
Article Figures & Data
Figures
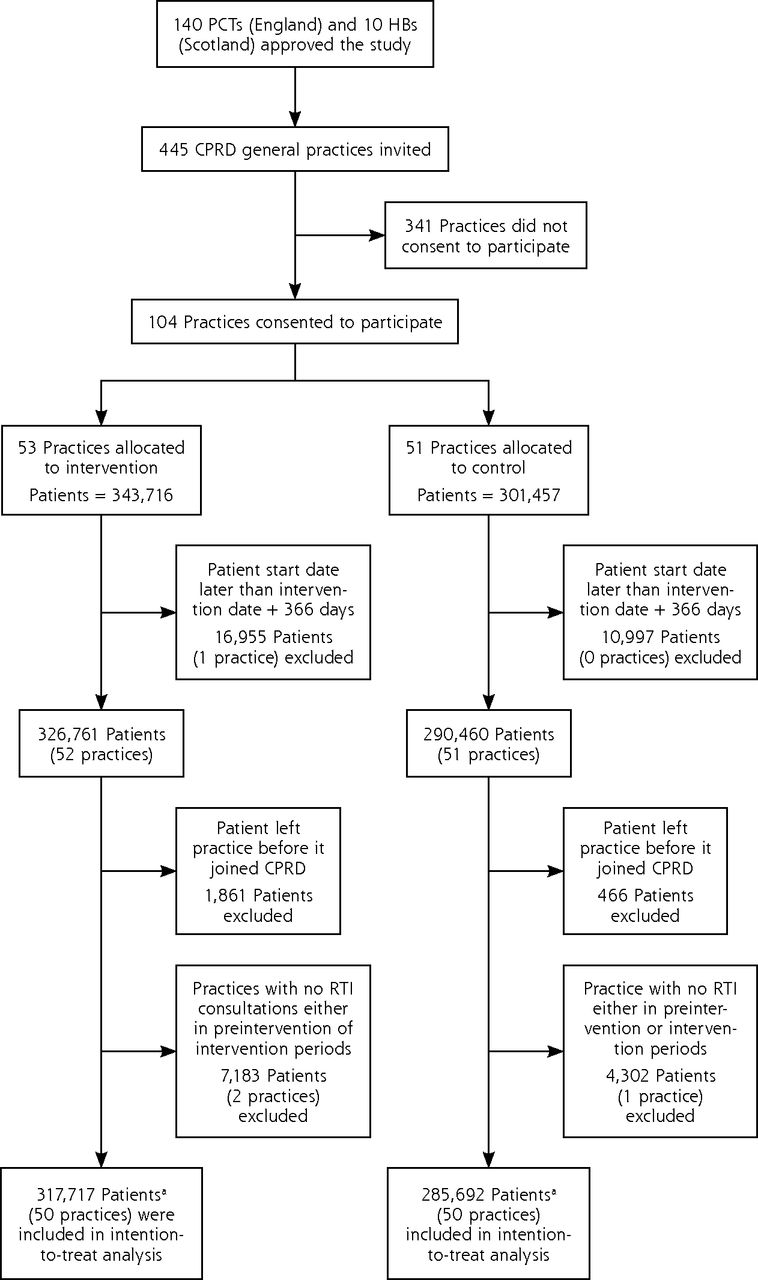
- Figure 1
Flow diagram charting progress through the trial.
CPRD = Clinical Practice Research Datalink; HB =Health Board; PCT = Primary Care Trust; RTI = respiratory tract infection.
a Figure includes participants contributing to analysis either in 12-month preintervention or 12-month intervention periods.

Tables
Characteristic Intervention Trial Arm Control Trial Arm Family practices Number of family practices 50 50 Mean eligible participants aged 18–59 y, No. 4,132 3,547 Distribution by region, No. (%)a London 8 (16) 9 (18) Midlands 9 (18) 8 (16) North 9 (18) 8 (16) South and East 13 (26) 13 (26) South West 8 (16) 8 (16) Scotland 3 (6) 4 (8) Distribution by start date, No. (%) December 2010 14 (28) 17 (34) January 2011 19 (38) 17 (34) March 2011 15 (30) 15 (30) April 2011 2 (4) 1 (2) Patients Eligible patients aged 18–59 y, No. 12-Month preintervention period 292,398 264,137 12-Month intervention period 294,929 263,895 Person years analyzed, No. 12-Month preintervention period 270,437 251,994 12-Month intervention period 283,776 234,373 Female patients, No. (%) 12-Month preintervention period 145,116 (50) 132,375 (50) 12-Month intervention period 147,199 (50) 132,378 (50) Patients aged 45–59 y, No. (%) 12-Month preintervention period 102,743 (35) 94,194 (36) 12-Month intervention period 102,317 (35) 93,850 (36) -
↵a Midlands includes East and West Midlands; North includes North East, North West, Yorkshire, and Humberside; South and East includes South Central, South East, and East Anglia.
-
- Table 2
Consultation and Antibiotic Prescribing for Respiratory Tract Infection per 1,000 Registered Patients
Characteristic Intervention Trial Arm Control Trial Arm Adjusted Mean Differenced (95% CI) P Value Before Mean (Range) After Mean (Range) Before Mean (Range) After Mean (Range) RTI consultation ratea 219 (181–254) 209 (176–247) 216 (186–246) 218 (184–244) −9.10 (−21.51 to 3.30) .148 Antibiotic prescription rateb 116 (91–131) 108 (87–129) 111 (86–135) 114 (85–128) −9.69 (−18.63 to −0.75) .034 Antibiotic prescriptions per RTI consultationc 53 (46–60) 52 (45–58) 52 (45–60) 52 (45–59) −1.85 (−3.59 to −0.10) .038 -
RTI=respiratory tract infection.
-
Note: Figures are mean (interquartile range) of family practice-specific values for 12 months before and after intervention.
-
↵a Consultation rate per 1,000 person-years.
-
↵b Antibiotic prescriptions for respiratory tract infections per 1,000 person-years.
-
↵c Proportion of consultations with antibiotic prescribed.
-
↵d Difference between intervention and control trial arms after intervention, adjusting for preintervention value, as well as mean age and proportion of women at each practice.
-
- Table 3
Proportion of Consultations for Different Types of Respiratory Tract Infection With Antibiotic Prescribed
Infection Type Intervention Trial Arm Control Trial Arm Adjusted Mean Differencea (95% CI) P Value Before Mean (Range) After Mean (Range) Before Mean (Range) After Mean (Range) Cough and bronchitis 47 (36–59) 45 (37–52) 46 (38–55) 47 (38–55) −2.49 (−4.83 to −0.15) .030 Colds 37 (21–48) 36 (22–46) 38 (27–50) 38 (30–49) −1.05 (−4.28 to 2.18) .519 Otitis media 59 (45–73) 56 (43–67) 60 (48–72) 57 (47–71) −1.54 (−6.85 to 3.77) .566 Rhinosinusitis 89 (82–95) 89 (83–92) 88 (86–94) 86 (82–93) 1.07 (−1.26 to 3.41) .362 Sore throat 58 (51–65) 57 (50–64) 57 (50–67) 57 (48–66) −1.59 (−4.27 to 1.09) .242 -
Note: Figures are mean (interquartile range) of family practice-specific values for 12 months before and after the intervention, except where indicated.
-
↵a Difference between intervention and control trial arms after intervention, adjusting for preintervention value, as well as mean age and proportion of women at each practice.
-
- Table 4
Intervention Utilization and Antibiotic Prescribing by Quartile of Intervention Utilization
Control Practices Lowest Quartile of Utilization (13)a Second Quartile (13) Third Quartile (13) Highest Quartile of Utilization (13) Intervention utilization (per 1,000 consultations for RTI) Prompt views, median (IQR) Not applicable 0 (0–0) 12 (7–18) 63 (46–68) 159 (104–166) Leaflets printed, median (IQR) Not applicable 0 (0–0) 6 (0–0) 3 (2–4) 25 (13–40) RTI consultations with antibiotics prescribed, % (IQR) Before intervention 52 (45–59) 55 (49–61) 53 (46–59) 55 (51–63) 50 (41–57) After intervention 52 (45–59) 54 (46–63) 54 (51–60) 53 (52–61) 48 (42–54) Unadjusted mean difference, No. (95% Cl) 0.7 (−0.6 to 2.0) −1.2 (−5.1 to 2.8) −1.0 (−2.9 to 0.9) −1.4 (−3.9 to 1.0) −1.6 (−5.0 to 1.7) Adjusted test for trend across categories, No. (95% CI)b −0.64 (−1.23 to −0.05),c P =.034
In Brief
Electronic Health Records for Intervention Research: A Cluster Randomized Trial to Reduce Antibiotic Prescribing in Primary Care (eCRT Study)
Alex Dregan , and colleagues
Background Because implementing cluster randomized trials can be logistically challenging, costly and time-consuming, researchers sought to evaluate the feasibility of conducting intervention research remotely using primary care electronic health records. Specifically, the authors looked at the effectiveness of electronically delivered decision support tools at reducing antibiotic prescribing for respiratory tract infections in a randomized trial of 603,409 primary care patients in England and Scotland.
What This Study Found Intervention arm practices used decision support tools remotely installed and delivered during consultations that were activated when family physicians entered a medical code for the respiratory tract infection. The tools provided information for education and decision support, including a summary of antibiotic prescribing recommendations, a patient-information sheet, summary of research evidence concerning no-antibiotic or delayed-antibiotic prescribing strategies, information on the definite indications for antibiotic prescription and information and evidence on the risks from nonprescribing. The researchers found the use of the intervention and its effect on care were low ? one-quarter of intervention family practices made little or no use of the intervention, and antibiotic prescribing was only slightly lower at practices that made greater use of the intervention (a 1.85% reduction in the proportion of consultations with antibiotics prescribed). Despite the limited impact, however, the study demonstrates that cluster randomized trials can be conducted remotely through electronic health records.
Implications
- Using electronic health records in intervention research, the authors assert, has the potential to allow large studies to be conducted at a low cost in settings where care is routinely delivered, making it suitable for the evaluation of important clinical and public health interventions.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Developing a data-enabled nudge intervention for childhood antibiotics in primary care: a qualitative study
- Electronic health record-based behaviour change interventions aimed at general practitioners in the UK: a mixed methods systematic review using behaviour change theory
- Optimising antimicrobial stewardship interventions in English primary care: a behavioural analysis of qualitative and intervention studies
- Peritonsillar Abscess and Antibiotic Prescribing for Respiratory Infection in Primary Care: A Population-Based Cohort Study and Decision-Analytic Model
- Theory-based electronic learning intervention to support appropriate antibiotic prescribing by nurse and pharmacist independent prescribers: an acceptability and feasibility experimental study using mixed methods
- Theory-based electronic learning intervention to support appropriate antibiotic prescribing by nurses and pharmacists: intervention development and feasibility study protocol
- Examining influences on antibiotic prescribing by nurse and pharmacist prescribers: a qualitative study using the Theoretical Domains Framework and COM-B
- Effectiveness and safety of electronically delivered prescribing feedback and decision support on antibiotic use for respiratory illness in primary care: REDUCE cluster randomised trial
- Relationship between prescribing of antibiotics and other medicines in primary care: a cross-sectional study
- Advances in optimizing the prescription of antibiotics in outpatient settings
- Electronically delivered, multicomponent intervention to reduce unnecessary antibiotic prescribing for respiratory infections in primary care: a cluster randomised trial using electronic health records--REDUCE Trial study original protocol
- Safety of reduced antibiotic prescribing for self limiting respiratory tract infections in primary care: cohort study using electronic health records
- Continued high rates of antibiotic prescribing to adults with respiratory tract infection: survey of 568 UK general practices
- In This Issue: Technical and Personal Systems, and Novel Risk Factors