
Abstract
The recent confluence of: (1) changing state and national insurance-related policies, and (2) the rapid growth in electronic health record (EHR) use, yields an unprecedented opportunity for patient-centered medical homes (PCMHs) and other primary care practices or care settings to use health information technology (HIT) and health information exchange (HIE) in novel ways to impact patient health. We propose that HIT is an untapped resource for supporting clinic-based efforts to help eligible patients obtain and maintain insurance coverage. This commentary presents a conceptual model and guiding principles for this idea. Additionally, it describes insurance support tools that could be used to conduct ‘inreach’ and ‘outreach’ with patients around health insurance, similar to how HIT is used to manage chronic disease and panels of patients, and to improve population health outcomes.
INTRODUCTION
Expansions in health insurance are concurrent with increasing implementation and adoption of electronic health records (EHRs) and other health information technology (HIT). Such changes present a unique opportunity for patient-centered medical homes (PCMHs) and other primary care practices or care settings to use HIT to maximize coverage among eligible patients.1,2 We propose that insurance coverage gaps are often preventable,3–5 and that HIT is an untapped resource for closing these gaps. Since even short gaps in health insurance can negatively impact patient outcomes,6–8 these opportunities for increased coverage have the potential to improve health.
In a previous essay, we discussed how PCMHs could view uninsurance as a chronic illness and apply tenets and tools of the Chronic Care Model to treat it.9 In follow-up, this commentary: (1) provides guiding principles for HIT infrastructure development to support health insurance enrollment and re-enrollment, and (2) describes how HIT and health information exchange (HIE) could be used to organize and communicate this information to patients.
Guiding Principles For the Use of HIT and HIE to Help Keep Patients Insured
Patients are usually affiliated with multiple organizations which impact their health. For example, a patient may simultaneously: (1) be enrolled in an insurance program (eg, Medicaid); (2) receive medical services; and (3) receive educational and social services from local, county, or state facilities. Historically, information relevant to a patient’s health has not been integrated or coordinated across multiple organizations; in particular, data from insurance payers were rarely made available to medical care teams. Though HIE efforts have recently increased the ability to share aggregated patient-level clinical data across health care organizations,10,11 its use remains minimal in clinical settings. One study found users accessed an available HIE system during only 2.3% of encounters.12
As HIT and HIE capabilities have grown, the potential to share diverse data across organizations in ways that could benefit patients’ health has also improved. For example, HIT is being used in some health care settings to improve communication between patients and care teams and to address federal priorities to improve the ‘Meaningful Use’ of EHRs.13 Our guiding principles suggest PCMHs and other primary care practices or care settings could use HIT, including EHR functionalities, to help patients maintain health insurance coverage, and how these tools enable communication and enrollment support.9 In addition, we suggest developing HIE systems that facilitate the transfer of coverage information between a patient’s insurer and other health-related organizations.
Bringing Insurance Support into Health Care Settings
Patients are often unclear about the need to reapply for health insurance coverage, or unsure of coverage expiration dates.14 Additionally, patients in the same family often have different types of coverage, with variable enrollment requirements. In the past, patients have not usually received health insurance assistance from their medical providers. Most previous efforts to assist individuals with health insurance enrollment and retention occurred outside of health care settings (eg, employment settings, state Medicaid offices, etc) and did not take advantage of EHR data. Health care settings, however, often have information about patients’ eligibility for and enrollment in health insurance programs. These data are usually manually entered or automatically imported into many EHRs, and pertain to current insurance plan coverage. They sometimes include information about income and employment; yet they are used solely to facilitate billing and little else. We propose that PCMHs and others could employ several new methods for harnessing EHR data, HIT tools, and HIE capabilities to help eligible patients obtain and maintain health insurance coverage.
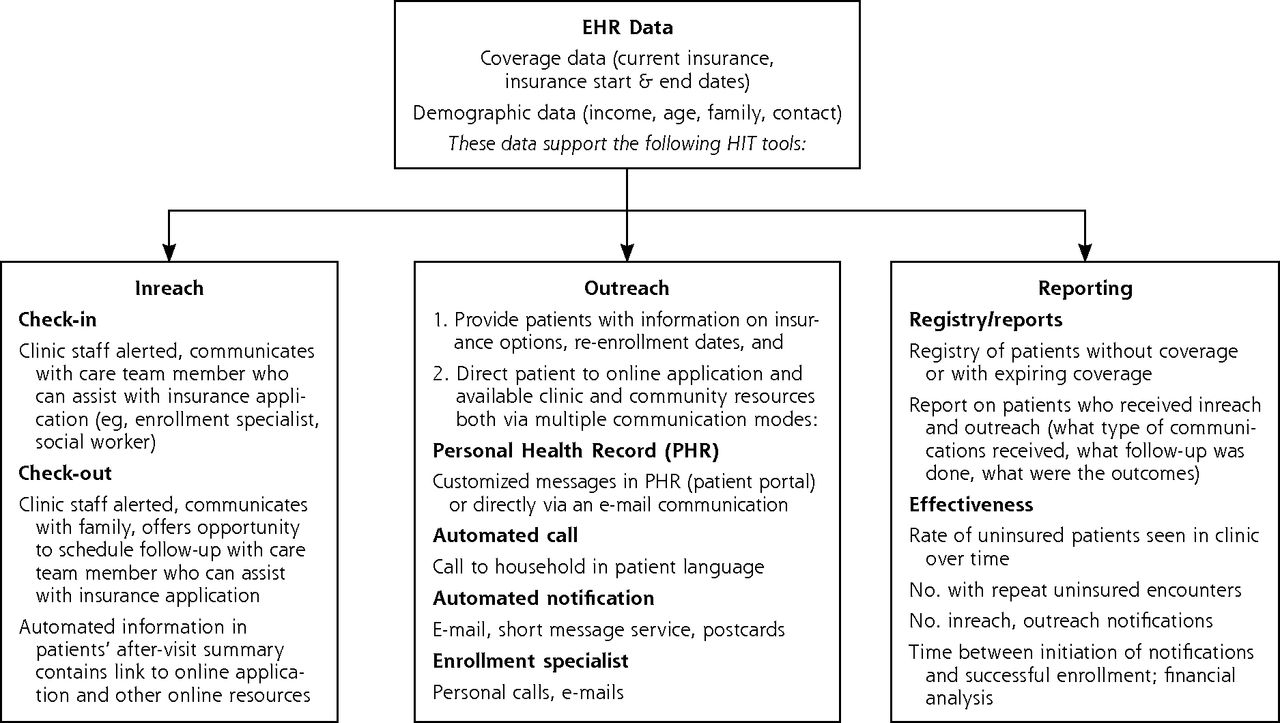
First, data on insurance coverage and eligibility must be consistently and accurately recorded in the EHR. A good starting place is the data already being collected and/or automatically imported. PCMHs could work with their health care systems and/or EHR vendors to create or enhance electronic interfaces with insurance plans, populating EHR fields with more detailed information about patients’ health insurance coverage status. At a minimum, we recommend clinics collect start and end dates of coverage and basic demographic data, including income and age, to help assess insurance eligibility. Once such information is reliably captured into discrete EHR fields, the data could be aggregated to support functions which facilitate numerous activities (Figure 1).

Use of health information technology (HIT) to help keep patients insured.
With these data, existing HIT functionality to support the activities shown in Figure 1 could be adapted from panel management and clinical decision-support tools proven effective in chronic disease management. These functions include ‘inreach,’ in the form of automated rule-based reminders (eg, ‘pop-ups’) that activate when a patient checks into the clinic. This reminder would prompt front desk staff to talk with patients about their health insurance expiration date and/or facilitate referrals to appropriate resources within (eg, enrollment specialists or clinic staff who specialize in coverage assistance) or outside (eg, state or federal websites and local agencies available to assist patient with health insurance enrollment) the clinic.9,15–20 For clinics that ask about health insurance information before a visit, tools could be tailored to identify scheduled patients without coverage and facilitate communication between the enrollment specialist and patient regarding their potential options to gain insurance. In addition, EHR tools could create customized messages about potential insurance plans available to the patient (if uninsured), or enrollment expiration dates (if insured), to be included with the after-visit summary.
To support ‘outreach,’ coverage eligibility data could be aggregated into registries of patients who are uninsured or nearing their health insurance expiration/re-enrollment date. Registry data could support automated systems that facilitate and track voicemail, e-mail, text, or other communications to patients. Such data could also feed into a personal health record or patient portal, enabling patients to receive automated, customized messages with information about their eligibility for health insurance, enrollment expiration dates, and Internet links to online applications or resources.9
HIT tools supporting health insurance inreach and outreach could be tailored to meet the needs of specific care settings and patient populations. For example, a federally qualified health center that serves uninsured and publically insured patients could benefit from tools that help identify and reach uninsured patients who are eligible for public coverage, or communicate expiration dates to patients. In practices with insured patients, the tools might emphasize selection of the most appropriate coverage for their needs.
There is a significant business case for implementing HIT systems to help keep patients insured. For example, clinicians in traditional fee-for-service markets benefit when patients are insured. Patients who lose coverage are often unable to schedule visits, so they seek care outside of visits (eg, telephone calls, e-mails) in ways that are not commonly reimbursed.21–23 In health care settings that see a large number of uninsured patients, such as community health centers (CHCs), it is financially imperative to keep eligible patients insured. One study of 185,959 CHC pediatric patients found that 38,726 uninsured children visited a CHC; 11,618 remained uninsured at all subsequent visits in a 2-year time period.24 Assuming a $27.82 Medicaid fee-for-service reimbursement rate for an office visit with an established patient,25 the clinic lost $323,212.76 in revenue during that period. The amount could be much higher depending on the payer and/or how complicated the visit was.
As the Accountable Care Organization model and global payments spread, outreach functions such as those proposed here would address the imperative to conduct panel management and other population health approaches to care,10 and optimize reimbursement for a population’s health care. Clinicians being paid to care for a population of patients will want to keep them continuously insured in order to optimize reimbursement. Clinicians incentivized to improve health outcomes in a panel of patients will want to help their patients stay insured, to make sure they have coverage for and access to recommended preventive care (eg, mammograms, immunizations) and chronic disease care services (eg, laboratory tests for monitoring diabetes). Although the business case for developing and implementing such tools is sound, the primary benefit would be to keep patients insured so as to maximize their ability to access essential health care services.
In addition to collecting and sharing information to keep patients insured, HIT could be developed to identify which health insurance plans best meet a patient’s needs. Such functions could incorporate clinical information from the EHR (eg, diagnoses, current medications) into a decision worksheet to help patients understand what health insurance benefits they might need, and how to predict downstream costs associated with their coverage options. The worksheet could illustrate how certain low-cost plans with high deductibles, restrictive networks, and copays might cost more in the long term. For some patients with costly medications and other treatments necessary to manage their chronic diseases, this tool could help them better understand how a plan with a cheaper premium might have higher downstream costs that could hinder their ability to access care and stay healthy. This would be particularly helpful for ACA-related coverage options, as they are known for having high deductibles and restrictive networks.26 These HIT and HIE capabilities could expand upon existing functionality in some EHRs that exchange information regarding services covered by insurance (eg, SureScripts, which continually updates insurance formulary information to enable clinicians to see the cost of a prescription when it is being electronically prescribed.)
Limitations
Utilizing HIT to assist patients with insurance retention has potential issues and pitfalls. For example, technology development is expensive, as is clinic staff time to conduct activities related to patient insurance enrollment and retention. Another issue is confidentiality; HIEs hold promise, but patients may not be comfortable having certain information or sensitive data (eg, citizenship or employment) collected and shared across organizations. Despite these limitations, we believe there is a compelling case for using HIT to support continuous health insurance.
Policy Relevance
Recent policies to expand Americans’ insurance coverage options include the Children’s Health Insurance Program, reauthorized in 2009, which successfully expanded health insurance coverage options for millions of US children, and the Affordable Care Act (ACA), through which millions of children and adults will have increased access to coverage.27,28 Concurrently, policies incentivizing the meaningful use of EHRs and HIE were authorized by Congress.2,29 After passage of the Health Information Technology for Economic and Clinical Health (HITECH) Act, many US health care systems implemented EHRs. By 2012, 72% of office-based physicians were using an EHR.30 Meaningful use Stage 2 builds on these efforts, mandating increased interoperability between disparate HIT systems, and creating additional opportunities for HIE. These confluent events yield an unprecedented opportunity to use clinical data and functions in novel ways.15–20
Although some clinics already engage in health insurance outreach activities and insurance coverage discussions with patients, these efforts are not usually supported by HIT or HIE. We anticipate that many health care organizations will embrace having enhanced capacity to help their patients obtain and keep coverage because of the benefits to be gained from having stably insured patients. Insurance coverage is associated with the receipt of necessary health care,7 so HIT functions that support coverage may improve patients’ access to care, and consequently their health outcomes.
The ideas presented here are intended to challenge readers to consider how HIT can be used to help support patients in new ways. Using HIT to support clinics’ efforts to conduct health insurance inreach and outreach to patients is just one example of a novel way to harness HIT capabilities and expand the scope and function of an EHR; our example may be differentially relevant to readers depending on their own experience, state policy environment, and practice setting. We recognize that this idea pushes the boundaries of services traditionally provided in medical care settings, and of how medical practices are currently organized. Recent policy changes, however, have created opportunities for primary care organizations to adapt and innovate in order to serve patients better in a changing environment.31 Those involved with primary care delivery and HIT/HIE design and policy must lead this thinking, and contribute to new ways that care settings can address the health care Triple Aim: better population health, better health care, and lower cost per capita.32
CONCLUSIONS
We present guiding principles and strategies for harnessing HIT to support health insurance enrollment and retention efforts within primary care clinics. The methodologies, while novel, are based on currently available EHR and HIE tools. These efforts are timely in terms of current policy initiatives, as they have the potential to maximize insurance coverage continuity for many patients and positively impact the health care Triple Aim.
Footnotes
-
Conflicts of interest: authors report none.
-
Funding support: This work was financially supported by the Agency for Healthcare Research and Quality (AHRQ) grant number (1 R01 HS018569), the Patient-Centered Outcomes Research Institute (PCORI), the National Cancer Institute (NCI) of the National Institutes of Health, grant number (1 R01 CA181452 01), and the Oregon Health & Science University Department of Family Medicine. The funding agencies had no involvement in the preparation, review, or approval of the manuscript.
- Received for publication March 20, 2014.
- Revision received July 1, 2014.
- Accepted for publication August 5, 2014.
- © 2014 Annals of Family Medicine, Inc.




{kind=link}