. Younger, working-aged, healthy adults, in particular, accessed a variety of immunizations during off-clinic hours. With the low rates of adult and adolescent vaccination in the United States, community pharmacies are creating new opportunities for vaccination that expand access and convenience.
INTRODUCTION
The National Foundation for Infectious Diseases estimates that 50,000 adults die annually from vaccine-preventable diseases in the United States.1 Although childhood vaccination rates exceed 90% for most recommended vaccines,2 adult vaccination rates are all below national goals. Adult immunization rates for recommended vaccines range from a low of 14% for the herpes zoster vaccine to a high of 64% for the tetanus vaccine (the rate for the tetanus, diphtheria, and pertussis vaccine is 8.2%).3 Influenza vaccination is recommended for all individuals aged 6 months and older. In a given season, approximately 23,000 influenza-associated deaths occur, mostly in adults.4 Adult influenza vaccination rates vary widely, but they average just 40.5%, with the highest rates seen in those aged 65 years and older (69.6%).5
Community pharmacies are uniquely positioned to increase immunization rates in the United States. In a 2009 survey, only 20% to 30% of internists and family physicians stocked all vaccines recommended by the Centers for Disease Control and Prevention (CDC), with nearly 80% not planning to increase their offerings and 2% planning to stop carrying them altogether.6 The CDC refers to pharmacies as nontraditional locations for receiving vaccines, offering advantages such as community-based locations, access, and convenience.7 In the 2010–2011 influenza season, 18.4% of people were vaccinated in a store (eg, supermarket or drug store).8 Evidence in the medical literature suggests that pharmacies have the capacity to influence previously difficult-to-reach populations, including the medically underserved.9–13 Pharmacies may be especially effective in immunizing high-risk older adults, who are more likely to use pharmacy services for prescription medication than the general population.14 Little is known, however, about the vaccination behaviors of younger working-aged adults.
Whereas most traditional providers (eg, primary care physician offices) administer vaccinations during traditional clinic hours (9:00 am to 5:00 pm, Monday through Friday),15 community pharmacies often offer expanded hours that allow patients to receive vaccinations at more convenient times. The objectives of this study were to analyze the types of vaccines administered and patient populations vaccinated during off-clinic hours in a national community pharmacy, and implications for vaccination access and convenience.
METHODS
Study Design and Population
We retrospectively analyzed all vaccinations administered at the Walgreens pharmacy chain between August 1, 2011, and July 31, 2012. Pharmacy records for all immunizations administered at the pharmacy during the study period were identified. At the time of the study, there were more than 7,800 Walgreens pharmacies located in 49 states (North Dakota did not have any), the District of Columbia, and Puerto Rico that provided immunization services. More than 26,000 Walgreens pharmacists have completed the American Pharmacist Association’s Pharmacy-Based Immunization Delivery Training.
We categorized the time of vaccination as occurring during traditional hours (9:00 am to 6:00 pm weekdays) or off-clinic hours, consisting of weekdays 6:00 pm to 9:00 am, weekends, and 10 federal holidays—New Year’s Day, birthday of Martin Luther King, Jr, Washington’s Birthday, Memorial Day, Independence Day, Labor Day, Columbus Day, Veterans Day, Thanksgiving Day, and Christmas Day.16 We identified the type of vaccine from the Food and Drug Administration’s 11-digit National Drug Code.
Demographic characteristics of the patients vaccinated during the study period were noted, including their age and sex, urban vs other residence, and any chronic conditions, based on the Medical Condition Code as developed by Medi-Span.17 Population density area of residence was classified as metropolitan, micropolitan, small town, or rural based on zip codes of the patient address according to the Rural Urban Commuting Area codes.18
We classified patients as insured (having private or government insurance, or redeeming a voucher to receive a vaccination) or uninsured at time of vaccination. Patients were classified as receiving a vaccination in a state in which pharmacists are authorized to administer either (1) all CDC-recommended immunizations per protocol or with a patient-specific prescription, or (2) selected CDC-recommended immunizations limited to influenza, pneumonia, zoster, or some combination thereof.19 Vaccine type was classified as either a vaccine included on the CDC adult or adolescent recommended immunization table20,21 or other vaccine approved by the Food and Drug Administration (eg, for travel), consisting of typhoid, yellow fever, rabies, and Japanese encephalitis. We also noted the number of vaccines a patient received during the year as well as whether patients picked up a prescription medication at the time of vaccination.
Statistical Analysis
We first used univariate analyses to describe the temporal distribution of vaccinations, type of vaccine, and patient characteristics in the study population, and their use of traditional and off-clinic hours for vaccination. Percent of traditional clinic and off-clinic use were detailed for each subgroup of patients identified by the characteristics studied.
We conducted logistic regression analysis using the patient characteristics and pharmacy use variables. The model consisted of age category, sex, urban classification, presence of 1 or more chronic conditions, patient insurance status, state-level pharmacist immunization privilege for CDC-recommended vaccinations, vaccine type, number of vaccinations received, and whether the patient picked up a prescription medication at the time of vaccination. These factors were hypothesized to be predictors of pharmacy-based immunization services. The results of the model are presented as odds ratios (ORs) predicting the likelihood a patient with a given characteristic would use off-clinic hours for their vaccination.
Statistical significance was assessed at the α = .05 level. All data analysis was performed with SAS 9.2 software (SAS Institute Inc). This study was approved by the Quorum institutional review board under protocol 26510.
RESULTS
Distribution of Vaccinations
During the study period, 6,250,402 vaccinations were administered to the study population. Of these, 85.0% were for influenza and 15.0% were for other vaccine-preventable diseases: herpes zoster (shingles); pneumonia; tetanus, diphtheria, and acellular pertussis (Tdap); meningitis; typhoid; hepatitis A and/or B (hepatitis); human papillomavirus (HPV); measles, mumps, and rubella (MMR); varicella zoster (chicken pox); yellow fever; rabies; polio; and Japanese encephalitis—in order of greatest to least frequency.
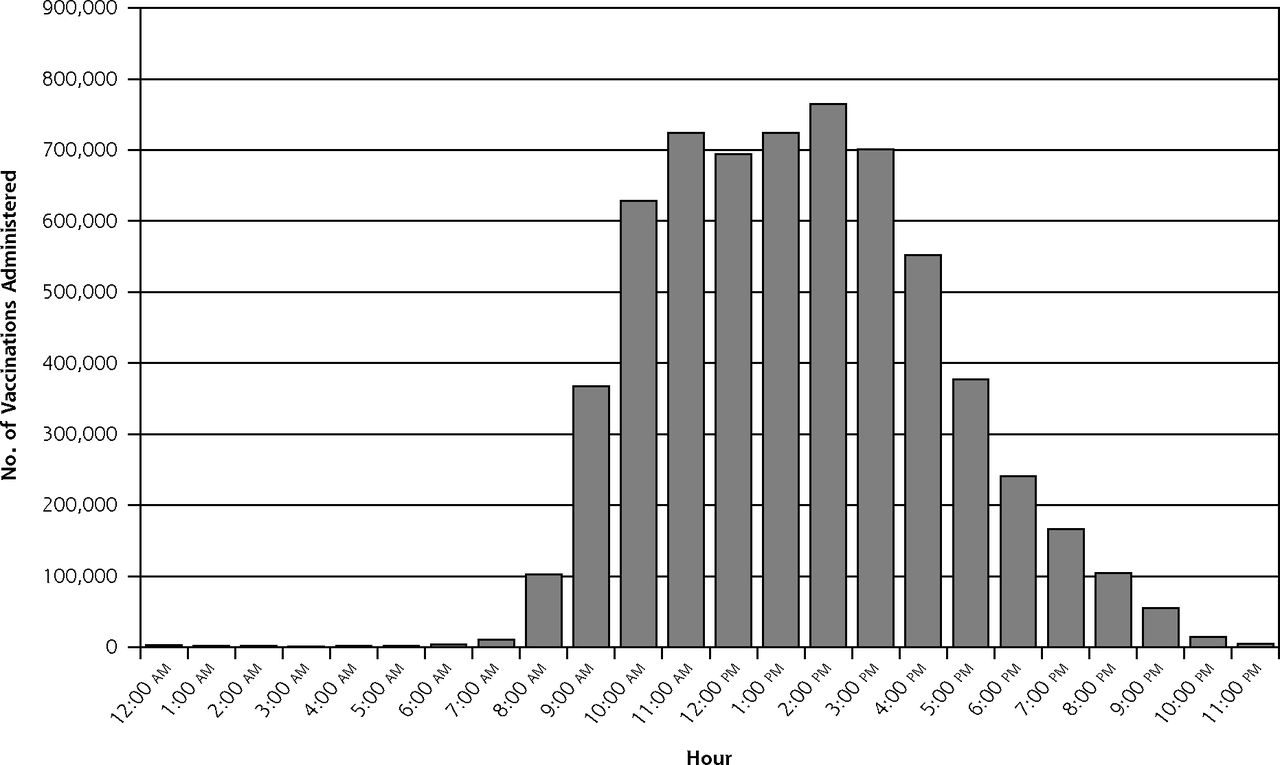
By time, 4,344,050 (69.5%) of the immunizations were administered during traditional clinic hours, and 1,906,352 (30.5%) were administered during off-clinic hours (Table 1). Of the total vaccinations administered, 17.4% were on weekends, 10.2% on evenings, and 2.9% on holidays. There were 1,093,128 vaccinations (17.5% of all vaccinations) administered during lunch hours, defined as weekdays 11:00 am to 1:00 pm, and 150,366 vaccinations (2.4% of all vaccinations; 7.9% of off-clinic vaccinations) were administered during overnight hours (10:00 pm to 9:00 am) (Figure 1). The smallest number of vaccinations, 1,680 (0.03% of all vaccinations), was administered between 3:00 am and 4:00 am.
Temporal Distribution of All Vaccinations Administered
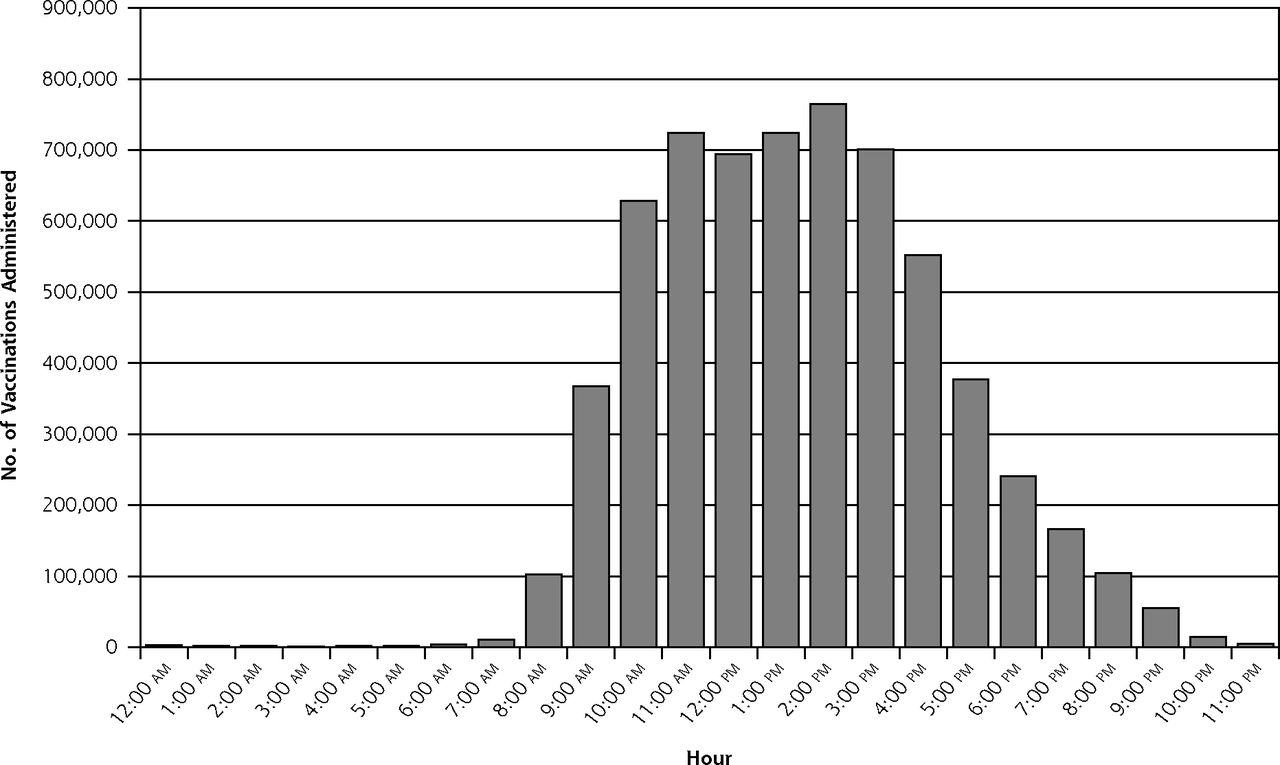
Hourly distributions of vaccinations.
Source: Walgreens pharmacy claims data, August 2011 through July 2012.
The vaccine types with the greatest proportion administered during off-clinic hours were typhoid (41.5%), Tdap (34.5%), HPV (33.8%), varicella zoster (31.6%), influenza (31.5%), hepatitis (31.4%), and yellow fever (30.8%) (Figure 2).

Vaccinations with the greatest proportion administered during off-clinic hours.
Tdap = tetanus, diphtheria, and acellular pertussis; HPV = human papillomavirus; hepatitis = hepatitis A and/or B.
a Vaccines for polio; measles, mumps, and rubella (MMR); meningitis; pneumonia; rabies; herpes zoster (shingles); and Japanese encephalitis.
Source: Walgreens pharmacy claims data, August 2011 through July 2012.
Demographics of Study Population
Table 2 displays traditional clinic and off-clinic hour vaccinations administered by patient characteristics and pharmacy use. For the 5,787,970 unique patients vaccinated, the average age was 60.8 years during traditional hours and 53.1 years during off-clinic hours. Among patients aged younger than 65 years, 39.0% received their vaccinations during off-clinic hours. About one-third of both men (32.5%) and women (30.4%) did so.
Vaccinations Administered According to Time, by Patient Characteristics and Pharmacy Use
Among patients stratified by the population density classifications, the largest proportion receiving vaccinations during off-clinic hours resided in metropolitan areas (32.3%). The proportion vaccinated during off-clinic hours was similar for patients without vs with chronic conditions (31.9% vs 30.5%) but greater for uninsured patients vs insured patients (37.6% vs 29.7%).
Pharmacy Use of Study Population
Among patients who received a travel or other vaccine not routinely recommended by the CDC, 40.3% were vaccinated during off-clinic hours, compared with 31.3% of patients receiving a CDC-recommended vaccination. The proportion of patients vaccinated during off-clinic hours was generally similar among patients receiving multiple vs single vaccines during the year (33.9% vs 31.1%) and among patients also picking up a prescription as compared with those just receiving a vaccine (31.5% vs 31.3%).
Predictors of Vaccination During Off-Clinic Hours
Table 3 displays the multivariate adjusted ORs with 95% CIs for vaccination during the off-clinic hours. With respect to patient characteristics, patients were more likely to be vaccinated during off-clinic hours if they were male vs female (OR = 1.080; 95% CI, 1.076–1.084) and if they resided in a metropolitan area (OR = 1.336; 95% CI, 1.319–1.353). On the other hand, patients were less likely to be vaccinated during off-clinic hours if they were aged 65 years or older vs younger (OR = 0.447; 95% CI, 0.445–0.449), had at least 1 chronic condition (OR = 0.980; 95% CI, 0.976–0.983), or had insurance (OR = 0.991; 95% CI, 0.987–0.996).
Adjusted Associations of Patient Characteristics and Pharmacy Use With Vaccination During Off-Clinic Hours
With respect to pharmacy characteristics and vaccination-related factors, patients were more likely to use off-clinic hours if they were vaccinated in states that authorize pharmacists to administer all CDC-recommended vaccines vs states that authorize pharmacists to administer only influenza, pneumonia, and zoster vaccines (OR = 1.044; 95% CI, 1.040–1.049), if they received travel vaccines vs routine CDC-recommended vaccines (OR = 1.166; 95% CI, 1.137–1.195), and if they received multiple vaccines at the pharmacy during the year (OR = 1.353; 95% CI, 1.343–1.363). Picking up a prescription medication at the time of vaccination did not significantly influence off-clinic use (OR = 1.000; 95% CI, 0.994–1.005).
DISCUSSION
Key Findings
In our study of more than 6 million vaccinations administered in more than 7,500 pharmacies nationwide, we focused on immunization services during hours outside of traditional medical clinic hours. The off-clinic population received immunizations from 6:00 pm to 9:00 am, Monday through Friday, and any time on weekends and US federal holidays. Results show that approximately 30% of the study population received 1 or more vaccinations during these off-clinic hours. Almost 200,000 patients were vaccinated on a federal holiday, most often Columbus Day and Veterans Day. As these holidays occur in October and November, respectively, and coincide with typical influenza season in the northern hemisphere, expansion of pharmacy hours to include these holidays facilitates access and convenience for influenza vaccinations (as well as others) during a time when traditional providers are not likely available.
Results of this study also illustrate the access and convenience that community pharmacies provide for the typical working-aged population (aged 18–49 years). More than 1 million vaccinations took place during lunch hours (11:00 am to 1:00 pm), possibly demonstrating use of these hours by patients working traditional workday hours of 9:00 am to 5:00 pm. For this population, community pharmacies may offer a more convenient and time-efficient avenue for vaccination than physicians’ offices. Furthermore, the more than 150,000 vaccinations that occurred during the overnight hours of 10:00 pm to 9:00 am demonstrate the value that 24-hour community pharmacies may provide to nightshift workers. According to the US Bureau of Labor Statistics, 15 million Americans work during overnight hours, either on a regular or occasional basis.22 For this population, 24-hour pharmacies may provide immediate access to vaccinations during their break time. In the workplace, absenteeism and productivity have been shown to improve with influenza vaccination.23,24 Allowing the working population to use convenient times outside of respective work hours to be vaccinated may thus increase vaccination rates and improve productivity.
Individuals receiving travel vaccines used off-clinic hours approximately 40% of the time. Travelers who plan to visit developing countries should take a number of preventive measures, including getting relevant vaccines. Some vaccines, such as the yellow fever vaccine, are mandated for country entry as determined by the World Health Organization. Other vaccine-preventable diseases, such as typhoid fever, have known country-specific risks, such as travel to the Indian subcontinent, but are often not given, resulting in numerous preventable cases of the disease.25 It is estimated that only about 14% and 11% of travelers receive the hepatitis A and tetanus vaccines, respectively, before departure to a developing country.26 Although these low immunization rates stem in large part from lack of awareness of risk by travelers, they may also be related to primary care clinician recommendations. When compared with primary care clinicians, pharmacists may provide more consistent and accurate recommendations for travel vaccines.27
The results of our multivariate model show that patients accessing vaccinations during off-clinic hours were more likely to be aged younger than 65 years. Patients aged younger than 18 years used off-clinic hours for vaccination more than any other age-group in the study (Table 2). According to the CDC, influenza vaccination rates are low for people aged 13 to 17 years (34.5%) and 18 to 49 years (29.9%) compared with those aged 65 years and older (69.6%).5 With the low rates of adult and adolescent vaccination in the United States, community pharmacies are creating new opportunities for vaccination that may help the country achieve the Healthy People 2020 vaccination goals.28 A study conducted in rural West Virginia suggested that convenience was the primary determining factor in mothers’ decisions to take their children to pharmacies for vaccinations.29 Expanded hours and access to vaccination for patients aged younger than 18 years may ultimately prevent students from missing school because of illness or because of the need to visit a physician’s office during school hours.
Results show that pharmacists are also vaccinating patients aged 65 years and older, who are at higher risk for health complications from vaccine-preventable diseases such as influenza, pneumonia, and herpes zoster. In our sample, approximately 46% of patients fell into this age-group, with a higher proportion receiving vaccination during traditional clinic hours. This finding may also just represent a population more likely to be retired who already normally access medical care during the day. Using only prescription profiles, pharmacists previously demonstrated their ability to target high-risk populations for pneumococcal vaccine.30 Interestingly, for the 40% of our patients with at least 1 inferred chronic condition, the frequency did not differ greatly whether they were vaccinated during traditional or off-clinic hours, suggesting patients with or without chronic diseases use nontraditional hours for vaccination in a similar manner. A previous study indicated that pharmacists were successful at identifying at-risk patients and providing additional immunization services.30 Of patients receiving influenza vaccinations at a community pharmacy, 4.9% who were also at risk for invasive pneumococcal disease received the vaccination per pharmacist recommendations during the study period. In this study, this rate was higher than a benchmark uptake rate of 2.9%, a rate typically seen at physicians’ offices.30
In our sample, 94% of all vaccinations were provided in a metropolitan or micropolitan setting, which most likely reflects the greater availability of pharmacies and those open during off-clinic hours in urban areas. Not all people in urban areas have equal access to health care services, which is an element of the Health Resources and Services Administration definition of a Medically Underserved Area (MUA). A previous study found that 43% of the US population resides within an MUA, and Walgreens pharmacies served nearly one-half of this population; nationwide, nearly one-third of influenza vaccinations were administered by pharmacies located in MUAs.13
Unfortunately, pharmacists’ ability to fully enhance vaccination rates is limited by a patchwork of state laws that allow either unrestricted authority to administer vaccines or a variety of restrictions. For example, 41 states/territories allow pharmacists to give any vaccine, but 17 restrict pharmacist administration to patients aged 18 years and older. All 50 states, the District of Columbia, and Puerto Rico now at least allow pharmacists to administer influenza vaccinations to all adults aged 18 years or older, however. A 2004 study showed that as more states allowed pharmacists to vaccinate, the immunization rates for those states were higher than the rates in states that did not allow this practice, suggesting pharmacists were not just shifting patient populations from medical clinics, but identifying new populations.31 In our study, patients residing in states that authorized pharmacists to administer all CDC-recommended vaccinations were more likely to use off-clinic hours. If states expand pharmacist immunization privileges, patient access and coverage may increase. A previous study estimated that if states were granted full immunization privileges, there would be a 148% increase in pneumococcal vaccination and a 77% increase in herpes zoster vaccination.32
In our study, there was no significant difference in the use of off-clinic hours for patients only receiving a vaccination vs patients also picking up a prescription. Overall, a relatively small proportion of patients (13.1%) picked up a prescription medication at the vaccination visit. This pattern may be due to a relatively better overall health status of patients receiving vaccinations and thus a lack of a need to fill any prescriptions, or due to patients seeking immunization services from a pharmacy independent of prescription services. The CDC reports that persons whose last physician’s visit for a routine checkup was at least 1 year ago were more likely to receive vaccinations in a nonmedical setting than those whose last physician’s visit for a routine checkup was more recent (53.5% vs 38.8%), suggesting that the availability of influenza vaccination in nonmedical settings can complement health care professional efforts by reaching populations less likely to be seen by clinicians.8
Few studies have demonstrated this type of off-clinic hours access made possible by community pharmacies. One study analyzing retail clinics found that from 2007 to 2009, 44.4% of all visits (including nonimmunization visits) were on the weekend or during weekday hours when physician offices are typically closed.33 Previous studies have also indicated that patients trust the pharmacist to administer immunizations and value the ease of access.34 Our study builds on the model of pharmacy-based immunization access by exploring patient use of the times pharmacists are available to vaccinate, patient demographics, and pharmacy use.
Limitations
This study involved only a single pharmacy chain; however, a survey of multiple chain pharmacies indicated that many have also expanded hours and vaccine offerings.35 As this was a retrospective pharmacy immunization record review, we could only speculate why patients chose to be vaccinated when they did. According to the previous studies, convenience is likely the greatest driver of use of pharmacy-based immunizations.7,29 Second, we used a time period to serve as a proxy for traditional clinic hours, but we did not have data on clinics that might have had expanded hours. Prescription data were used exclusively to infer the presence of a chronic condition in vaccinees, but patients may have received their medications for chronic conditions from a different pharmacy, potentially underestimating the rate of comorbid illnesses; however, when patients seek vaccination, pharmacists use a standardized screening tool that can determine presence of medical conditions. The data we used did not include patient race, which has been demonstrated to be a driver of vaccination uptake.8
Implications
The typical individual who accesses immunization services during off-clinic hours is male, younger, and healthier, and resides in an urban area. When immunization access is expanded, patients will seek and receive vaccinations at a time that is most convenient to them, often when medical clinics are closed. Although those older than 65 years of age continue to represent the largest segment receiving vaccinations in the pharmacy, younger working-aged patients may be more likely to receive vaccinations during off-clinic hours. Expanding the ability of pharmacists to administer all vaccines to adolescents and adults in all states without a physician prescription, coupled with expanded hours of operation, is likely to have the greatest impact on pharmacy-based immunization rates.
Acknowledgments
The authors acknowledge Zhongwen Huang, MS, for his data management support and the more than 26,000 pharmacists who provided vaccinations to the study population.
Footnotes
-
Conflicts of interest: Dr Taitel, Mr Fensterheim, and Mr Cannon are employees of Walgreen Co. Dr Goad serves on the speaker’s bureau for Merck and Co, Inc.
-
Funding support: Financial support for this study was provided entirely by Walgreen Co.
- Received for publication September 7, 2012.
- Revision received December 28, 2012.
- Accepted for publication January 31, 2013.
- © 2013 Annals of Family Medicine, Inc.
References




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- "Vaccination needs to be easy for the people, right ?": a qualitative study of the roles of physicians and pharmacists regarding vaccination in Switzerland
- Pharmacists: Vaccine Heroes Among Non-physician Providers
- Primary care: Practice meets technology
- Evaluation of the first pharmacist-administered vaccinations in Western Australia: a mixed-methods study
- National community pharmacy NHS influenza vaccination service in Wales: a primary care mixed methods study
- Seasonal influenza vaccination delivery through community pharmacists in England: evaluation of the London pilot
- Defining and advancing ambulatory care pharmacy practice: It is time to lengthen our stride
- Pharmacists And Technicians Can Enhance Patient Care Even More Once National Policies, Practices, And Priorities Are Aligned
- In This Issue: Mindfulness in Practice and Policy