
Abstract
BACKGROUND We evaluated the effectiveness of a structured family-based cardiovascular health promotion intervention model in improving weight management among adults.
METHODS We conducted an open label, cluster randomized controlled trial (ClinicalTrials.gov NCT02771873) with families serving as the unit of intervention. Families were randomly assigned via computer-generated numbers to receive either the comprehensive package of interventions or enhanced usual care in a 1:1 ratio. Nonphysician health workers delivered the comprehensive package of interventions, which included annual screening for cardiovascular risk factors, structured lifestyle modification sessions, referral to a primary health care facility for individuals with established risk factors, and active follow-up to evaluate self-care adherence. Weight, body mass index (BMI), and waist circumference were measured at baseline, 1 year, and 2 years to assess the intervention’s effect on weight management. We used a generalized estimating equation model to analyze the between-group population average changes in these anthropometric parameters.
RESULTS In total, 1,671 participants (1,111 women) from 750 families participated. The mean age of the study population was 40.8 (SD = 14.2) years. The attrition rate at the 2-year follow-up was 3%. The adjusted population average change attributable to the intervention at the 2-year follow-up were −2.61 kg in weight (95% CI, −3.95 to −1.26; P <.001), −1.06 kg/m2 in BMI (95% CI, −1.55 to −0.58; P <.001), and −4.17 cm in waist circumference (95% CI, −5.38 to −2.96; P <.001).
CONCLUSION The reduction in weight achieved in the family-based intervention could have a substantial public health impact in preventing future diabetes and other noncommunicable disease conditions.
INTRODUCTION
Obesity, a high-priority sustainable development concern worldwide, poses a substantial risk to the long-term health and welfare of people and the planet. Despite the availability of multiple paths and strategies for addressing obesity and the importance of managing obesity risk to achieve the sustainable development targets of reducing premature mortality from noncommunicable diseases,1 obesity remains a public health challenge. Globally, obesity is estimated to be present in 1.9 billion adults.2 Furthermore, high body mass index (BMI) was associated with 4.7 million deaths and 148 million disability-adjusted life years lost in 2017.3 Global health policy- and decision-makers, however, often fail to prioritize interventions to reduce obesity at the population level.
In India, an estimated 135 million people are obese.4 The recent National Family Health Survey-5 indicates an increase in the prevalence of obesity in most of the states and union territories of India.5 Obesity rates among adults vary from 15% to 27% in different regions.6 Furthermore, the Global Burden of Disease study estimates suggest a more than twofold increase in obesity prevalence from 1990 to 2016 in India.7 Although the obesity pandemic is still in early stages in India when compared with other high-income countries,8 lack of focus on managing the rising obesity prevalence at the population level will increase the noncommunicable disease burden on the already strained public health system,9 and result in a substantial rise in death and illness during productive life years.
Obesity risk management strategies often focus on individual-level approaches like calorie restriction, lifestyle modifications, pharmacotherapy, and surgery.10-12 While these methods are effective in high-income settings, family-based interventions have also shown promise in reducing obesity and related health risks.13 Family-based interventions often target the entire family environment to promote healthier behaviors. The effectiveness of such strategies in low- and middle-income countries, however, remains largely unexplored. The PROgramme of Lifestyle Intervention in Families for Cardiovascular risk reduction (PROLIFIC Study) was a cluster randomized controlled trial conducted in India to assess the effectiveness of family-based interventions in promoting cardiovascular health.14 We present the secondary outcomes of the PROLIFIC study related to weight management (ie, weight, BMI, and waist circumference).
METHODS
Study Design and Participants
The PROLIFIC trial evaluated the efficacy of a family-based integrated cardiovascular risk management intervention in reducing cardiovascular risk among individuals with a family history of premature coronary heart disease. The detailed study protocol13 and the primary outcome results14 were published elsewhere.
Family members of individuals with premature coronary heart disease were invited to participate in the PROLIFIC trial. The trial included immediate family members (ie, siblings, children, parents, spouses) of persons diagnosed with coronary heart disease before the age of 55 years. To ensure accurate diagnosis, we reviewed medical records and angiogram reports of the index individual. We included adults aged 18 years or older, and excluded bedridden and terminally ill family members. A family with fewer than 2 eligible members was also excluded from the trial (Figure 1). Written informed consent was obtained from all the eligible family members.

The Trial Flow Diagram
CHD = coronary heart disease.
The trial recruitment was conducted from January 1, 2015 to April 30, 2017. Data collection occurred at baseline and annually during the study for 2 years.
The Institutional Ethics Committee of Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum (SCT/IEC/706-2015) approved the study.
Randomization
Each family, serving as the unit of intervention, was randomly assigned to either the treatment intervention group (ie, integrated cardiovascular disease risk management) or the enhanced usual care group (ie, 1-time counseling and annual screening for risk factors) using computer-generated random numbers at a 1:1 ratio. Randomization was performed after baseline data collection from all eligible participants in the selected families. An independent person generated and maintained the randomization codes using a simple random procedure. The trial was not blinded, and study personnel revealed the study group allocated to the participants after randomization. Annual assessments included all baseline measurements and were conducted by independent research nurses (also not blinded) at 1 year and 2 years.
Data Collection Tool
We used an interviewer-administered questionnaire. The questionnaire was adapted from the World Health Organization’s STEPwise approach to surveillance (WHO STEPS) survey tool. It captured data on demographic and socioeconomic variables, general health status, diet patterns, physical activity, tobacco use, and alcohol consumption. The questionnaire was administered at baseline, and repeated at 1 year and 2 years. Anthropometric measurements were performed according to the WHO STEPS protocol and included measurements of height, weight, and waist circumference.
Intervention Group Activities
The study used the community’s existing health care infrastructure to administer structured lifestyle interventions and offer care coordination at the family level.14 Trained nonphysician health workers (NPHWs), mainly accredited social health activists from the family’s region, delivered the interventions. Initially, we provided a 2.5-day training session to all NPHWs involved in the study. The training focused on enhancing interpersonal communication and encouraging family discussions on healthier choices for coronary heart disease risk reduction. All NPHWs in the study also attended 1-day refresher training sessions every 6 months. The study team developed a pocket-size manual in the local language which all NPHWs received for quick reference.
Nonphysician health workers visited their assigned families once every 2 months for the first year. In the second year, however, the frequency was increased to once a month. The comprehensive package of interventions included screening for and detecting cardiovascular risk factors, discussing lifestyle alternatives, and making recommendations to improve cardiovascular health in families. The recommendations were based on the baseline risk profile of the participants and established family habits.14 All participants in the intervention group received a customized health diary. During each family visit, the NPHW used the health diary to set lifestyle goals for the next 1-2 months. The lifestyle goals included: (1) increasing the intake of locally available and seasonal fruits and vegetables to 400-500 g or 4-5 servings per day; (2) reducing the average daily intake of salt per person to less than one-fourth tablespoon; (3) reducing the intake of free sugar to less than 2 tablespoons per day; (4) increasing daily exercise time (mostly walking) to 30-60 minutes; and (5) abstinence from tobacco products and alcohol. The goals were set based on mutual consultation and agreement with other family members.
The set goals for each participant were reviewed during subsequent visits. Those who achieved the goals in their previous visit were encouraged to continue the same strategies during the subsequent visits. Success stories were also shared with those who could not reach their goals. The NPHWs involved all the family members in detailed discussion while reviewing the lifestyle goals. All families in the intervention group received a recipe book in the second year. The recipe book provided healthier alternatives to everyday food items based on the typical Kerala diet for breakfast, lunch, and dinner. The NPHWs used this recipe book to explain the healthier dietary options during home visits. The PROLIFIC study interventions are fully described using by the Template for Intervention Description and Replication (TIDieR) Checklist and detailed in the main study publication.15
The NPHWs facilitated 2-3 peer group sessions for individuals with established chronic conditions (eg, diabetes, hypertension), so they could share their experience in adopting healthier options by changing the family processes. The study team repeated all baseline assessments at both follow-up visits.
Obesity Outcome Measures
The main outcome measurements were anthropometric indicators of obesity (ie, weight, BMI, and waist circumference). Measurements taken at baseline, 1 year, and 2 years were included in the analysis. Height was measured in centimeters using a stadiometer Seca 213 (seca GmbH & Co KG) scale accurate to 0.1 cm. Weight was measured in kilograms using digital weighing scales (Seca HN 286) accurate to 0.1 kg. The measurements were taken while the participant stood still without footwear, with 1 foot on each side of the scale, facing forward, and arms at their side. Body mass index was calculated as body weight divided by the square of body height (eg, kg/m2). Waist circumference was measured around the abdomen at the level of the iliac crest at the end of a normal expiration. A nonelastic measuring tape recorded it to the nearest 0.1 cm (Seca 201).
Statistical Analysis
We summarized demographic data by intervention group, using means and standard deviations for continuous data and frequencies and percentages for categorical data. We analyzed the obesity outcome variables using a statistical model based on the generalized estimating equations (GEE) framework for clustered data. The population average between-group difference in the outcome variables over the 2 years was evaluated. The study had more than 80% power to detect between-group mean differences of 2 kg in weight, 1 kg/m2 BMI, and 2 cm in waist circumference. The power was calculated for a 2-sided test with an α of 0.05 and a ρ or intra-cluster correlation coefficient of 0.10. We introduced an exchangeable working correlation matrix and robust standard errors in estimating average effect size after adjustment for age, sex, and education status. Furthermore, Gaussian family distribution and identity link functions were introduced. All the GEE models to estimate the effect size included a variable for the treatment group and its interaction with follow-up time. All quantitative analyses were done using STATA version 16.1 (StataCorp).
RESULTS
Characteristics of the Study Population
The selection process and recruitment are detailed in previous publications.14 Only 2 of 980 index patients and their families declined participation in the study (Figure 1). Inadequate documentation to support the diagnosis of premature coronary heart disease was the main reason for exclusion (n = 199). Furthermore, in 29 patients, the diagnosis was made more than a year ago. Ultimately, 750 families agreed to participate in the trial. These families were then randomly divided into 2 groups: the intervention group had 368 families with 825 participants, and the usual care group had 382 families with 846 participants. At the 2-year follow-up, 807 of the 825 intervention group participants were available; of these, 805 had complete outcome data for the analysis. In the usual care group, 822 were available.
Most of the participants in the trial were women (1,111; 66.5%) (Table 1). The mean age of the study population was 42.0 years in the intervention group and 40.6 years in the usual care group. The mean years spent in school were 13.2 years in the intervention group and 13.5 years in the usual care group. Nearly one-half of the participants in the trial reported a monthly family income of more than 10,000 Indian rupees. The proportion of smokers among male participants was 7.84% in the intervention group and 7.88% in the usual care group. The baseline socio-demographic characteristics and obesity measurements were marginally different between the intervention and control groups.
Baseline Characteristics of the Study Population (N = 1,671)
Intervention Delivery and Reach
The NPHWs for the trial conducted a median of 13 visits to every family of the intervention group in 2 years. Many families had multiple participants, each participant attended an average of 12 sessions during the study period (all family members were not available during all the intervention sessions).
All families in the intervention group set health goals and documented them in their diaries with support from their NPHWs. At the individual level, 811 of the 825 participants in the intervention group set health goals at least once during the study period. Furthermore, 712/825 participants reviewed their health goals 3 times during the study. Overall, 634 participants in the intervention group achieved at least 1 health goal, and 425 achieved all of their health goals.
Anthropometric Measurements
Body Weight
The mean body weight at baseline was similar in both groups (ie, 65.5 kg intervention; 65.3 kg control). Over the study period, the mean weight in the intervention group decreased while body weight in the control group increased (Table 2). At 2 years, the population average between-group difference in body weight attributable to the interventions after adjustment for clustering and baseline socio-economic characteristics was −2.60 kg (95% CI, −3.95 to −1.26; P <.001).
Changes in Anthropometric Measures
Body Mass Index
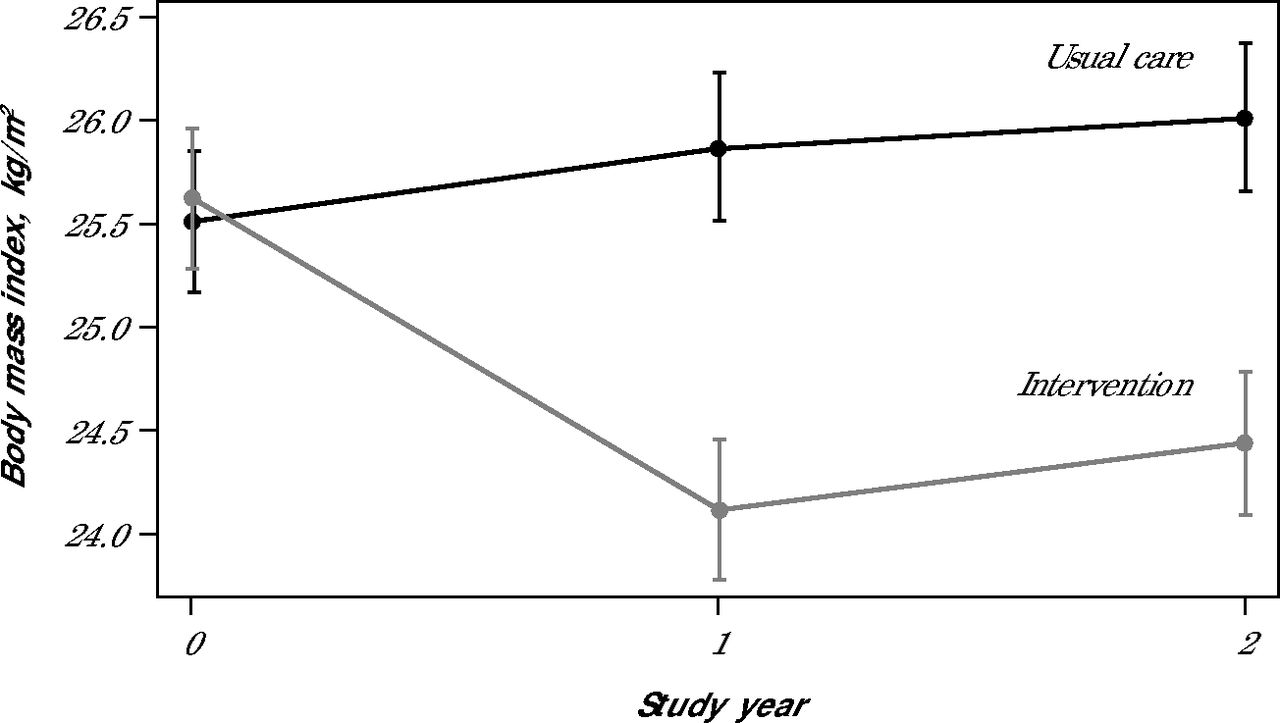
The mean BMI at baseline was similar in both the groups (ie, 25.7 kg/m2 intervention; 25.5 kg/m2 control). Over the study period, the mean BMI of the intervention group decreased while BMI in the control group increased (Table 2). At 2 years, the population average between-group difference in BMI attributable to the interventions was −1.06 kg/m2 (95% CI −1.55 to −0.58; P < .001) after adjustment for clustering and baseline socio-economic characteristics (Figure 2).

Population Average Between-Group Change in Body Mass Index in Intervention and Usual Care Groups
Note: Data was analyzed using a generalized estimating equations model adjusted for clustering at family level, age, sex, and educational status.
Waist Circumference
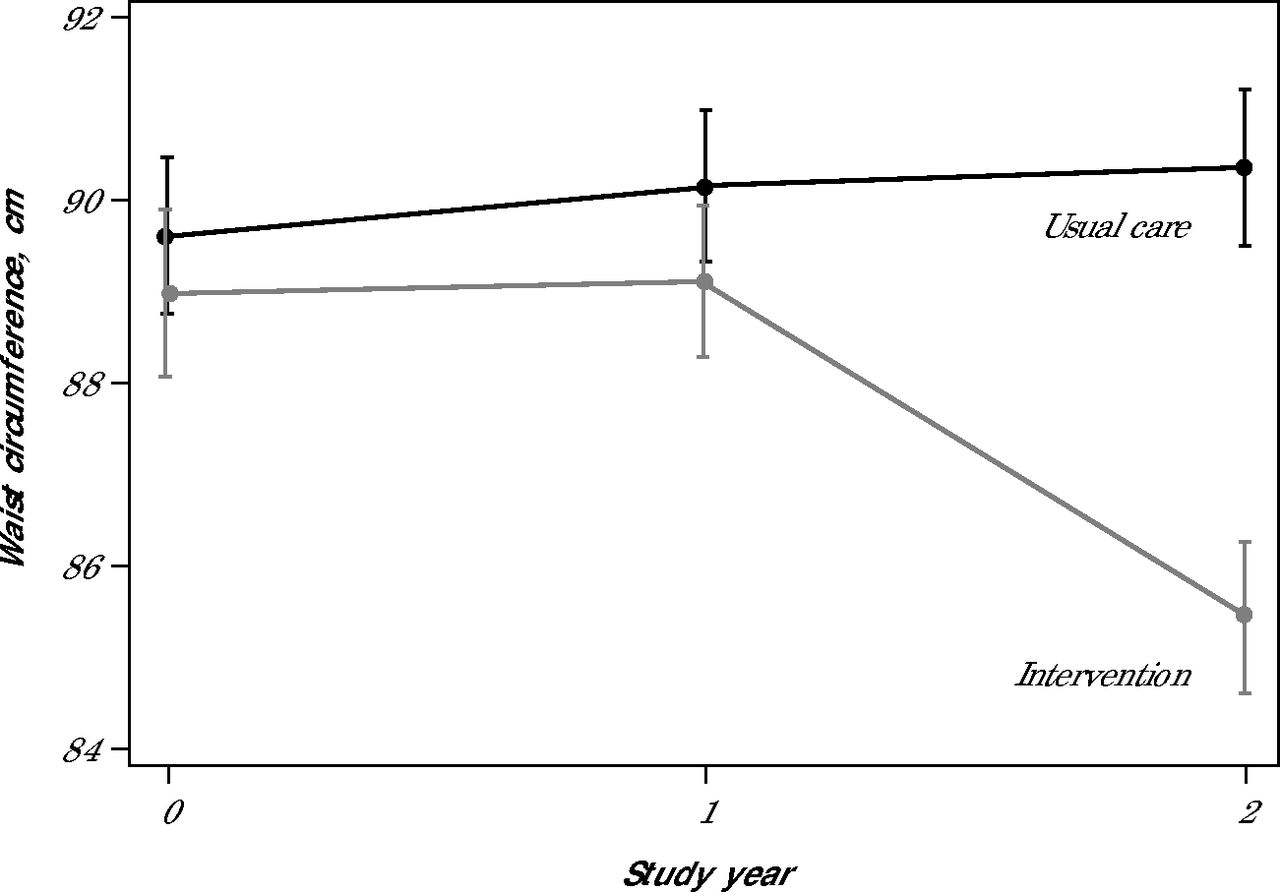
The mean waist circumference at baseline was similar in both the groups (ie, 89.1 cm intervention; 89.5 cm control). Over the study period, the mean waist circumference of the intervention group decreased while it increased in the control group (Table 2). The population average between-group difference in waist circumference at the 2-year follow-up attributable to the interventions (Figure 3) after adjustment for clustering and baseline socio-economic characteristics was −4.17 cm (95% CI, −5.38 to −2.96; P <.001).

Population Average Between-Group Change in Waist Circumference in Intervention and Usual Care Groups
Note: Data was analyzed using a generalized estimating equations model adjusted for clustering at family level, age, sex, and educational status.
DISCUSSION
Our study demonstrated that a family-based cardiovascular risk reduction strategy delivered by frontline health workers as a package of interventions effectively improved weight management in individuals with a family history of premature coronary heart disease. At the end of the 2-year study period, we observed clinically meaningful reductions in body weight, BMI, and waist circumference (a marker of central obesity). The population level decline in anthropometric measures of obesity observed after the interventions in our study can impart substantial public health gain by preventing future diabetes and other chronic noncommunicable disease conditions.
A vast body of evidence supports intentional weight loss for preventing and treating cardiovascular conditions. Reduction in general and central obesity measures, as seen in our study, could avert 25% to 32% of diabetes incidence in high-risk individuals.16,17 Structured lifestyle modification (SLM) interventions are considered more effective than drug interventions in reducing the incidence of diabetes.18 Delaying the onset of diabetes is associated with overall gain in survival. On average, individuals gain 3-4 years in life expectancy by delaying diabetes diagnosis by 1 decade.19 Furthermore, SLM interventions effectively reduce cardiovascular risk factors such as blood pressure and lipid levels.17 Therefore, the benefits to total cardiovascular health could be immense in the long run among individuals adopting SLM interventions.
In high-risk individuals, SLM interventions for diabetes prevention yielded clinically meaningful reductions in BMI and waist circumference.20 The degree of reduction, however, was relatively better in our family-based approach compared with SLM interventions delivered at the individual level. The dose of and adherence to SLM interventions is related to the magnitude of health benefits. Over 2 years, NPHWs made a median of 13 visits per intervention family. Further, 86% of the study participants reviewed their health goals 3 times during the study. This indicates a high level of engagement with and adherence to the interventions. Additionally, a family-based approach may help to improve the sustainability of the changed behavior over a longer period. In our study, we took advantage of family ties and strong bonds between family members to encourage healthier lifestyle decisions at the family level.
In low- and middle-income countries, the family-based strategy for managing adult cardiovascular risk has not been tested. The family has always been at the center of effective intervention by NPHWs, especially in managing maternal and child health conditions in India. The role of NPHWs in fostering a family from the perspective of improving cardiovascular health, however, is not explored in existing national programs. The impact of this intervention model at the population level for the entire population could be tremendous. Over 150,000 Ayushman Bharat Health and Wellness Centres (AB-HWCs) have been operationalized in India.21 The AB-HWCs are an appropriate platform for scaling up family-based interventions with the help of NPHWs, which could significantly affect the population’s ability to prevent and manage chronic conditions.22
The randomized controlled trial design, the intensive nature of the interventions, the high degree of adherence to the intervention delivery plan by the NPHWs, the low attrition rate, and the control of clustering at the family level in the analysis are the major strengths of the study. The randomized controlled trial design and randomization after baseline data collection eliminated selection bias and regression dilution effects. To mitigate the potential for performance bias, we employed several strategies. First, we engaged an independent team of research nurses to conduct outcome assessments at the 1- and 2-year follow-up visits. Second, we relied on objective, standardized measurement tools to minimize the influence of subjective factors on data collection. The study’s other limitations are the exclusion of children, and the exclusive focus on intermediate-level physiologic and behavioral risk factors. In low-resource settings, the intervention’s intensive nature and reliance on a skilled workforce could pose financial challenges. Additionally, the relatively higher educational level of our participants may have influenced the intervention outcomes.
CONCLUSION
Our study demonstrates that a family-based approach can make adopting health promotion interventions easier in high-risk families. The reduction of anthropometric measures of obesity observed after the interventions could have a substantial public health impact in preventing future diabetes and other noncommunicable disease conditions.
Footnotes
Conflicts of interest: P.J. received research grants from: the US National Heart Lung and Blood Institute for a worksite-based cardiovascular risk reduction initiative (R01HL125442-05); the Australian National Health and Medical Research Council (1160283 and 1169766); the World Diabetes Federation (WDF-15-959); the National Institute of Health Care Research; and the Indian Council of Medical Research for diabetes and hypertension risk reduction interventions. All other authors report none.
Author contributions: P.J. conceived the study with guidance from S.H., and S.G. P.J., S.H., S.G., and T.R.L. were involved in the study coordination and supervision of data collection. P.J., A.S., S.H., S.G., and S.I. were involved in data analysis and initial interpretation. All authors critically reviewed the manuscript and approved the final version.
Funding support: The Wellcome Trust/DBT India Alliance supported this study. The study was part of a Clinical and Public Health Intermediate Fellowship to P.J. (IA/CPHI/14/1/501497). The funding agency was not involved in the study design, conduct, data collection, analysis, interpretation, reporting, or manuscript preparation for publication
- Received for publication December 5, 2024.
- Revision received October 15, 2024.
- Accepted for publication October 30, 2024.
- © 2025 Annals of Family Medicine, Inc.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.