
Abstract
PURPOSE We sought to compare and contrast patterns of change toward patient-centered medical homes (PCMHs) in 5 New Orleans primary care safety net clinics in the aftermath of Hurricane Katrina. We assessed the general direction of change in practice to discover possible reasons for differences in patterns of change, and to identify impediments to change.
METHODS Data collection consisted of 5 semiannual telephone interviews with clinic leadership over 2.5 years supplemented by administrative audits. We used standard survey indexes of PCMH to monitor practice change. We conducted site visits and unstructured in-person interviews with clinicians and staff of the 5 clinics.
RESULTS PCMH index scores improved during the observation period with variations in rates of change and initial levels of PCMH. Qualitative analysis suggested possible explanations for this differential success: (1) early vs later starts in practice change, (2) funding based on patient outcomes, (3) demands that compete with practice change, (4) qualities of clinic leadership, and (5) relations with the communities where patients live. Barriers to practice change included high demand for services, deficient linkages between hospital and specialty care, lack of staff resources, and a need to focus on clinic finances.
CONCLUSIONS The PCMH model can successfully address the needs of safety net populations. Stable leadership committed to serving safety net patients via the PCMH model is important for successful practice transformation. Beyond clinic walls, cultivating deep ties to the communities that clinics serve also supports the PCMH model.
- organizational change
- patient-centered medical home
- primary care
- safety nets
- practice-based research
- vulnerable populations
INTRODUCTION
The patient-centered medical home (PCMH) model is a promising one for improving quality and efficiency in primary care clinics that target safety net patients—patients who because of poverty and unemployment are uninsured or reliant on public insurance streams such as Medicaid. We sought to fill gaps in understanding how PCMH-driven health reforms could better quality, accessibility, and continuity of care for such patients.1–7
Post–Hurricane Katrina New Orleans is a model for transformation of primary care safety net health systems envisioned by federal health reform.8 The Affordable Care Act created Federally Qualified Health Center (FQHC) Advanced Primary Care Practice Demonstration projects,9 with a budget of approximately $42 million for road testing new models for delivering care. A new approach to safety net care in New Orleans, necessitated by Katrina’s devastation, provides a unique window into the real world of health reform, with important lessons that augment what can be learned from the national FQHC demonstration project. The chronology and details of major events in this process are given in Supplemental Appendix 1, available online at http://annfammed.org/content/11/Suppl_1/S60/suppl/DC1.
In 2008, the federal government provided $100 million to the state of Louisiana, via the Louisiana Public Health Institute, for support of 25 multisite health care delivery systems providing primary care and behavioral health services to safety net patients throughout the Greater New Orleans Area (NOLA).10* Thirty-nine nonprofit clinics (located in predominantly poor areas) received federal grant funding to enhance patient access, along with financial incentives for obtaining PCMH recognition from the National Committee for Quality Assurance (NCQA) by December 2009.12 Most clinics evolved by adopting “niche strategies” responsive to uncertainties in funding streams and changes in public policies that have long characterized the environment of safety net care.13,14 The varied implementation strategies by which they achieved recognition as medical homes can demonstrate how meaningful health reform can be achieved despite the challenging circumstances faced by most safety net providers.
METHODS
In 2007, our research team received a grant from the Commonwealth Fund to evaluate the progress of NOLA clinics as they pursued practice reforms and formal NCQA recognition as medical homes, with the aid of federal grant recovery funds under the Primary Care Access and Stabilization Grant.8 As a part of that evaluation, we conducted semiannual survey telephone interviews with clinic leaders. These interviews were supplemented with routine administrative data on each clinic collected semiannually by the Louisiana Public Health Institute staff at approximately the same time.
We collected additional data in periodic site visits to observe clinic operations and conduct informal interviews with clinic leaders, staff, and patients in 5 clinics that had successfully made changes in practice consistent with the PCMH model. For these 5, we combined data from the evaluation study’s phone interviews and administrative audits with qualitative data from site visits to address 3 questions about trajectories of PCMH implementation: (1) Did the 5 clinics implement and maintain key elements of the PCMH model in caring for safety net patients? (2) What factors explain variations in the consistency and success of PCMH implementation across the 5 clinics? (3) What challenges did the 5 clinics experience in transforming their practices in accordance with the PCMH model?
Data Sources
Data From Periodic Structured Interviews
As a part of our evaluation study, every 6 months from June 2008 to June 2010, leaders of the 5 clinics (4 physicians and 1 nurse practitioner) were interviewed by telephone for about 45 to 60 minutes using a protocol adapted from the National Study of Small and Medium Physician Practices and the NCQA Physician Practice Connection Patient-Centered Medical Home survey tools.15,16 Respondents had principal responsibility for clinic operations and were knowledgeable about care processes and quality improvement efforts at the clinics they led. If we identified inconsistencies in responses over time (eg, interviewee stated the clinic had a registry for diabetic patients initially and then subsequently reported no such registry), the primary author (D.R.R.) conducted an additional 1-hour interview with each clinic leader to validate responses. This process clarified the reasons for reversals in trends (real changes or mistaken responses), and when mistakes were identified, we corrected the data.
Qualitative Data
We made 3 rounds of half-day site visits to each clinic. In addition to direct observation of daily clinic life, we conducted audio-taped, semistructured individual and group interviews with clinic staff that included persons in charge of clinical and financial operations (clinic managers, medical directors, chief executive officers, chief financial officers), clinicians (staff physicians, nurse practitioners, social workers, and care managers), and support staff in charge of reception, billing, scheduling, and data management. A total of 64 semistructured interviews with 52 clinic staff were conducted during 3 site visits between July 2010 and January 2012. Interview foci included (1) a brief overview of practice history and experience post Katrina, (2) leadership’s strategic vision for practice transformation, (3) official policies, practices, and directives issued to pursue those goals, (4) an evaluation of resources for achieving this vision, (5) internal and external barriers to implementing change, (6) strategies used to overcome those barriers, and (7) specific events, people, or both that shaped the practice’s chances of success. All interviews were professionally transcribed.
Data Analysis
Quantitative analysis drew on data from the 5 semiannual waves of surveys, conducted over a 2.5-year observation period. We constructed survey indices to gauge the progress of PCMH implementation, focusing on 3 of the 7 components of the PCMH model deemed most relevant to safety net care: enhanced patient access, coordination and integration of care, and emphasis on quality and safety.17 Consistent with prior research,15,18 each clinic was assigned 1 point per domain if it passed a minimum threshold. Table 1 shows the domains defining each of the 3 components measured. Points were summed to create an index score for each of 3 medical home components separately: access, coordination, and quality/safety of care. We also created an overall “medical home” index by summing all points on the 3 above-mentioned indices. Scores on each index were standardized to provide a distribution ranging from 0 to 100, with higher index values indicating higher degrees of implementing PCMH processes. Baseline PCMH score was measured in June 2008, with 4 waves of follow-up every 6 months thereafter. Standardized scores were plotted by time of measurement for each of the 5 clinics to compare trajectories of change.
Patient-Centered Medical Home Indices
Qualitative data were analyzed using the method of constant comparison,19 allowing us to compare changes in the 5 clinic cases at each stage of data collection, and then to follow up on important observations, framed as research questions, in later iterations of the process. As data analyses and findings accumulated over time, our research questions changed to reflect new insights and accumulation of increasingly detailed information. As coding and analysis progressed, we wrote memos summarizing in-progress findings. To facilitate our analysis, we maintained a shared, searchable qualitative database of coded interview transcripts, field notes from site visits, and analytic memos. We discussed analytic themes emerging in weekly team meetings to find areas of agreement or disagreement, referring back to original interview transcripts to confirm results, compare clinics, and reach a consensus on interpretation whenever possible.
RESULTS
Clinic Characteristics
Table 2 provides an overview of the organizational characteristics of the 5 clinics at baseline, in June 2008, derived from administrative audit data. The clinics varied with respect to ownership type (faith-based organizations, independent nonprofits, and university-based practices affiliated with medical schools), FQHC status, and organizational size (in terms of numbers of patients and clinicians) as well as most frequent presenting diagnoses in their patient populations. Patients of all 5 were predominately African American, low income, and without private or public health insurance coverage.
Baseline Organizational Characteristics of 5 Clinics in New Orleans
Trajectories of Implementing the PCMH Model
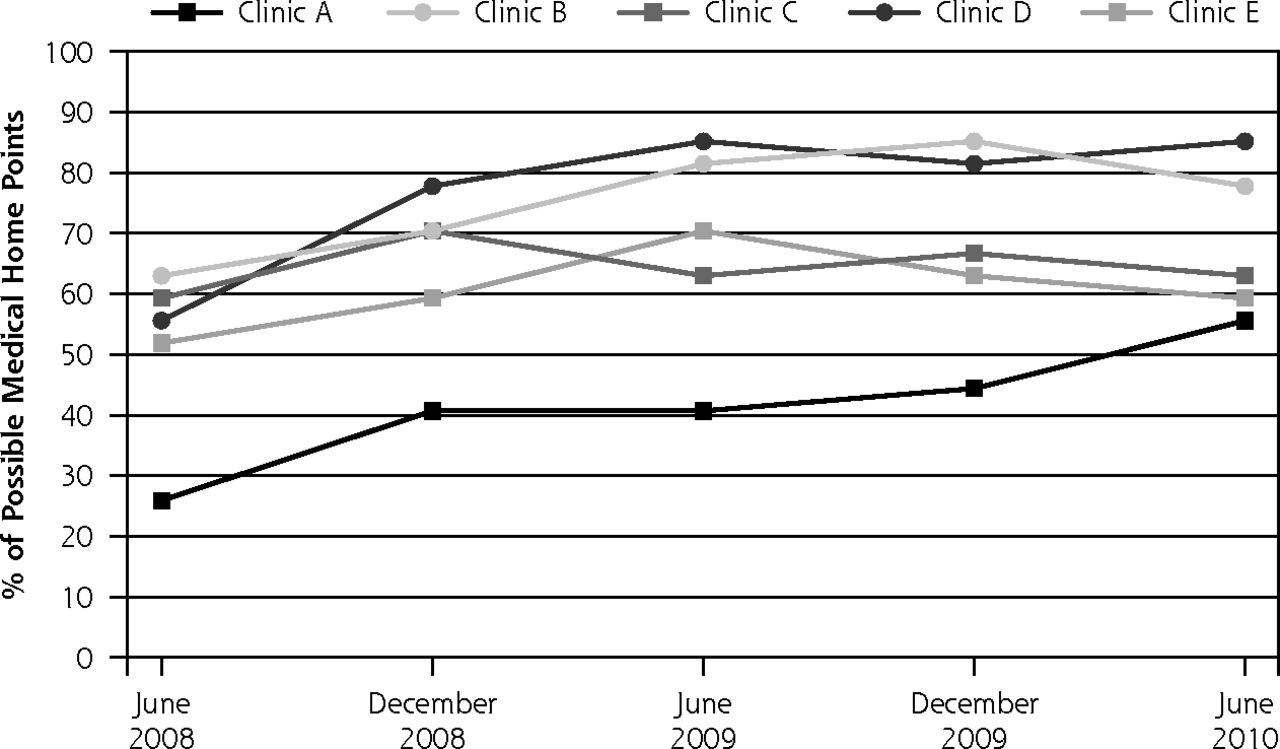
All 5 clinics studied showed improved or stable scores on PCMH indices over time and achieved relatively high levels of implementation. The time paths for achieving practice improvements varied considerably, however, falling into distinctive patterns that reflected substantial differences in degrees of success.
Trajectories of overall PCMH implementation fell into roughly 3 categories. Figure 1 shows that clinics B and D made steady, early improvement in PCMH reforms. Both started from relatively high baseline levels and maintained high scores over the 1.5 years covered by the last waves of data collection. In contrast, clinics C and E had roughly similar baseline levels on the overall PCMH score, and both generally remained at those baseline levels throughout the follow-up period. Clinic A shows a third trajectory, starting at a comparatively low level of baseline PCMH implementation, but progressing steadily upward until it matched the higher scores attained by C and E.
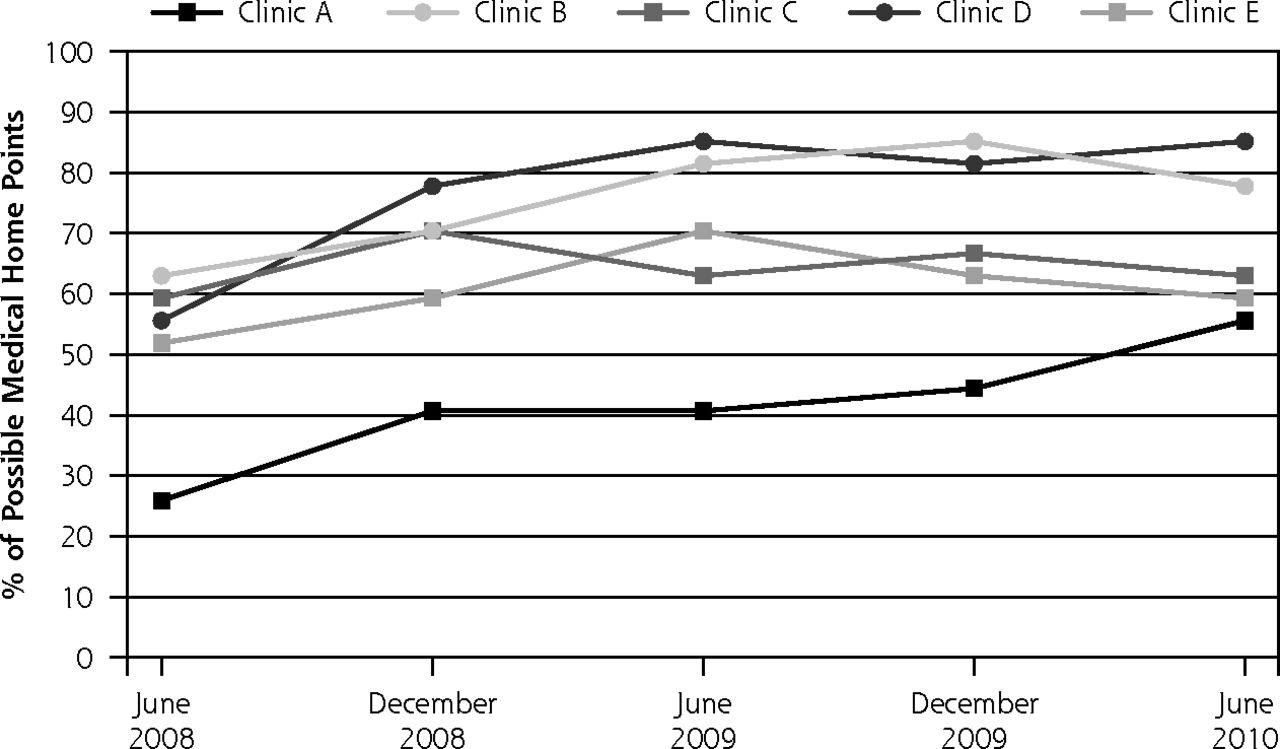
Use of medical home processes over time.
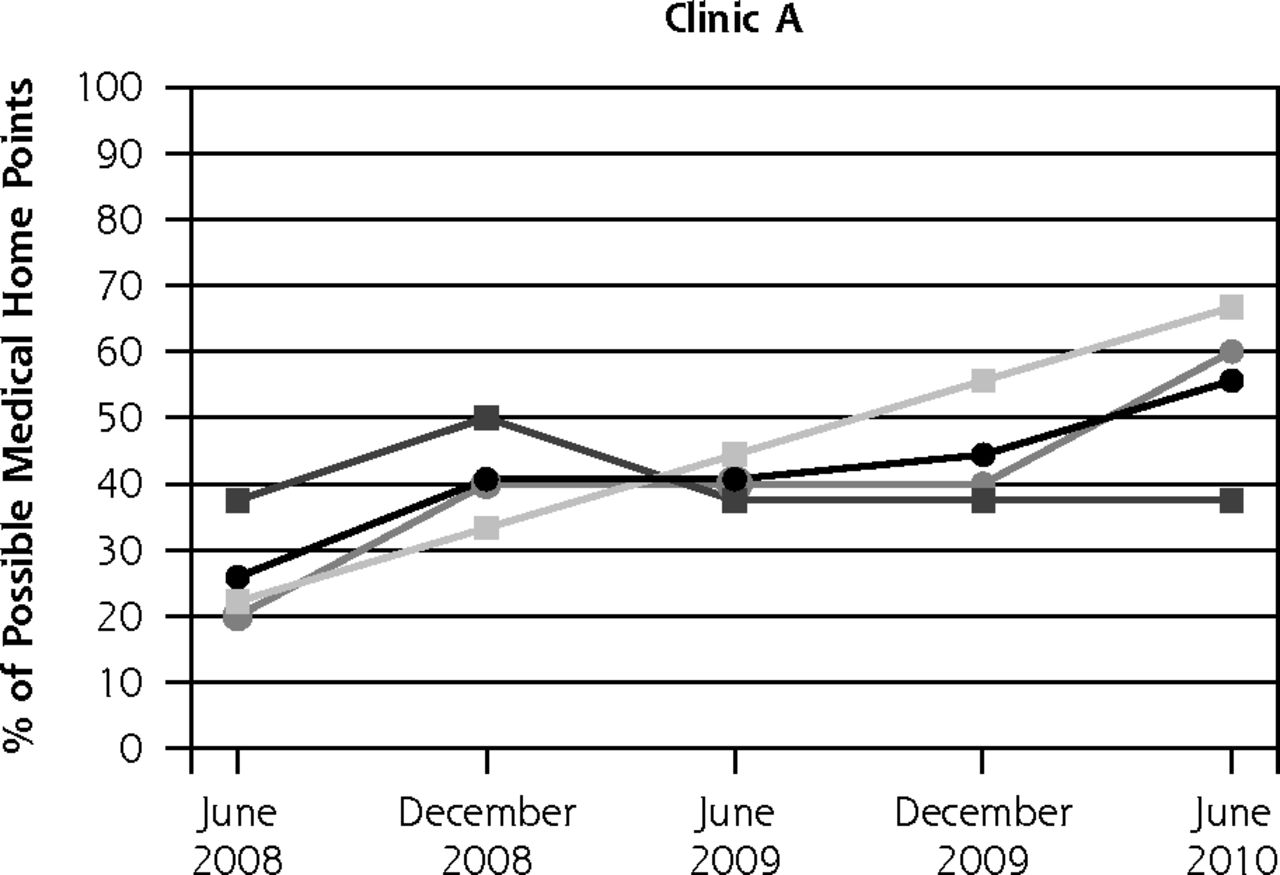
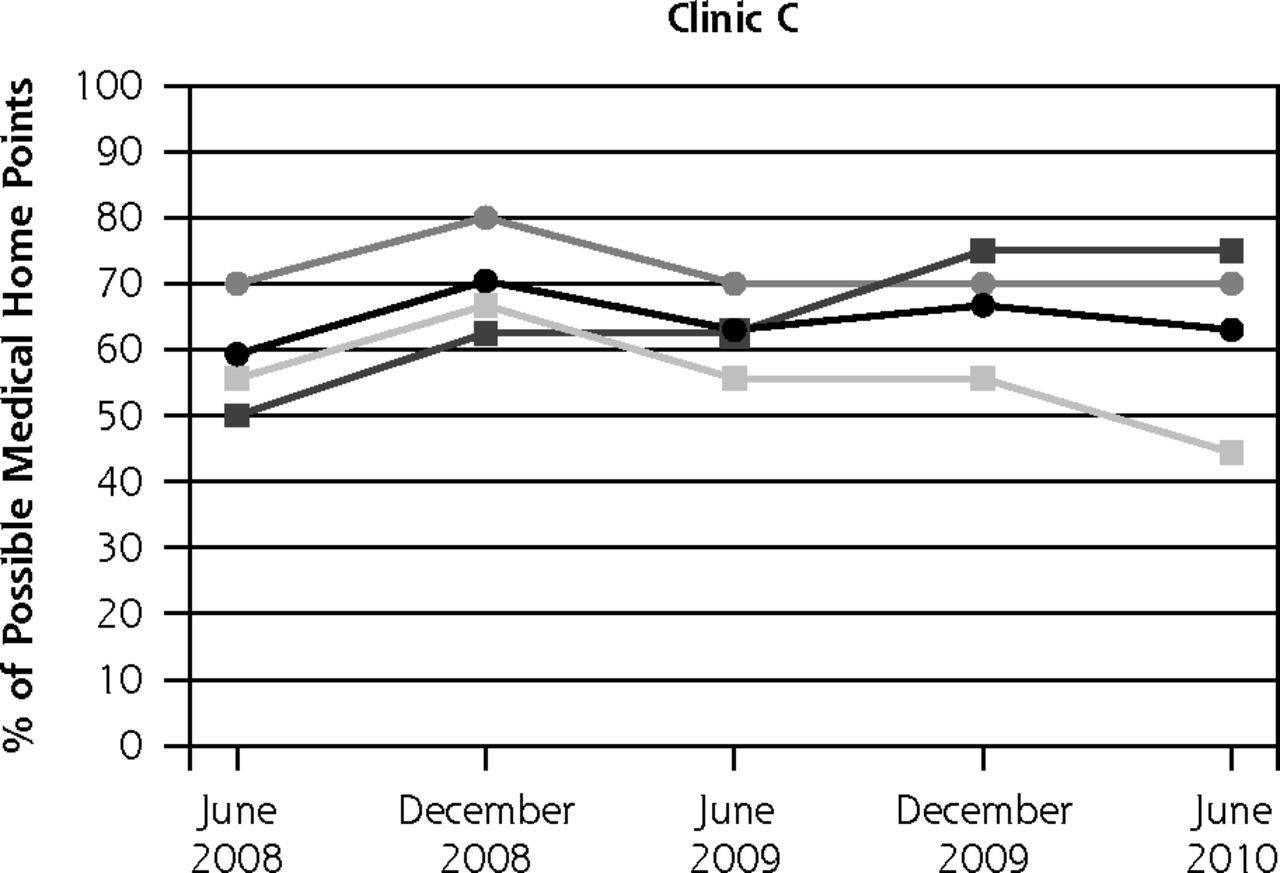
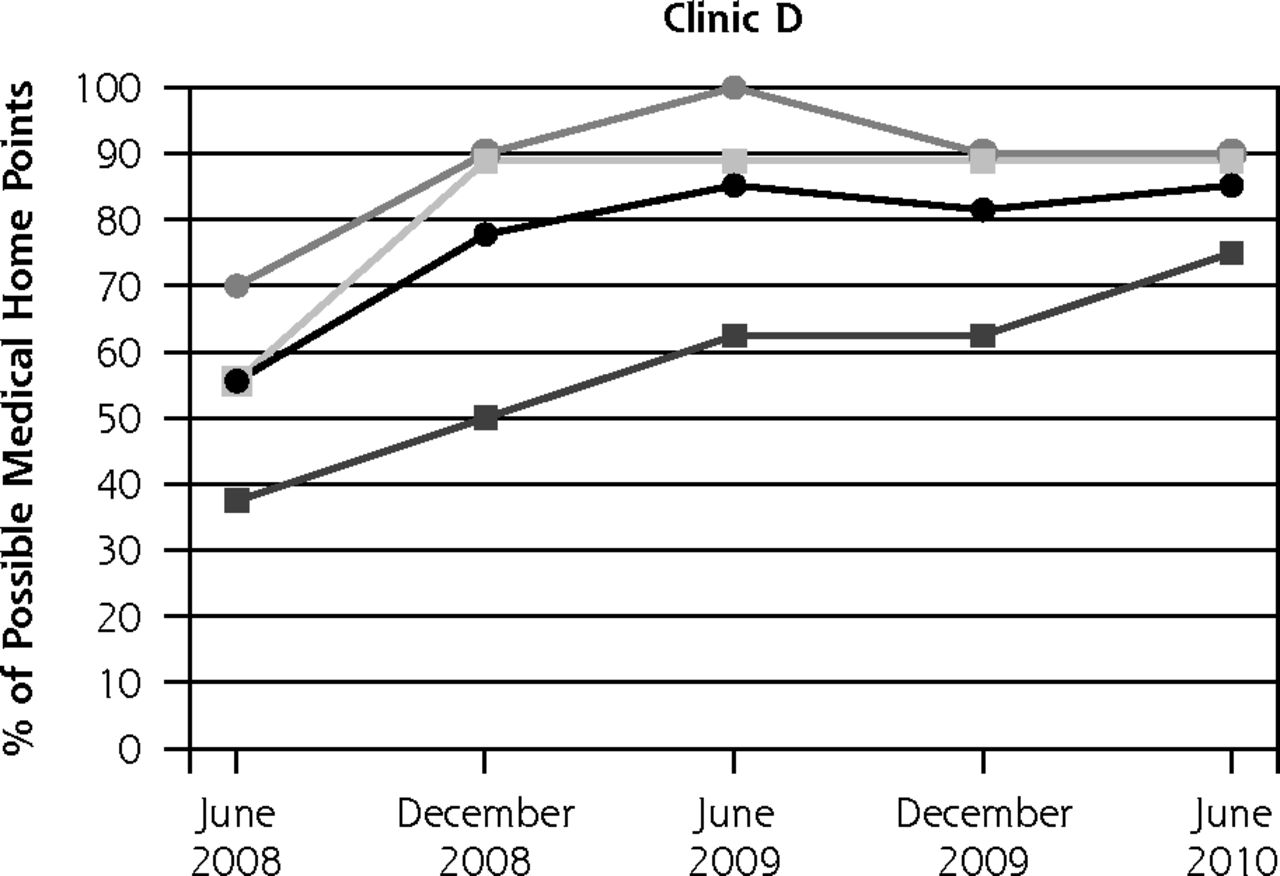
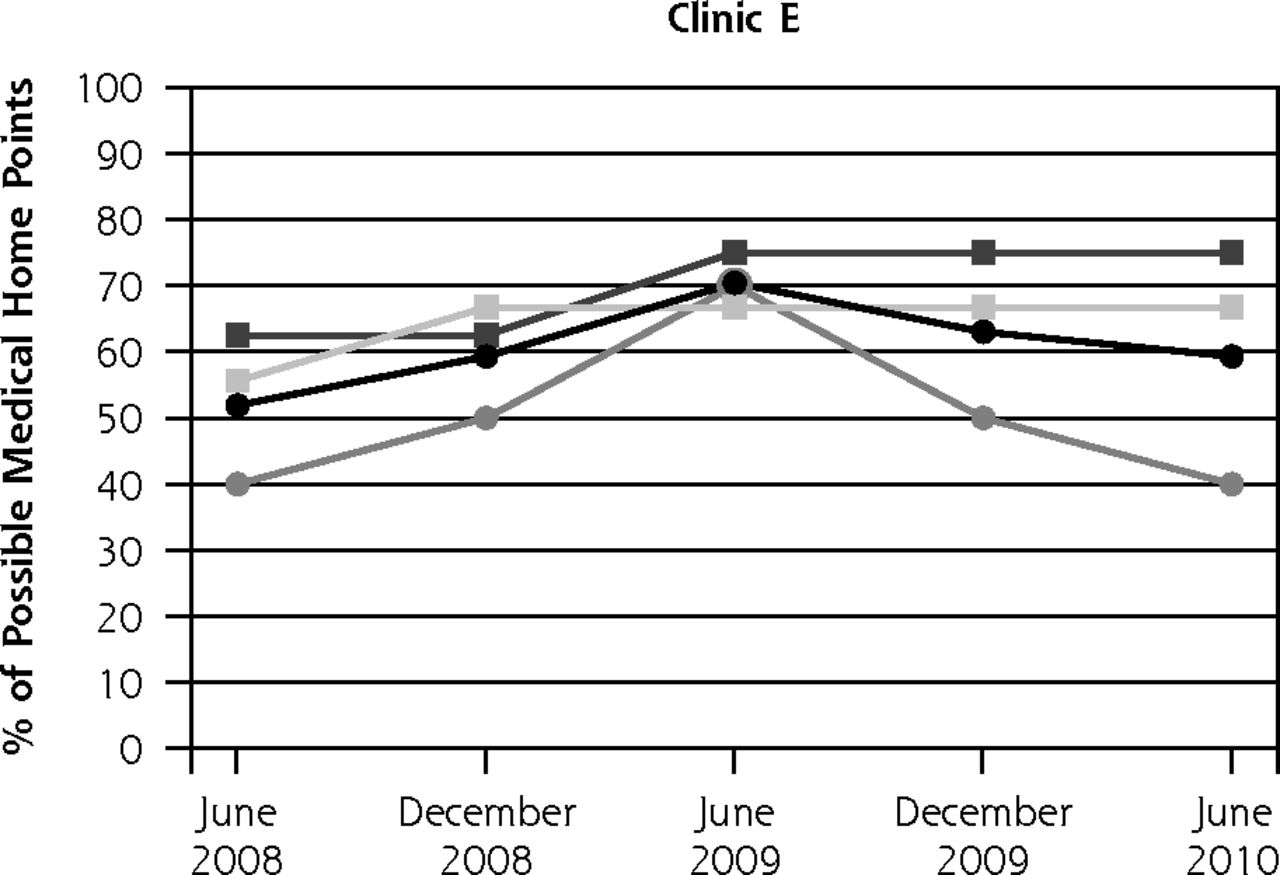
Figure 2 shows that time paths for implementing specific components of the PCMH model also varied across the 5 clinics in ways mirroring their overall trajectories. In clinics B and D, 2 of the 3 elements of the PCMH model—improved access and coordination of care—increased steadily to high values in roughly parallel fashion. Meanwhile, scores on quality and safety of care reached near-maximum values, but slightly declined toward the end of the observation period. In contrast, clinics C and E shared intermediate scores on access, coordination, and quality and safety at baseline. Both made steady gains in access over time. These 2 clinics made tandem gains initially, only to experience noteworthy declines later in the observation period (on quality and safety indices for E and care coordination for C). Finally, clinic A again pursued its own path: steady gains in coordination, and in quality and safety throughout, but low values, with minimal gains, in the accessibility of care.
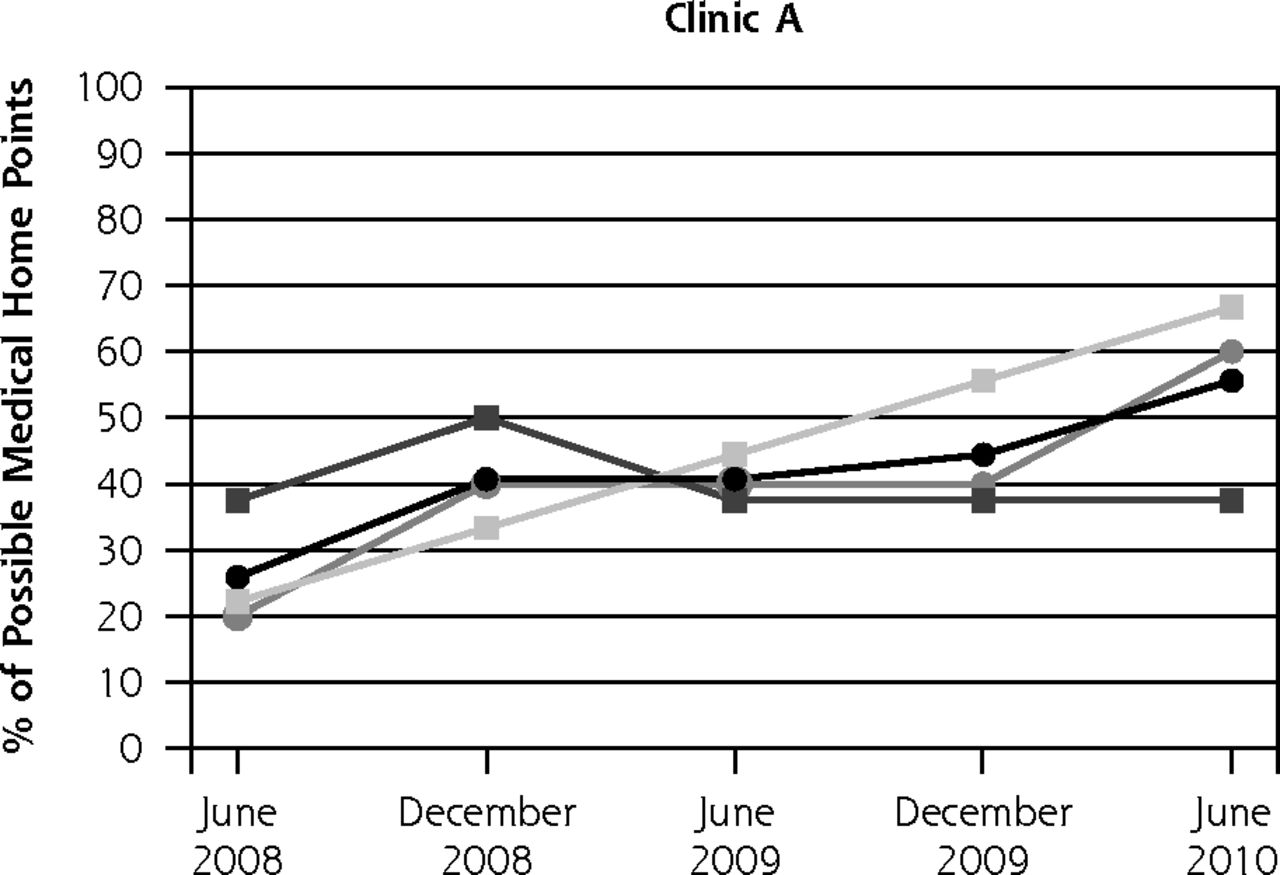

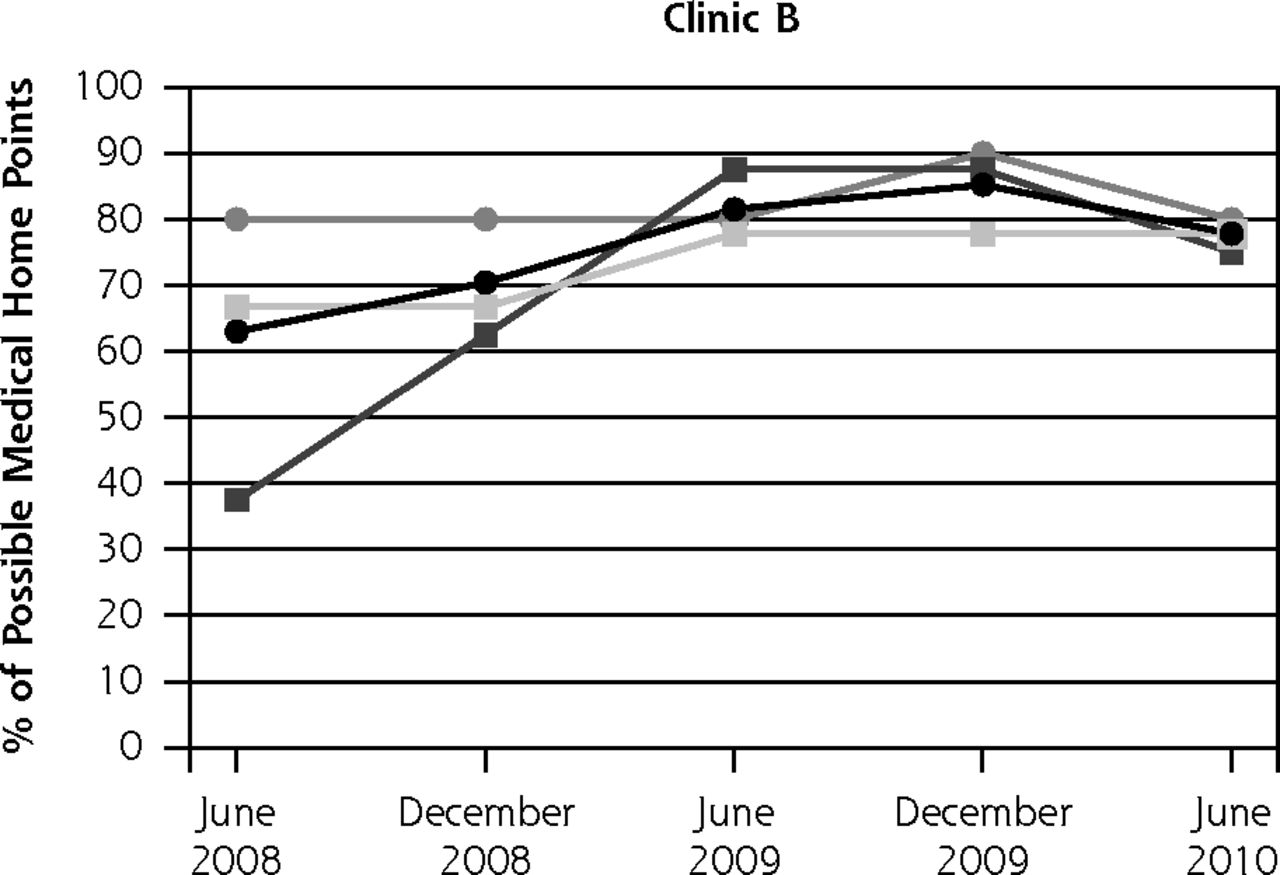


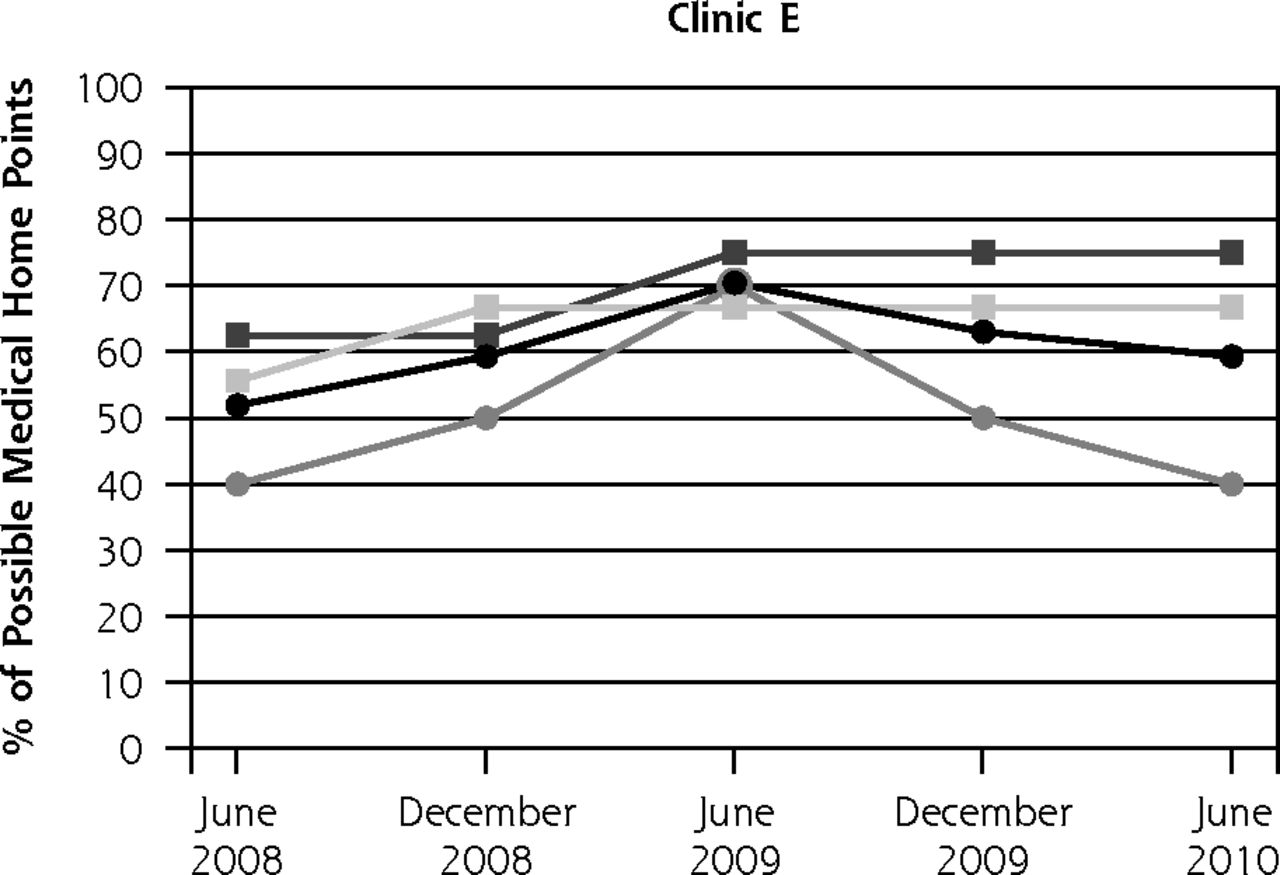
Trajectories of PCMH subindices in 5 clinics.
Explaining Variation Across Clinics
As noted above, all 5 clinics studied achieved relatively solid trajectories of positive change; however, clinics B and D exhibited relatively greater success overall and in specific indices of improved accessibility, coordination, and quality and safety of care. Qualitative data from direct observation and unstructured interviews with clinicians, staff, and patients provided some explanations for variations we observed in trajectories of change.
Early Adoption of PCMH-Like Innovations by Well-Positioned Practices
Before Katrina and the citywide push for medical homes, clinic B had already begun to implement practice changes based on the models of care that clinic leaders had learned from visiting quality improvement consultants and corporate philanthropists. Clinic B at baseline scored highest in overall in PCMH score, was the oldest clinic, and was the only FQHC affiliate—factors resulting in a “first mover” advantage. Clinic D shared a similar positive trajectory of change with B; in particular, it had been experimenting with mechanisms for increased access and linkages to specialty care through leadership connections with the health care consulting firm, the Institute for Healthcare Improvement.
Access to Supplementary Grants
After 2008, federal funding through the Primary Care Access and Stabilization Grant hurricane relief grant was a major factor driving PCMH transformations throughout NOLA.14 Still, the superior trajectories of change enjoyed by clinics B and D were linked to access to additional, more specialized funding streams that augmented those grants with flexible private funding to sustain clinic operations, help rebuild physical plants, and encouraged a focus on patient outcomes rather than simply increased numbers of patients served.
Ability to Balance Competing Priorities
All but 1 of the clinics served as a training site for physicians and future health professionals. Neither A nor D had particularly demanding training responsibilities, however, because they were not formally affiliated with a medical school. On the one hand, teaching clinics might have appeared to be advantaged by easy access to large numbers of medical residents; however, this resource came with the burden of teaching responsibilities, as well as rapid turnover in residents that could undercut goals for achieving stable patient access to a single, clearly identified primary care physician.
Positive Community Relations
Issues of trust arose quite naturally in relations between clinicians and safety net patients, particularly because NOLA’s poorest communities have historically lacked the ready access to primary care that more affluent populations take for granted. All 5 clinics studied took extraordinary steps to promote trust by creating friendly, open clinic environments. Clinics A and D, however, made establishing and maintaining trust with their patients’ communities central to their mission statements, and in clinic D’s case, this patient focus was a long-standing mission. Combating institutionalized racism was also a central theme in D’s efforts to establish relations of trust within its community.
Stability and Commitment of Clinic Leadership
Clinics B and D were both led by visionary medical directors who had long advocated for PCMH-like process improvements in the wider arena of primary care medicine. Both were well known and respected in the NOLA medical community, and as we observed, actively relied on their community leadership positions to advocate for their clinics, and negotiate with hospitals and specialty clinics for care needed by uninsured patients.
Recognizing the need for feedback on clinic experiences (from staff and patients) was a key ingredient of leadership in clinics with exceptional trajectories of change. So was recognition of the need for systematic data to support attempts at midcourse correction in efforts to transform primary care. Although all the clinics we studied trained their staffs in ways consistent with the PCMH model, B and D evidenced a sustained commitment to service improvement via ongoing cycles of quality improvement and systematic feedback on performance. Both did so with the aid of outside practice consultants who periodically observed process improvements, provided critical suggestions, and assisted in building data systems to monitor progress and make needed corrections.
Adapting to Common Constraints on PCMH Implementation in a Safety Net Context
Despite some differences observed between clinics, all 5 had measurable success at promoting PCMH improvements: each achieved NCQA recognition as a medical home. What is notable is that these improvements unfolded in a shared environment of limited resources, high patient demand, and unstable grant funding.
Unlimited Patient Demand
All clinics faced the challenge of providing unfettered primary care access to a large community of safety net patients, while at the same time improving quality and care coordination within the clinic.
Lack of Hospital or Specialty Care Involvement
All clinics experienced the lack of hospital and specialty care involvement as a major impediment to PCMH implementation. Clinics affiliated with medical schools had the advantage of closer alignment with the main public hospital. But they struggled with challenges commonly found in academic settings: bureaucratic hurdles, departmental politics, and underinvestment in primary care by the parent organizations. The FQHCs and medical school–affiliated clinics most successful in bridging the fragmented care systems to coordinate care were those able to devote staff time and resources to establishing and maintaining collegial relationships outside the clinic, and negotiating creative solutions that involved frequent communications via telephone calls, paging systems, fax machines, and requests for personal favors.
Sustaining Change
Although all clinics succeeded in implementing PCMH processes, they also universally faced difficulties in sustaining such changes over the study’s 2.5 years. Concern over the stability of funding in the face of uncertain grant support and insufficient coverage of uninsured patients was paramount and constant. In addition, an important element of success was the willingness of staff to dedicate ample time for meetings about changes the clinics were undergoing. Considerable resources were required to routinely examine measures of quality, provide useful feedback to clinicians, and discuss quality improvement. Ongoing staff training to take on new roles, routines, and responsibilities was another vital element of successfully sustaining PCMH clinical processes.
DISCUSSION
PCMH implementation occurred in 5 NOLA clinics serving safety net patients over the 2.5-year study period. Despite substantial differences, all faced similar challenges in implementing and sustaining PCMH changes: inadequate supply of well-trained staff dedicated to quality improvement; unstable funding; balancing comprehensive care management with maintaining unfettered access for new patients; lack of hospital and specialty care involvement; and service to safety net patients with multiple morbidities complicated by urgent personal and social needs. Medical school–affiliated clinics were also burdened by their primary mission to train future health professionals. How the 5 clinics met these challenges reflects differences in starting advantages, historical missions, and relationships to the communities they serve. But trajectories of change were also affected by capacities built and sustained from within each clinic: its leadership, capacities for strategic planning, and data measurement and reporting.
It has been argued that the PCMH ultimately should not be considered merely the sum of its component parts, but instead an integrated whole.20–22 The real-world clinics we studied, however, seemed to face a common set of challenging decisions forcing trade-offs that ultimately resulted in substantial variation across specific dimensions of primary care improvements. One trade-off, for example, was between improving access, and improving quality and coordination of care. Facing constrained resources and overwhelming service demand, safety net clinic employees perceived an ethical dilemma when forced to choose between unfettered access for all new patients, and limiting such access to better address the broader medical and social needs of their established patient population.
Our study methods and interpretations of the data we collected have limitations. Survey interviews with clinic leaders covered only 3 of the 7 components of the PCMH model. The other components—regular personal physician, multidisciplinary team care, whole-person orientation, and reformed payment to clinicians—were not surveyed, but did emerge as issues in clinician interviews done during site visits. Also, we relied entirely on semiannual interviews with clinic leaders to quantitatively track changes. These responses were essentially self-reports subject to errors ranging from misunderstanding questions to giving responses meant to “look good” to outsiders. To minimize the former, we trained interviewers before each interview cycle so that they knew what each question was addressing, how to clarify confusions, and how to probe with follow-up questions. To minimize “look good” responses, we tried to gain trust in face-to-face meetings and to emphasize that using their responses to measure PCMH was not part of a “horse race” with winners and losers. Validation interviews, done when we found inconsistent reports, tried to address both kinds of errors. Finally, the study context undoubtedly largely influenced the findings. We give our reflections on this context in Supplemental Appendix 2, available online at http://annfammed.org/content/11/Suppl_1/S60/suppl/DC1.
Our interpretation of differences between clinics is likewise subject to errors of attribution. Although the Primary Care Access and Stabilization Grant that responded to Katrina’s devastation created conditions akin to a “natural experiment,” it is not one that permits carefully controlled comparisons. To understand differences in trajectories of change, we relied on informants’ assessments of the importance of events as much as on our own. Although we believe that our interpretations are plausible, we cannot know what patterns of practice change would have occurred in the absence of factors (eg, fully committed clinic leadership and cultivation of strong ties with communities) that we argue encouraged successful transformations consistent with the PCMH model.
Acknowledgments
We are grateful for support by our New Orleans partners at the Louisiana Public Health Institute. Without the steadfast participation of the personnel of the 5 clinics, this study would not have been possible. We are grateful to the directors, clinicians, and clinic staff, who despite their heavy schedules, found time to meet with us. We owe special thanks to Leticia Wiley for editorial support and to Brandie Hollinger of the UCSF School of Nursing who provided support in coding and creating memos for qualitative data.
Footnotes
-
Conflicts of interest: authors report none.
-
↵* This grant was made under a provision of the Deficit Reduction Act of 2005 authorizing payments to restore access to health care in affected communities.11
-
Funding support: This research was funded by The Commonwealth Fund and the Agency for Healthcare Research and Quality, R18HS019139.
-
Disclaimer: The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.
- Received for publication June 18, 2012.
- Revision received January 14, 2013.
- Accepted for publication January 22, 2013.
- © 2013 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Recommendations for a Mixed Methods Approach to Evaluating the Patient-Centered Medical Home
- Patient-Centered Medical Homes In Louisiana Had Minimal Impact On Medicaid Population's Use Of Acute Care And Costs
- Challenges of Medical Home Transformation Reported by 118 Patient-Centered Medical Home (PCMH) Leaders