
Article Figures & Data
Figures
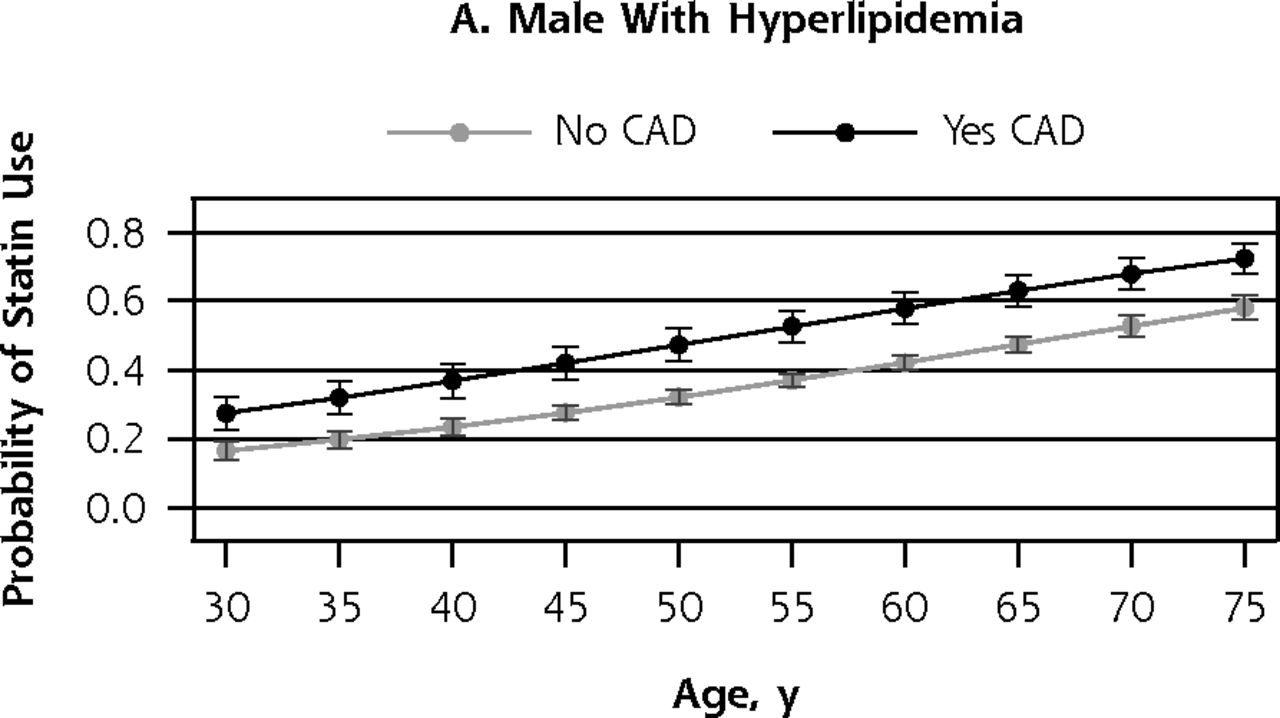
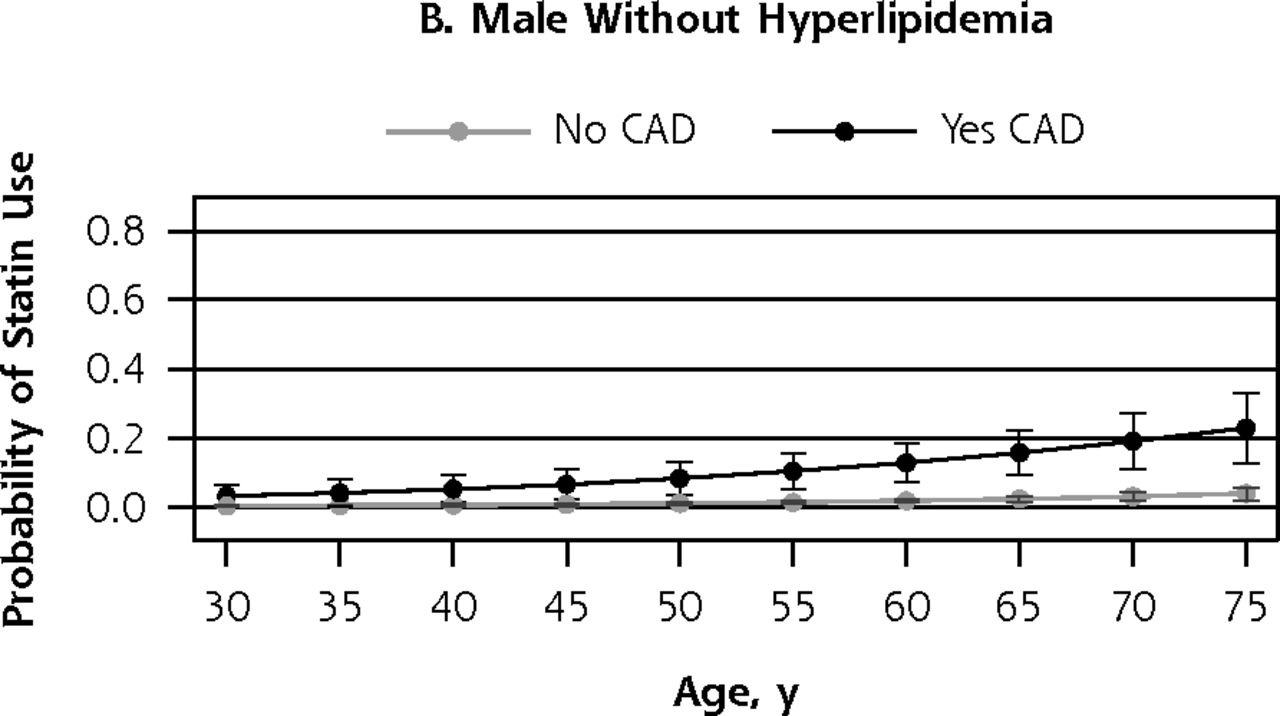
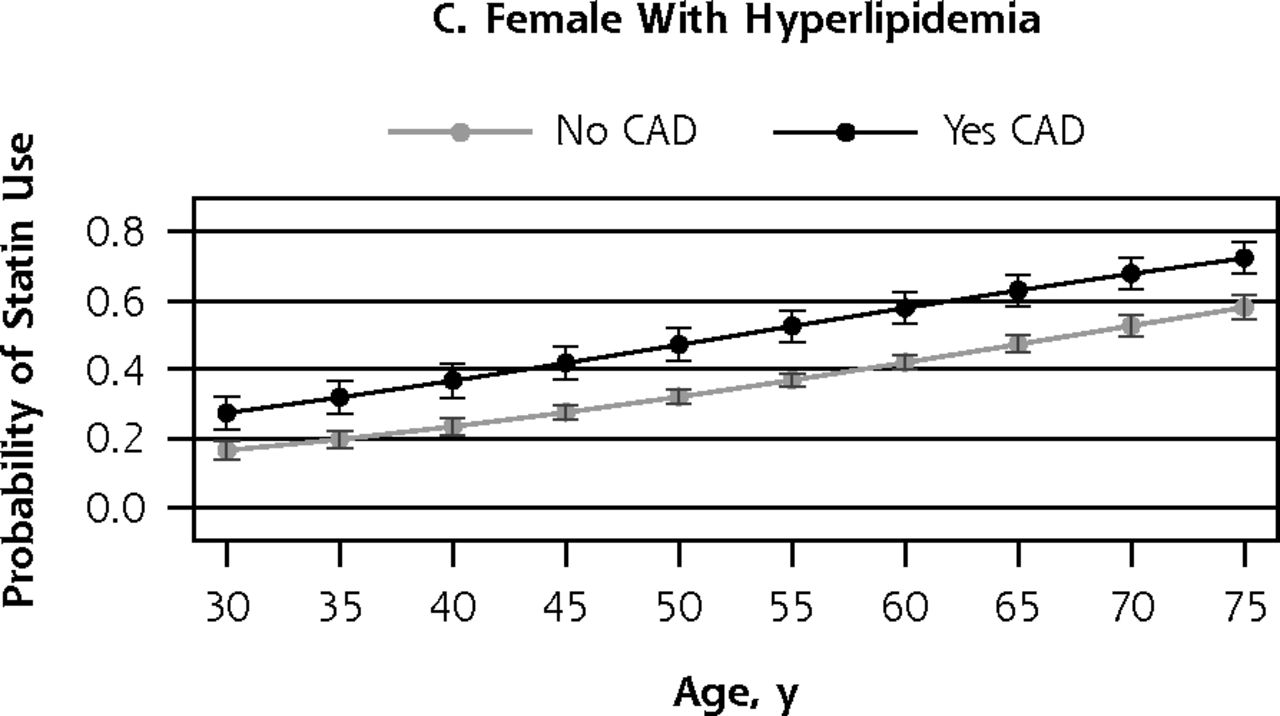
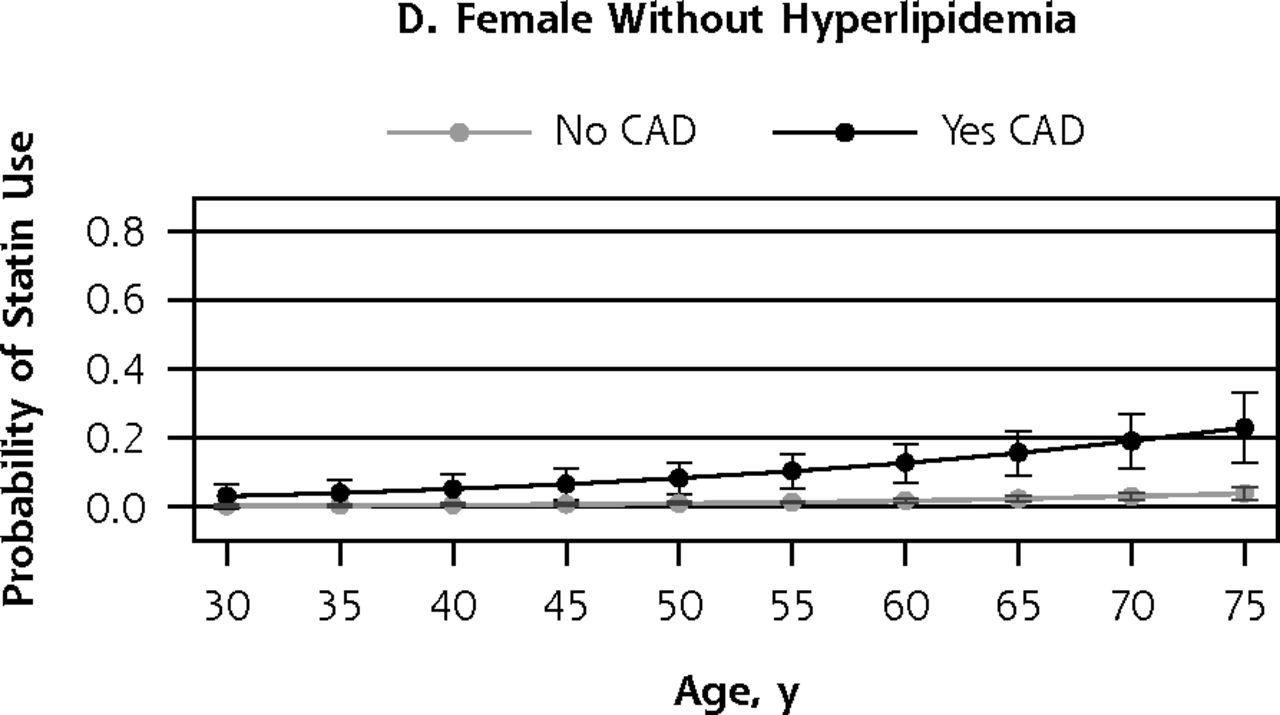
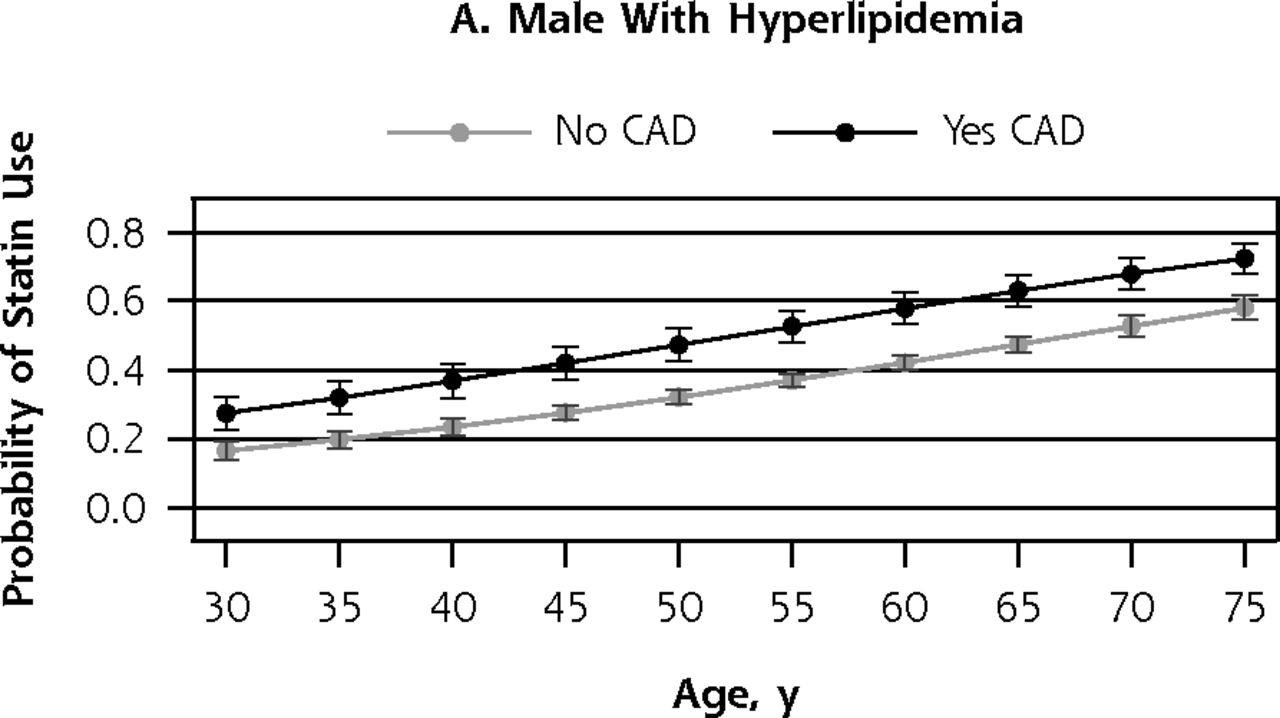
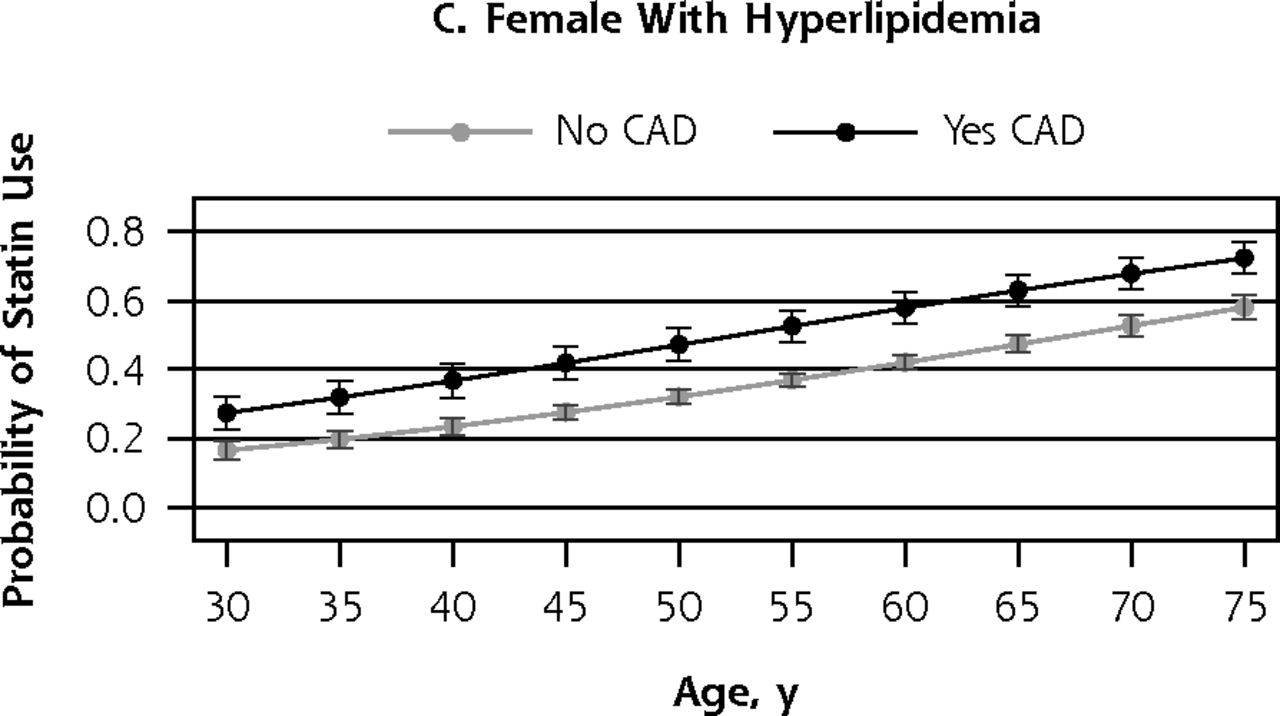
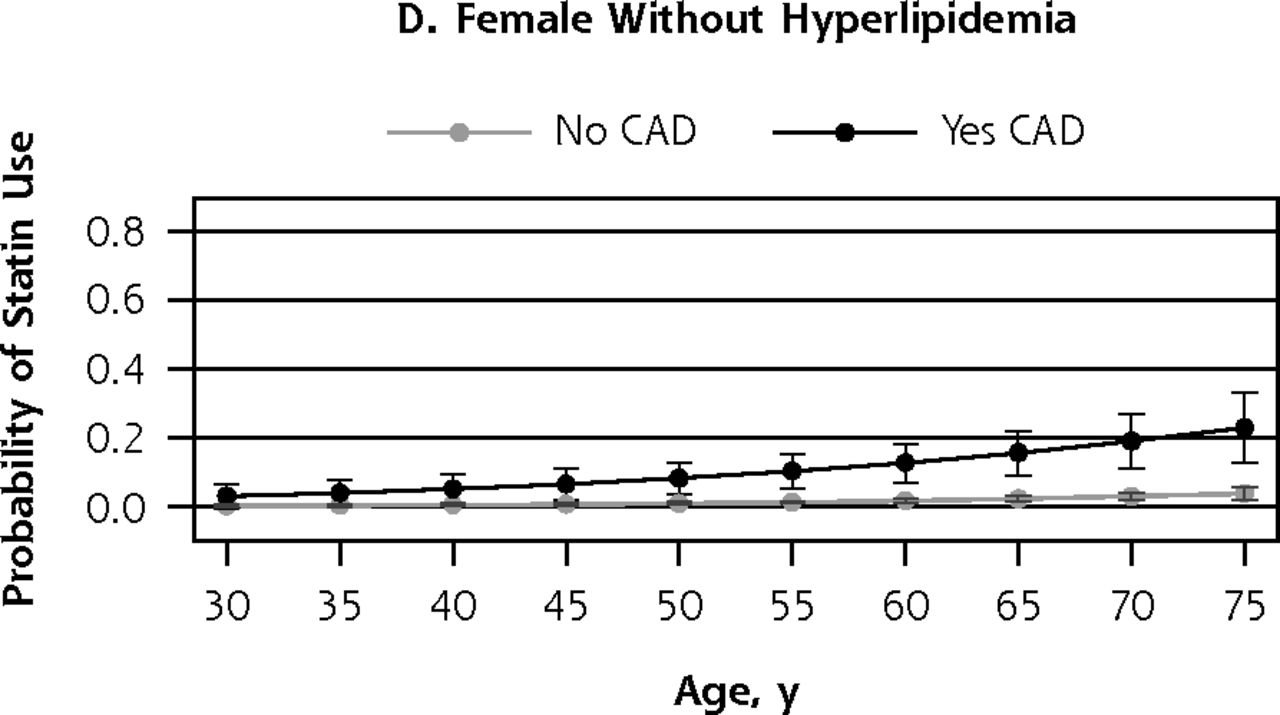
- Figure 1
Probability of statin use by presence of coronary artery disease, according to sex and presence of hyperlipidemia.
CAD = coronary artery disease.
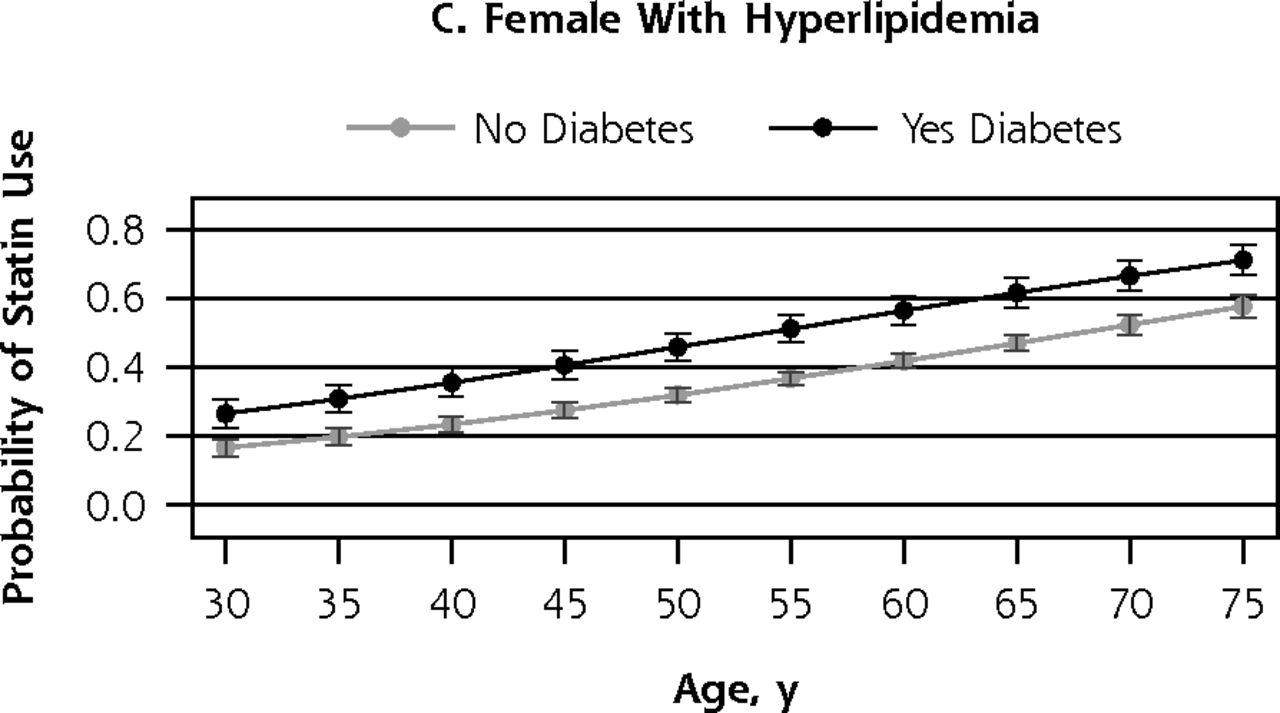
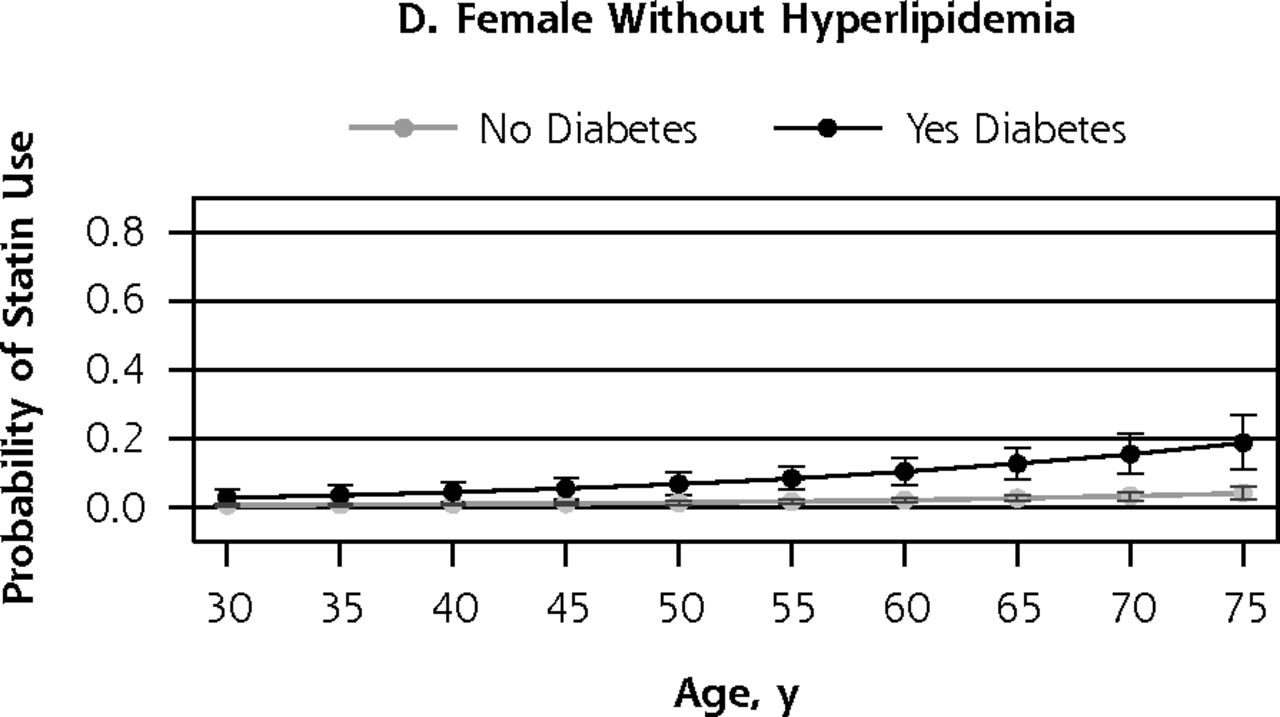
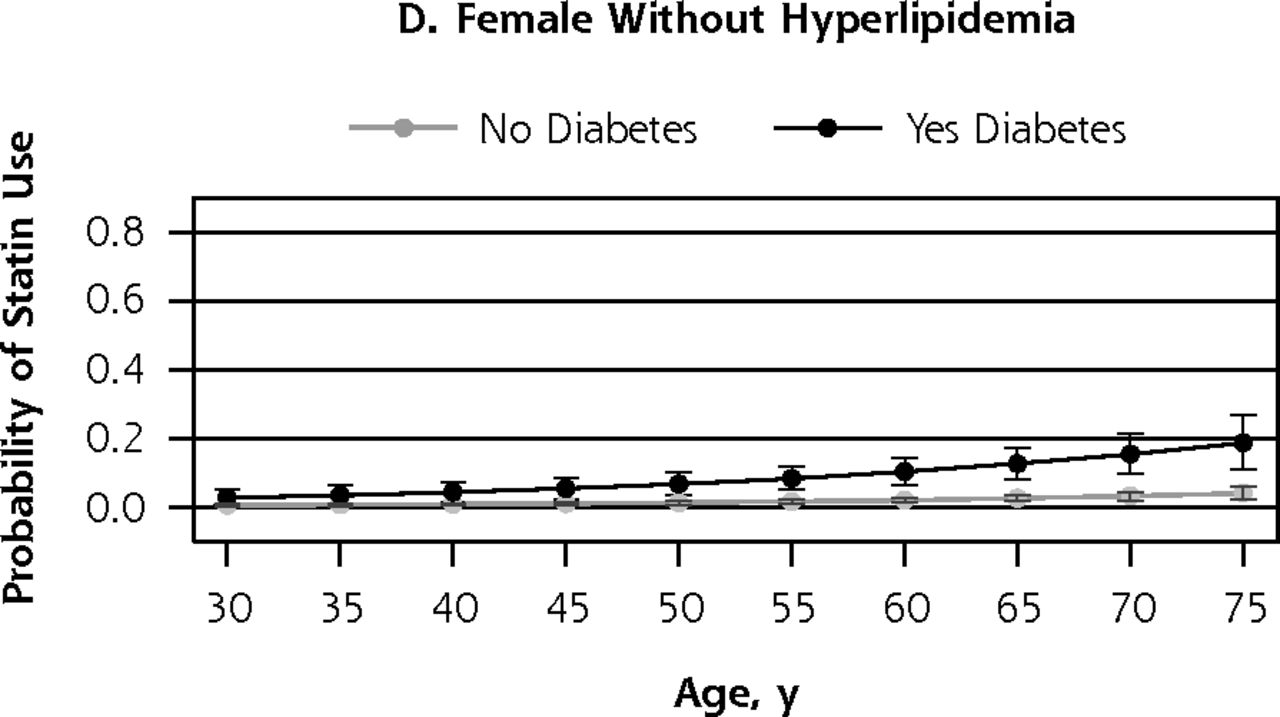
- Figure 2
Probability of statin use by presence of diabetes after age 40, according to sex and presence of hyperlipidemia.
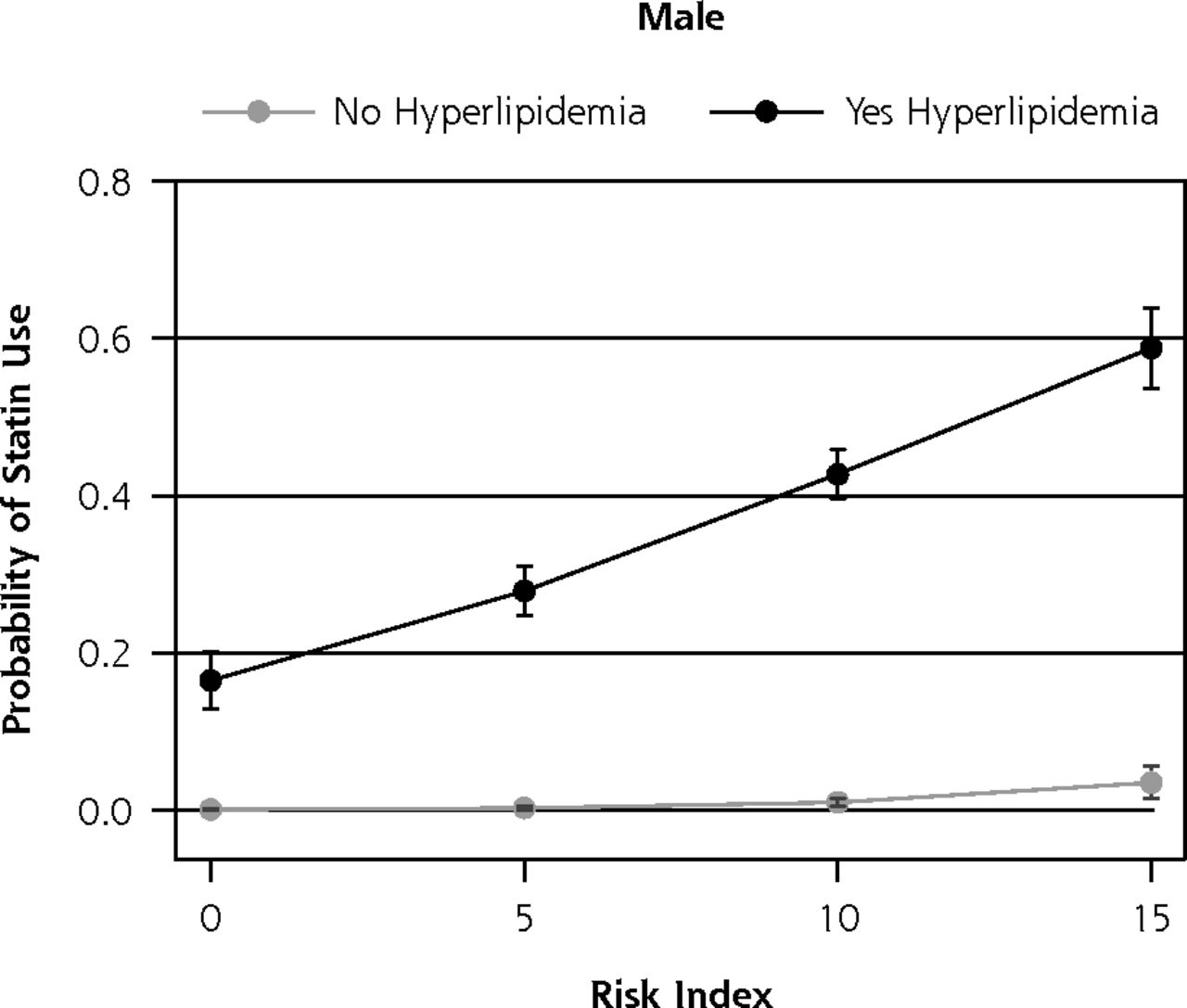
- Figure 3
Probability of statin use in an individual without diabetes or coronary artery disease by modified cardiovascular risk index, according to sex.



Tables
Characteristic Overall Sample Coronary Artery Disease Diabetes and Aged >40 Years Total On Statin Not on Statin Total On Statin Not on Statin Total On Statin Not on Statin Individuals, No. 16,712 2,799 13,913 1,304 694 608 2,016 992 1,019 Weighted proportion, % – 18.8
(18.0–19.7)81.2
(80.3–82.0)– 58.2
(54.6–61.7)41.8
(38.3–45.4)– 52.0
(49.4–54.6)48.0
(45.4–50.6)Population in millions, No. 166
(159–173)31.2
(29.2–33.2)135
(129–140)13.4
(12.3–14.5)7.8
(7.0–8.6)5.6
(4.9–6.3)18.7
(17.3–20.0)9.7
(8.9–10.6)9.0
(8.2–9.8)Age, y 51.3
(51.0–51.6)61.1
(60.6–61.6)a49.0
(48.7–49.3)a62.9
(62.3–63.6)64.9
(64.1–65.7)a60.2
(59.1–61.4)a60.3
(59.6–60.9)61.8
(61.1–62.6)a58.5
(57.6–59.4)aSex, female, % 50.8
(50.2–51.4)46.7
(44.8–48.7)b51.7
(50.9–52.5)b41.4
(38.4–44.5)37.8
(33.6–42.3)b46.4
(41.9–51.1)b49.3
(46.8–51.8)49.8
(46.0–53.6)48.8
(44.8–52.8)Tobacco users, % 18.6
(17.7–19.5)16.4
(14.8–18.2)b19.1
(18.1–20.1)b21.7
(18.5–25.3)19.7
(15.9–24.0)b24.7
(20.5–29.4)b17.0
(15.1–19.0)15.7
(13.4–18.4)18.3
(15.5–21.5)Hypertension, % 39.2
(38.1–40.3)70.7
(68.2–72.7)b31.9
(30.8–33.1)b80.3
(77.6–82.8)84.2
(80.6–87.4)b74.8
(70.7–78.5)b81.1
(78.8–83.1)86.0
(83.1–88.6)b75.7
(72.1–78.9)bHyperlipidemia, % 38.4
(37.5–39.3)95.8
(94.8–96.6)b25.1
(24.3–26.0)b78.7
(76.2–81.1)94.3
(92.0–96.0)b57.1
(52.7–61.4)b77.4
(75.0–79.5)94.8
(92.7–96.3)b58.5
(54.7–62.3)bRace/ethnicity, % White 69.5
(67.6–71.3)77.8
(76.0–80.3)b67.5
(65.5–69.5)b74.9
(71.8–77.7)80.3
(76.7–83.4)b67.3
(62.1–72.1)b62.8
(59.4–66.1)67.3
(63.3–71.0)b58.0
(53.3–62.5)bBlack 11.2
(10.1–12.5)9.4
(8.0–11.0)11.6
(10.4–13.0)11.5
(9.6–13.6)9.1
(6.9–12.1)14.8
(11.9–18.2)16.4
(14.0–19.0)14.4
(11.9–17.4)18.4
(15.2–21.5)Hispanic 12.8
(11.4–14.3)7.2
(6.1–8.5)14.1
(12.6–15.8)8.2
(6.4–10.5)5.4
(4.0–7.3)12.2
(8.9–16.3)13.0
(11.0–15.3)10.2
(8.1–12.7)16.9
(14.0–22.2)Asian 4.7
(3.9–5.6)3.6
(2.6–4.9)4.9
(4.2–5.9)2.7
(1.8–4.0)3.2
(2.1–4.9)1.9
(1.0–3.7)4.4
(3.4–5.7)4.9
(3.5–6.7)3.9
(2.8–5.5)Other 1.8
(1.4–2.3)2.0
(1.3–3.0)1.8
(1.4–2.2)2.7
(1.8–4.2)1.9
(1.0–3.8)3.9
(2.3–6.3)3.5
(2.4–4.8)3.2
(2.1–4.9)3.7
(2.4–5.8)Insurance, % Any private 70.7
(67.6–72.0)69.9
(67.4–72.3)b70.9
(69.5–72.3)b55.1
(51.3–58.9)59.7
(55.0–64.1)b48.8
(43.5–54.1)b60.6
(57.8–63.3)62.2
(58.4–65.9)b58.8
(54.9–62.6)bPublic 15.6
(14.7–16.6)25.7
(23.6–27.9)13.3
(12.4–14.3)37.3
(34.0–40.8)35.8
(31.7–40.1)39.4
(34.9–44.2)30.5
(27.9–33.3)32.5
(29.2–36.0)28.4
(24.7–32.4)None 13.7
(12.8–14.6)4.4
(3.6–5.5)15.8
(14.8–16.9)7.6
(6.1–9.3)4.5
(3.1–6.7)11.8
(9.1–15.1)8.9
(7.5–10.6)5.3
(3.6–7.7)12.8
(10.7–15.3)Characteristic With Hyperlipidemia Odds Ratio (95% CI) P Value Without Hyperlipidemia Odds Ratio (95% CI) P Value Coronary artery disease 1.94 (1.58–2.40) <.001 11.10 (5.51–22.80) <.001 Diabetes 1.90 (1.59–2.28) <.001 8.56 (4.35–16.87) <.001 Hypertension 1.35 (1.14–1.60) .001 2.30 (1.29–4.11) .005 Cerebrovascular disease 0.87 (0.64–1.17) .36 0.59 (0.17–2.01) .40 Peripheral arterial disease 1.04 (0.60–1.81) .88 8.38 (2.71–25.93) <.001 Tobacco use 0.98 (0.82–1.16) .76 1.26 (0.60–2.65) .53 Sex (male) 1.19 (1.04–1.37) .01 1.47 (0.81–2.66) .21 Age (per year) 1.05 (1.04–1.05) <.001 1.06 (1.03–1.09) <.001 -
Notes: An odds ratio exceeding 1 indicates higher likelihood of statin use. Odds ratios are adjusted for insurance status, race, and poverty category.
-
- Table 3
Odds Ratios for Statin Use in Individuals Without Coronary Artery Disease or Diabetes
Characteristic Odds Ratio (95% CI) P Value Hyperlipidemia 91.65 (60.27–139.36) <.001 Age (per year) 1.06 (1.05–1.07) <.001 Hypertension 1.35 (1.12–1.64) .001 Sex (male) 1.33 (1.12–1.59) .002 Cerebrovascular disease 1.52 (1.01–2.29) .047 Peripheral arterial disease 1.59 (0.61–4.16) .34 Tobacco use 1.00 (0.79–1.27) .99 -
Notes: An odds ratio exceeding 1 indicates higher likelihood of statin use. Odds ratios are adjusted for insurance status, race, and poverty category.
-
The Article in Brief
Cardiovascular Risk and Statin Use in the United States: A Cross-Sectional Analysis
Michael E. Johansen , and colleagues
Background New guidelines from the American College of Cardiology and American Heart Association substantially broaden the number of individuals for whom statin medications are recommended, primarily by expanding the eligible population to lower levels of cardiovascular risk. This study examines the relationships between statin use and cardiovascular risk, diagnosis of hyperlipidemia (high cholesterol and triglyceride levels), and other risk factors.
What This Study Found Many people at high risk for cardiovascular disease, including those with coronary artery disease, diabetes or both, are not receiving statins. An estimated nine million people over 40 years of age with diabetes and 5.6 million people with coronary artery disease--populations that have clearly been shown to benefit from the drugs--are not on statins. Those with high cholesterol but without diabetes or heart disease are more likely to be on statins than those without high cholesterol but who have diabetes or heart disease. Given that individuals with heart disease or diabetes are at considerably higher cardiovascular risk, this pattern strongly supports the notion that statin use is being driven by high cholesterol instead of by overall cardiovascular risk.
Implications
- Recently released ACC-AHA guidelines offer an opportunity to reframe statins as medications that reduce cardiovascular risk rather than as medications that lower cholesterol.
Annals Journal Club
May/Jun: Diagnosis or Risk Factors to Guide Statin Use?
The Annals of Family Medicine encourages readers to develop a learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club and sharing the results of your discussions in the Annals online discussion for the featured articles. RADICAL is an acronym for Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. The word radical also indicates the need to engage diverse participants in thinking critically about important issues affecting primary care and then acting on those discussions.1
HOW IT WORKS
In each issue, the Annals selects an article or articles and provides discussion tips and questions. We encourage you to take a RADICAL approach to these materials and to post a summary of your conversation in our online discussion. (Open the article online and click on "TRACK Comments: Submit a response.") You can find discussion questions and more information online at: http://www.AnnFamMed.org/site/AJC/.
CURRENT SELECTION
Article for Discussion
- Johansen ME, Green LA, Sen A, Kircher S, Richardson CR. Cardiovascular risk and statin use in the United States. Ann Fam Med. 2014;12(3):215-223.
Discussion Tips
This study provides a chance to consider factors associated with taking statin drugs in a nationally-representative sample of patients, and to consider the implications for our own prescribing practices.
Discussion Questions
- What question is asked by this study and why does it matter?
- How does this study advance beyond previous research and clinical practice on this topic?
- How strong is the study design for answering the question?
- To what degree can the findings be accounted for by:
- How patients were selected, excluded, or lost to follow-up? (How representative is this nationally-representative survey?)
- How the main variables were measured?
- Confounding (false attribution of causality because 2 variables discovered to be associated actually are associated with a 3rd factor)?
- Chance?
- How the findings were interpreted?
- What are the main study findings?
- How comparable is the study sample to similar patients in your practice? What is your judgment about the transportability of the findings?
- What contextual factors are important for interpreting the findings?2-5
- How might this study change your practice? Policy? Education? Research?
- Who the constituencies are for the findings, and how they might be engaged in interpreting or using the findings?
- What are the next steps in interpreting or applying the findings?
- What researchable questions remain?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals Journal Club: It's time to get RADICAL. Ann Fam Med. 2006;4(3):196-197.
- Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;pii:S0735-1097(13)06028-2 (e-pub ahead of print).
- Eckel RH, Jakicic JM, Ard JD, et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;pii:S0735-1097(13)06029-4 (e-pub ahead of print);.
- Goff DC Jr, Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA Guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;pii:S0735-1097(13)06031-2 (e-pub ahead of print).
- Wenger NK. Prevention of Cardiovascular Disease: Highlights for the Clinician of the 2013 American College of Cardiology/American Heart Association Guidelines. Clin Cardiol. 2014;37(4):239-51.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Medications associated with fracture risk in patients with rheumatoid arthritis
- Strategies for enhancing the initiation of cholesterol lowering medication among patients at high cardiovascular disease risk: a qualitative descriptive exploration of patient and general practitioners perspectives on a facilitated relay intervention in Alberta, Canada
- Diagnosis of osteoporosis in statin-treated patients is dose-dependent
- Statin Use in the U.S. for Secondary Prevention of Cardiovascular Disease Remains Suboptimal
- Cross-sectional analysis of the prevalence and predictors of statin utilisation in Ireland with a focus on primary prevention of cardiovascular disease
- 2013 ACC/AHA Cholesterol Guideline Versus 2004 NCEP ATP III Guideline in the Prediction of Coronary Artery Calcification Progression in a Korean Population
- Evidence-Based Policy Making: Assessment of the American Heart Associations Strategic Policy Portfolio: A Policy Statement From the American Heart Association
- In This Issue: Many Arrows Rather than Magic Bullets
- Do Clinical Guidelines Still Make Sense? Yes