
Article Figures & Data
Figures
- Figure 1
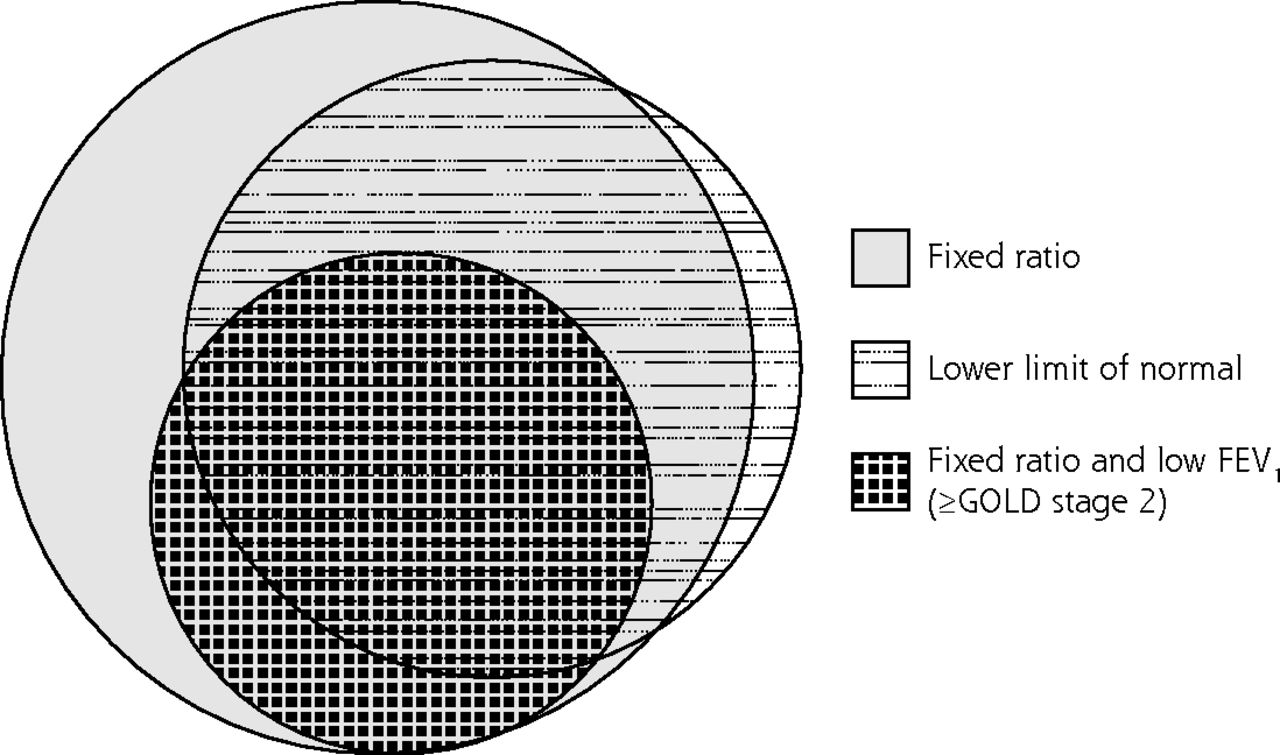
Venn diagram showing groups meeting various criteria for airflow limitation: the fixed ratio, the lower limit of normal, and the fixed ratio plus a low FEV1.
FEV1 = forced expiratory volume in 1 second; GOLD = Global Initiative for Chronic Obstructive Lung Disease.
Note: Low FEV1 is a value less than 80% of the predicted value.
- Figure 2
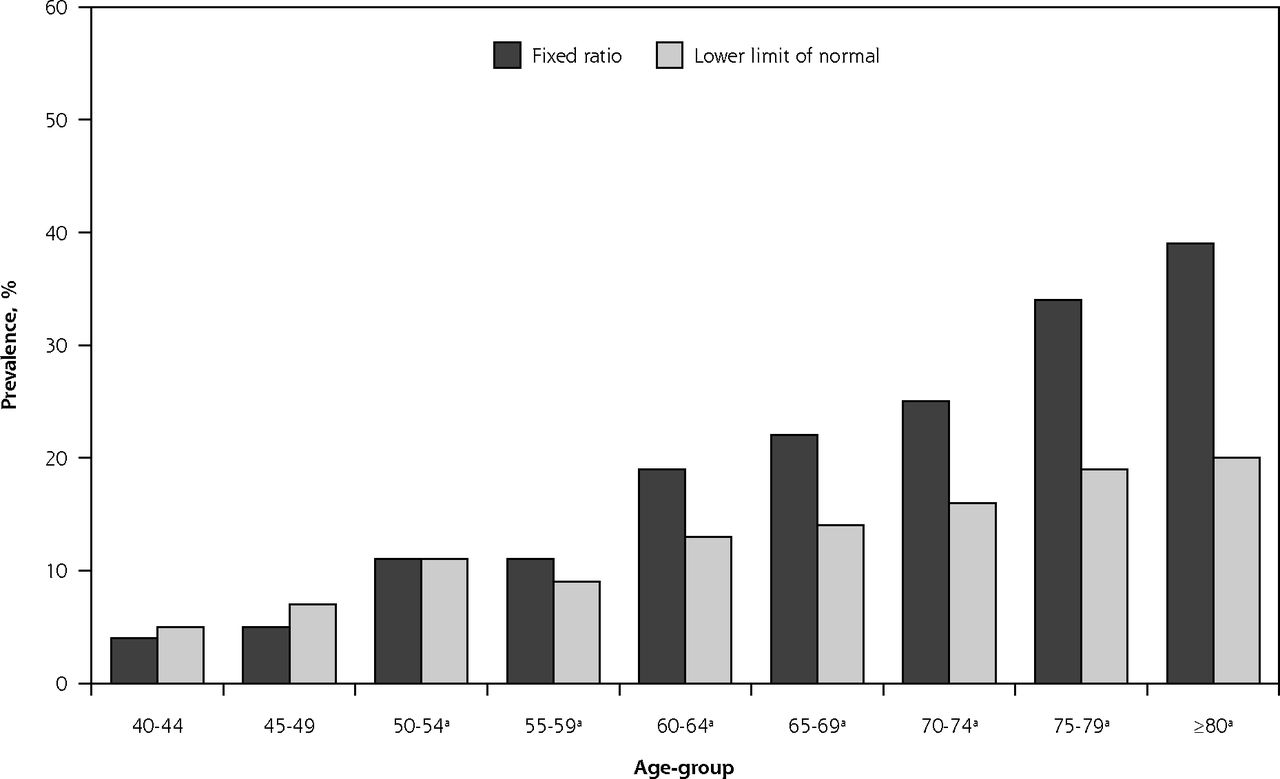
Prevalence of airflow limitation among men as determined by fixed ratio and by lower limit of normal.
aPrevalence differs significantly by fixed ratio vs lower limit of normal (P <.05).
- Figure 3
Prevalence of airflow limitation among women determined by fixed ratio and by lower limit of normal.
aPrevalence differs significantly by fixed ratio vs lower limit of normal (P <.05).


Tables
- Table 1
Patient Characteristics at Baseline, According to Criteria Used to Define Airflow Limitation
Characteristic Total (N = 4,882) No Airflow Limitationa (n = 4,038) Airflow Limitation FR+/LLN− (n = 297) FR−/LLN+ (n = 15) FR+/LLN+ (n = 532) FR+ and Low FEV1b,c (n = 363) LLN+ and Low FEV1b (n = 304) Age, mean (SD), y 57 (11) 56 (11) 68 (10) 45 (3) 62 (12) 64 (11) 63 (11) Sex (male), No. (%) 2,093 (43) 1,668 (41) 186 (63) 1 (7) 238 (45) 177 (49) 138 (45) Postbronchodilator FEV1, mean (SD), % predicted 95 (17) 98 (15) 92 (16) 77 (18) 77 (18) 65 (12) 64 (12) Postbronchodilator FVC, mean (SD), % predicted 97 (15) 96 (15) 101 (17) 99 (12) 98 (19) 85 (14) 86 (14) Body mass index, kg/m2 28 (6) 28 (6) 27 (5) 28 (5) 28 (5) 28 (6) 28 (6) Tobacco smoking status, No. (%)d Never smoker 2,091 (43) 1,852 (46) 95 (32) 8 (53) 136 (26) 73 (20) 100 (33) Former smoker 2,058 (42) 1,657 (41) 158 (53) 1 (7) 242 (46) 178 (49) 142 (47) Current smoker 729 (15) 527 (13) 43 (15) 6 (40) 153 (29) 111 (31) 61 (20) Education ≤12 years, No. (%) 493 (10) 366 (9) 43 (15) 0 (0) 83 (16) 65 (18) 55 (18) Race (white), No. (%) 4,464 (91) 3,663 (91) 277 (93) 14 (93) 510 (96) 343 (94) 290 (95) Conditions, No. (%) Chronic cough 619 (13) 432 (11) 45 (15) 6 (40) 136 (26) 113 (31) 102 (34) Chronic phlegm 467 (10) 312 (8) 35 (12) 1 (7) 119 (22) 96 (26) 85 (28) Chronic bronchitise 213 (4) 136 (3) 17 (6) 1 (7) 59 (11) 51 (14) 65 (21) Wheeze 1,273 (29) 939 (25) 78 (31) 8 (53) 248 (52) 192 (60) 166 (61) MRC dyspnea scalef 1.4 (0.8) 1.3 (0.7) 1.4 (0.8) 1.7 (1.2) 1.8 (1.1) 2 (1) 2.03 (1.2) SF-12 scores, mean (SD)g Physical scale 50 (9) 51 (9) 50 (9) 46 (14) 47 (11) 45 (11) 44 (12) Mental scale 52 (9) 52 (9) 54 (8) 49 (11) 52 (9) 53 (9) 52 (10) Exacerbation, No. (%) 996 (20) 779 (19) 58 (20) 4 (27) 155 (29) 119 (33) 100 (33) Cardiovascular disease, No. (%) 605 (12) 436 (11) 76 (26) 1 (7) 92 (17) 81 (22) 66 (22) -
FEV1 = forced expiratory volume in 1 second; FR = fixed ratio; FVC = forced vital capacity; LLN = lower limit of normal; MRC = Medical Research Council; SF-12 = Short Form 12-item health survey.
Notes: Continuous data are presented as mean (SD), dichotomous values as number (%). P value: univariate analysis of variance (ANOVA) or Kruskal-Wallis test for continuous variables and χ2 test for dichotomous variables.
-
↵a FR−/LLN−.
-
↵b FEV1 <80% of predicted.
-
↵c Collectively, these 2 criteria constitute Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage 2 or higher disease.
-
↵d Tobacco smoking status includes both cigarette and pipe smoking.
-
↵e Chronic cough and chronic phlegm for more than 2 years.
-
↵f MRC dyspnea scale scores range from 0 to 5; higher scores indicate worse health/dyspnea.
-
↵g SF-12 Physical and Mental scale scores range from 0 to 100; higher scores indicate better health.
-
- Table 2
Associations Between Airflow Limitation According to Various Criteria and Outcomes
Outcome No Airflow Limitationa (n = 4,038) Airflow Limitation FR+/LLN− (n = 297) FR+/LLN+ (n = 532) Chronic cough 1.00 1.40 (0.99–1.98) 2.54 (2.03–3.18) Chronic phlegm 1.00 1.43 (0.97–2.10) 3.04 (2.39–3.87) Chronic bronchitis 1.00 1.59 (0.93–2.72) 3.14 (2.25–4.37) Wheeze 1.00 1.54 (1.15–2.06) 3.25 (2.65–3.97) MRC dyspnea scaleb 1.00 1.14 (0.86–1.52) 2.33 (1.92–2.82) SF-12 Physical component scalec 1.00 −0.78 (.17) −3.31 (<.01) SF-12 Mental component scalec 1.00 0.47 (.40) −0.30 (.49) Exacerbation 1.00 1.33 (0.98–1.81) 1.90 (1.54–2.34) Cardiovascular disease 1.00 1.52 (1.14–2.04) 1.21 (0.93–1.56) -
FR = fixed ratio; LLN = lower limit of normal; MRC = Medical Research Council; SF-12 = Short Form 12-item health survey.
Notes: Multiple logistic regression analysis, except as otherwise noted. All models adjusted for age-group (<60 years), sex, and ever smoking. Data are presented as odds ratios (95% CIs) or parameter estimates (P values) from regression analysis. Number of FR−/LLN+ patients was too small for inclusion.
-
↵a Reference group (FR−/LLN−).
-
↵b Ordinal logistic regression analysis.
-
↵c Multiple linear regression analysis.
-
- Table 3
Associations Between Airflow Limitation According to Various Definitions and Outcomes
Outcome FR+/LLN−a (n = 297) FR+/LLN+ (n = 532) Chronic cough 1.00 1.81 (1.24–2.65) Chronic phlegm 1.00 2.13 (1.41–3.21) Chronic bronchitis 1.00 1.98 (1.12–3.48) Wheeze 1.00 2.11 (1.52–2.93) MRC dyspnea scaleb 1.00 2.04 (1.48–2.81) SF-12 Physical scalec 1.00 −2.39 (<.01) SF-12 Mental scalec 1.00 −1.10 (.11) Exacerbation 1.00 1.43 (1.01–2.02) Cardiovascular disease 1.00 0.79 (0.55–1.13) -
FR = fixed ratio; LLN = lower limit of normal; MRC = Medical Research Council; SF-12 = Short Form 12-item health survey.
Notes: Multiple logistic regression, except as otherwise noted. All models adjusted for age-group (<60 years), sex, and ever smoking. Data are presented as odds ratios (95% CI) or parameter estimate (P value) from regression analysis.
-
↵a Reference group.
-
↵b Ordinal logistic analysis.
-
↵c Multiple linear regression analysis.
-
- Table 4
Associations Between Airflow Limitation Criteria Alone and Further Refined by FEV1 and Outcomes
Outcome No Airflow Limitationa (n = 4,038) Airflow Limitation FR+ and Normal FEV1 (n = 466) LLN+ and Normal FEV1 (n = 248) FR+ and Low FEV1b,c (n = 363) LLN+ and Low FEV1b (n = 304) FR+ and LLN+ and Low FEV1b (n = 299) Chronic cough 1.00 1.32 (1.0–1.7) 1.59 (1.12–2.25) 3.32 (2.6–4.3) 3.65 (2.8–4.8) 3.64 (2.78–4.77) Chronic phlegm 1.00 1.55 (1.1–2.1) 1.83 (1.25–2.67) 3.65 (2.8–4.8) 3.91 (2.9–5.2) 4.10 (3.08–5.46) Chronic bronchitis 1.00 1.51 (1.0–2.4) 1.60 (0.90–2.82) 3.97 (2.8–5.7) 4.31 (3.0–6.3) 4.48 (3.09–6.51) Wheeze 1.00 1.59 (1.3–2.0) 2.15 (1.63–2.86) 4.50 (3.5–5.7) 4.60 (3.5–6.0) 4.58 (3.51–5.96) MRC dyspnea scaled 1.00 1.06 (0.8–1.3) 1.27 (0.95–1.69) 3.65 (2.9–4.6) 3.92 (3.1–5.0) 3.86 (3.03–4.92) SF-12 Physical scalee 1.00 −0.083 (.85) –0.85 (.15) −5.45 (<.01) −5.56 (<.01) −5.52 (<.01) SF-12 Mental scalee 1.00 −0.030 (.95) −0.22 (.71) −0.041 (.93) −0.42 (.44) −0.42 (.45) Exacerbation 1.00 1.25 (1.0–1.6) 1.37 (1.01–1.86) 2.39 (1.9–3.0) 2.32 (1.8–3.0) 2.39 (1.84–3.11) Cardiovascular disease 1.00 1.20 (0.9–1.6) 0.79 (0.52–1.21) 1.51 (1.1–2.0) 1.53 (1.1–2.1) 1.56 (1.15–2.12) -
FEV1 = forced expiratory volume in 1 second; FR = fixed ratio; LLN = lower limit of normal; MRC = Medical Research Council; SF-12 = Short Form 12-item health survey.
Notes: Multiple logistic regression analysis, except as otherwise noted. All models adjusted for age-group (<60 years), sex, and ever smoking. Data are presented as adjusted odds ratios (95% CI) or parameter estimate (P value) from regression analysis.
-
↵a Reference group (FR−/LLN−).
-
↵b FEV1 <80% of predicted.
-
↵c Collectively, these 2 criteria constitute Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage 2 or higher disease.
-
↵d Ordinal logistic regression analysis.
-
↵e Multiple linear regression analysis.
-
The Article in Brief
Clinical relevance of fixed ratio vs lower limit of normal of FEV1/FVC in COPD: patient-reported outcomes from the CanCOLD cohort
Wouter van Dijk , and colleagues
Background Currently, there is no consensus on the best spirometric diagnostic criteria to be used for clinical diagnosis of chronic obstructive pulmonary disease. Failure to resolve the controversy has resulted in inappropriate treatments for many patients. This study aims to shed light on the debate by analyzing data 4,882 adults aged 40 years and older participating in the Canadian Cohort of Obstructive Lung Disease study, a large, population-based study of lung health.
What This Study Found Comparing the clinical relevance of differing cutoffs of forced expiratory volume in one second/forced vital capacity (FEV1/FVC) for airflow limitation in COPD, the study found that airflow limitation defined solely by the fixed ratio was inadequate and may misdiagnosis patients with COPD, in particular those with cardiovascular complaints, leaving them at risk for inappropriate or unnecessary treatments. Conversely, a diagnosis of COPD established by low FEV1/FVC by fixed ratio and/or by lower limit of normal, coupled with a low FEV1 (<80 percent from predicted) was strongly associated with adverse clinical outcomes.
Implications
- The authors conclude that guidelines should be reconsidered to require both spirometry abnormalities in order to reduce overdiagnosis of COPD.
Annals Journal Club
Jan/Feb: Using Spirometry to Appropriately Diagnose COPD
The Annals of Family Medicine encourages readers to develop a learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club and sharing the results of your discussions in the Annals online discussion for the featured articles. RADICAL is an acronym for Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. The word radical also indicates the need to engage diverse participants in thinking critically about important issues affecting primary care and then acting on those discussions.1
HOW IT WORKS
In each issue, the Annals selects an article or articles and provides discussion tips and questions. We encourage you to take a RADICAL approach to these materials and to post a summary of your conversation in our online discussion. (Open the article online and click on "TRACK Discussion: Submit a comment.") You can find discussion questions and more information online at: http://www.AnnFamMed.org/site/AJC/.
CURRENT SELECTION
Article for Discussion
- van Dijk W, Tan W, Li P, et al. Clinical relevance of fixed ratio vs lower limit of normal of FEV1/FVC in COPD: patient-reported outcomes from the CanCOLD cohort. Ann Fam Med. 2015;13(1):41-48.
Discussion Tips
This article analyzes data from the cross-sectional phase of a population-based cohort study in Canada to examine the clinical relevance of different combinations of spirometry criteria for diagnosing chronic obstructive pulmonary disease (COPD). The study considers the impact of misdiagnosis of COPD while exploring diagnostic criteria and the relationship to clinically relevant disease.
Discussion Questions
- What question is asked by this study and why does it matter?
- How does this study advance beyond previous research and clinical practice on this topic?
- How strong is the study design for answering the question?
- What other modifying factors may be important to consider?
- To what degree can the findings be accounted for by:
- How patients were selected, excluded, or lost to follow-up?
- How the main variables were measured--both the diagnostic criteria and the outcome variables?
- Confounding (false attribution of causality because 2 variables discovered to be associated actually are associated with a 3rd factor)?
- Chance?
- How the findings were interpreted?
- What are the main study findings?
- How comparable is the study sample to similar patients in your practice? What is your judgment about the transportability of the findings?
- What contextual factors are important for interpreting the findings?
- How might this study change your practice? Policy? Education? Research?
- Who the constituencies are for the findings, and how they might be engaged in interpreting or using the findings?
- What are the next steps in interpreting or applying the findings?
- What might be the financial impact of this study's results?
- What researchable questions remain?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals Journal Club: It's time to get RADICAL. Ann Fam Med. 2006;4(3):196-197 http://annfammed.org/content/4/3/196.full.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Symptoms of COPD in the absence of airflow obstruction are more indicative of pre-COPD than overdiagnosis
- Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary
- Reply: The new ERS/ATS standards on lung function test interpretation: some extant limitations
- Accuracy and cost-effectiveness of different screening strategies for identifying undiagnosed COPD among primary care patients (>=40 years) in China: a cross-sectional screening test accuracy study: findings from the Breathe Well group
- How different are COPD-specific patient reported outcomes, health status, dyspnoea and respiratory symptoms? An observational study in a working population
- Rate of normal lung function decline in ageing adults: a systematic review of prospective cohort studies
- Use of the terms "overdiagnosis" and "misdiagnosis" in the COPD literature: a rapid review
- Comparison of different staging methods for COPD in predicting outcomes
- Office Spirometry in Primary Care for the Diagnosis and Management of COPD: National Lung Health Education Program Update
- The impact of different spirometric definitions on the prevalence of airway obstruction and their association with respiratory symptoms
- Overdiagnosis of COPD: precise definitions and proposals for improvement
- Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report: GOLD Executive Summary
- GOLD criteria overestimate airflow limitation in one-third of cases in the general Finnish population
- Lung function, forced expiratory volume in 1 s decline and COPD hospitalisations over 44 years of follow-up
- Chronic obstructive pulmonary disease: missed diagnosis versus misdiagnosis
- In This Issue: Policy and Practice