
Abstract
Lower rates for breast cancer screening persist among low income and uninsured women. Although Medicare and many other insurance plans would pay for screening mammograms done during hospital stays, breast cancer screening has not been part of usual hospital care. This study explores the mean amount of money that hospitalized women were willing to contribute towards the cost of a screening mammogram. Of the 193 enrolled patients, 72% were willing to pay a mean of $83.41 (95% CI, $71.51–$95.31) in advance towards inpatient screening mammogram costs. The study’s findings suggest that hospitalized women value the prospect of screening mammography during the hospitalization. It may be wise policy to offer mammograms to nonadherent hospitalized women, especially those who are at high risk for developing breast cancer.
INTRODUCTION
Breast cancer screening campaigns have reduced the disparity in mammography utilization by race, and the remaining differences may be largely explained by socioeconomic status and access to health care.1–2 Screening mammography has traditionally been offered in the outpatient setting. A recent study reported that almost 40% of hospitalized women were nonadherent with breast cancer screening, and a majority of hospitalized women claimed to be willing to undergo inpatient screening mammography if due and offered during hospitalization.3 Inpatient screening mammography may be more expensive than outpatient testing due to facility charges and radiology fee structures. Because of this potential cost differential, we set out to determine whether hospitalized women who are amenable to inpatient screening mammography would be willing to contribute towards the cost of the test. This study further seeks to establish the amount that hospitalized women are willing to pay towards an inpatient screening mammogram.
METHODS
We enrolled 250 women aged 50 to 75 years admitted to the general medicine service of Johns Hopkins Bayview Medical Center. Details of the enrollment methods have been published elsewhere.3 Of the patients enrolled, 57 (23%) were not interested in or amenable to inpatient screening mammography. They were excluded because we could not ask if they were willing to contribute to offset the cost of the test, leaving 193 women in the study group. Contingent valuation methods were used to assess the pretest contribution these women considered justified by the convenience of an inpatient screening mammogram. Contingent valuation is an economic technique that offers researchers the ability to assess the value of a health care service to patients by asking what they would be willing to pay for the service.4 The willingness-to-pay (WTP) variable may approximate patient-centeredness by allowing scientific inquiry to estimate how individuals value health care services.5 We asked the following question: “Current practice is not to order screening mammograms during one’s hospital stay, and you will not have one during this admission. However, in the future, if your hospital providers were able to arrange for a screening mammogram while you were in the hospital, would you be willing to pay $x out of pocket to offset the costs of this test?” Each respondent was randomly assigned one of 6 possible amounts for x (x = $5, $10, $30, $50, $75, or $125). The respondents were instructed to answer either “Yes” or “No,” thereby indicating whether the stated dollar amount was acceptable. This study was approved by the Institutional Review Board at our institution.
Respondent characteristics (presented as proportions and means) were compared using unpaired t test and χ2 tests. The probit regression model was used for the analysis of contingent valuation data to predict mean WTP. We used Stata statistical software, version 12.1 (StataCorp LP) for the analysis.6
RESULTS
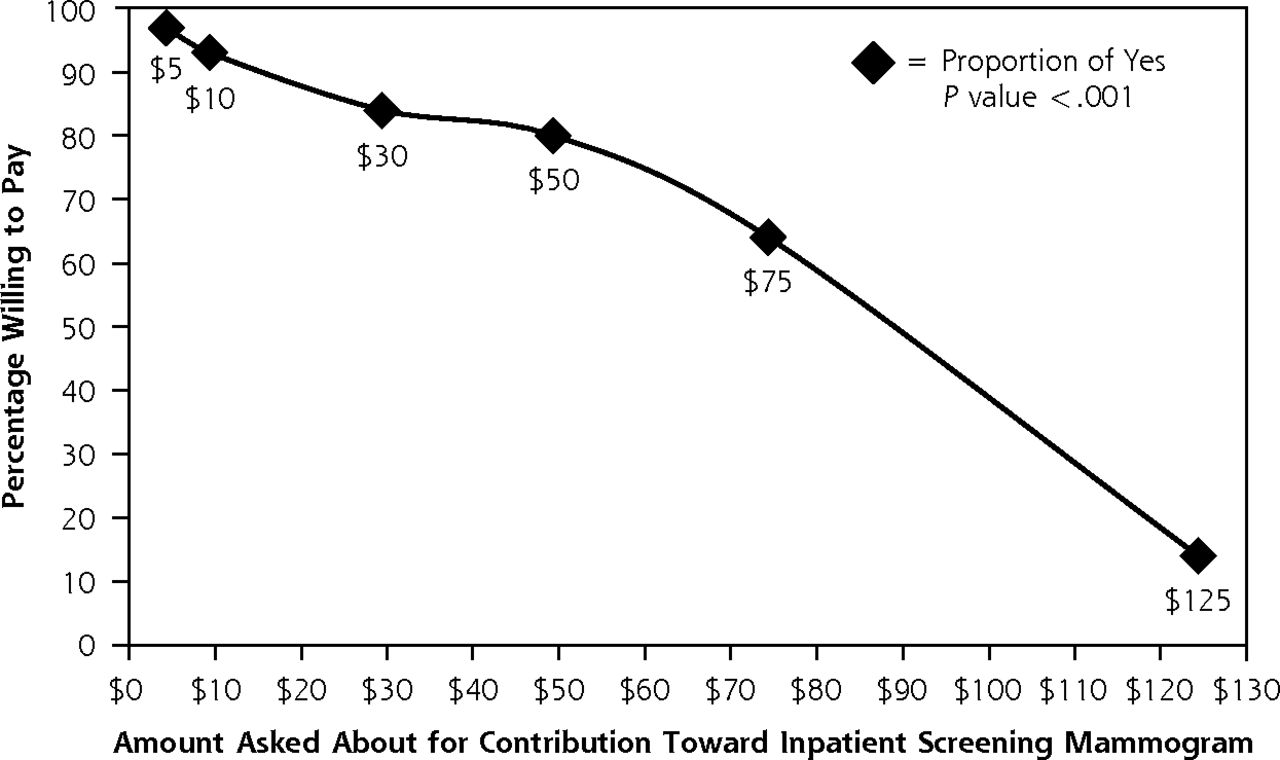
Characteristics of the study participants are shown in Table 1. The proportion of women willing to contribute toward inpatient screening mammography was inversely related to the dollar amount proposed (P <.001) in the contingent value question (Figure 1). The median acceptable WTP amount was $30. Using the Probit regression model, the unadjusted mean WTP amount was $84.14 (95% CI, $72.56–$95.74). After adjusting for 14 variables that could potentially influence WTP (Supplemental Appendix), the mean WTP was essentially unchanged ($83.41; 95% CI, $71.51–$95.31).

Proportion of hospitalized women willing to pay each of 6 amounts for inpatient screening mammography.
Characteristics of Hospitalized Women Who Would Be Willing to Have a Mammogram During a Hospitalization if it Were Due, Stratified by WTP Status
DISCUSSION
Our study suggests that a majority of hospitalized women, including those from low-income and high-risk groups, are willing to contribute money to offset the cost of screening mammography. This may not be a surprising finding because some of the barriers that women face when attempting to have a mammogram (difficulty in arranging transportation, forgetting to schedule the test, desire to avoid losing time at work, etc) are inconsequential when having the mammography performed during hospitalization.
Contingent valuation methods may be particularly relevant for understanding health prevention preferences, and they can generate estimates that may inform public policy considerations.7 The results of WTP analyses in health care are known to be influenced by respondent variables such as income, education, age, and race.8,9 No significant influence of such variables on WTP was found in our fairly diverse study population.
Many hospitalized patients are well behind on their routine preventive care. Nonetheless, cancer screening is not routinely performed in current hospital-based practice. Rationalizations for this include these: breast issues are unrelated to the reason for hospitalization, insurance coverage is uncertain, abnormal results would need follow-up, and hospitals may lack inpatient mammography services. Perhaps surprising to some, Medicare and most insurance companies cover screening mammograms ordered in the inpatient setting for hospitalized patients.10
Hospitalizations, when patients have time to reflect on their health in environments with a wealth of health care resources, may represent an opportunity for clinicians to optimize patients’ care by establishing patient-centered care plans.11 For this to become the norm would require a culture change in the field of hospital medicine and our nation’s inpatient units. As hospitals become core components of accountable care organizations, screening must become easier to coordinate in all settings.
Several limitations of this study should be considered. First, the study was conducted at a single hospital. Second, there may be concerns about the use of hypothetical questions, anchoring, and possible framing effects. Third, we did not solicit input about the potential impact of screening on the health care organization and its staff. Fourth, we previously reported that a substantial minority of women who were nonadherent to breast cancer screening cited barriers such as low priority compared to other problems or fear. These barriers would not necessarily be removed by offering screening during a hospital stay.3
Nevertheless, we did find that many hospitalized women want mammograms performed while they are in the hospital if they are due. Further, they are willing to share in the cost of the test. This represents more than a subtle preference. If we are truly moving towards patient-centered care, our hospitals will need to work out feasibility issues for breast cancer screening, including ways of deciding who is eligible and assigning responsibility for followup of abnormal results.
Footnotes
-
Conflicts of interest: authors report none.
-
Financial Support: Dr Wright is a Miller-Coulson Family Scholar, and this support comes from Hopkins Center for Innovative Medicine. This work was made possible in part by the Maryland Cigarette Restitution Fund Research Grant at Johns Hopkins.
-
Supplementary materials: Available at http://www.annfammed.org/content/12/6/556/suppl/DC1/.
- Received for publication March 17, 2014.
- Revision received April 16, 2014.
- Accepted for publication July 3, 2014.
- © 2014 Annals of Family Medicine, Inc.




{kind=link}