
Article Figures & Data
Figures
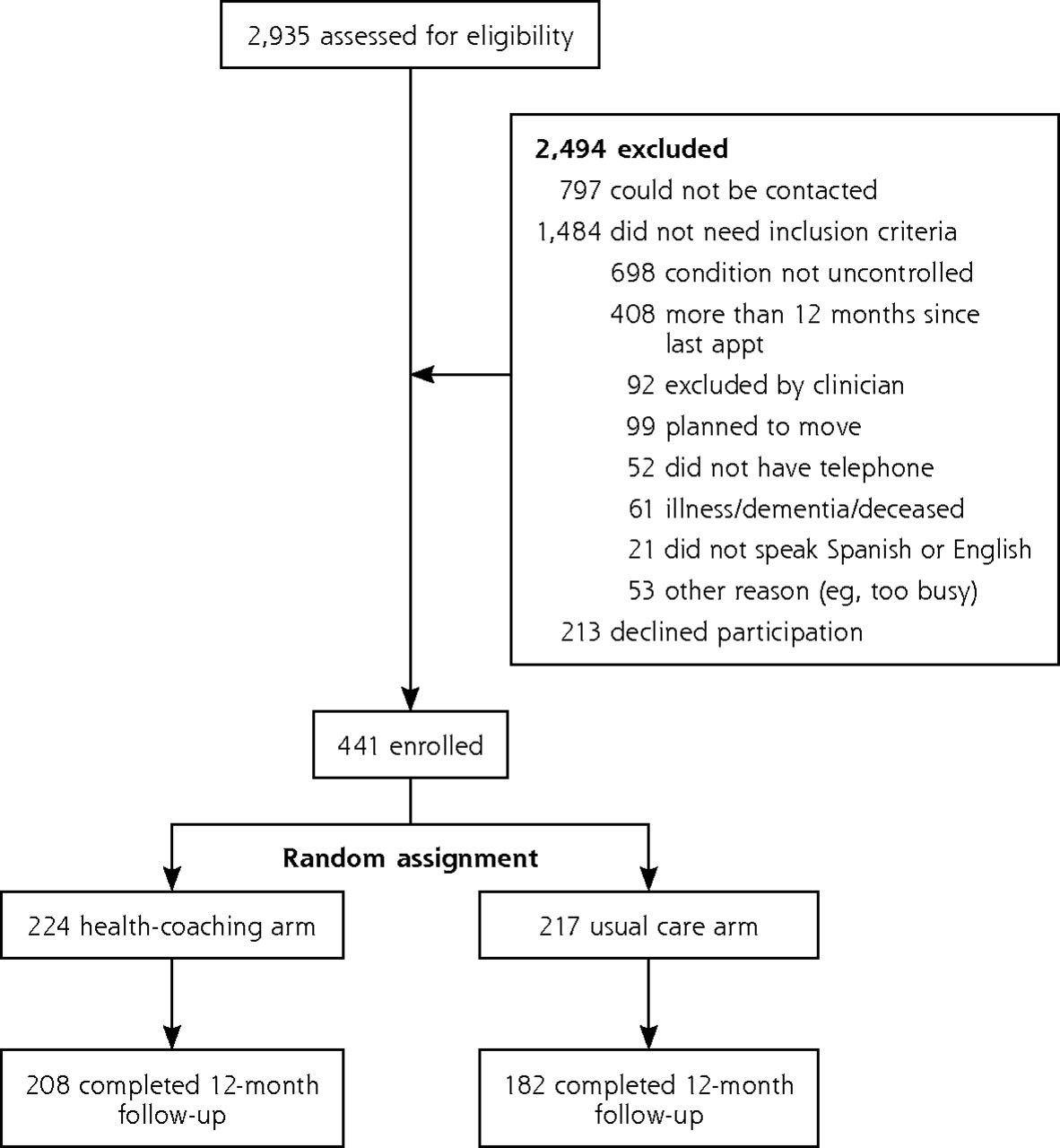
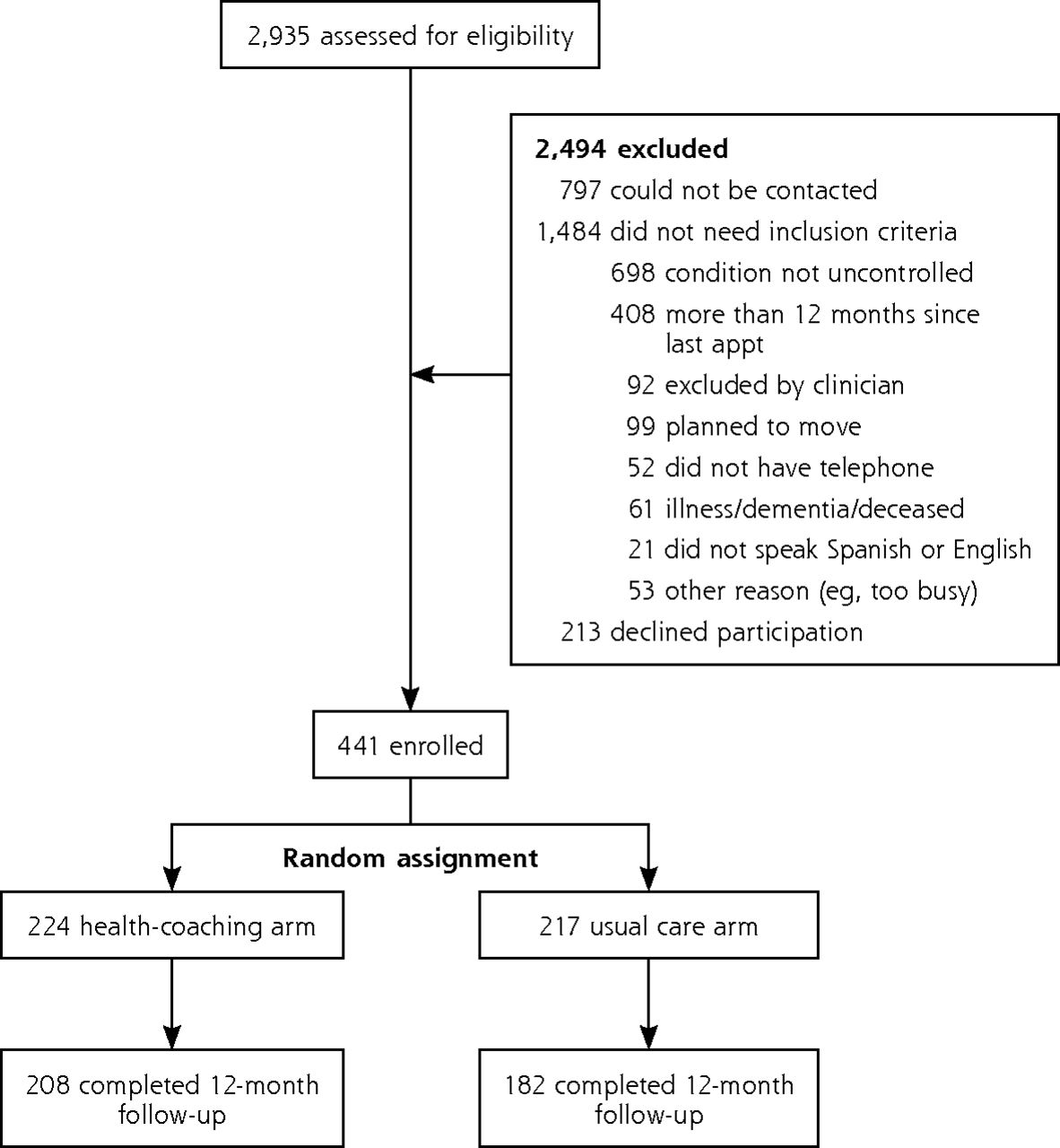
- Figure 1
CONSORT diagram.
appt = appointment; CONSORT = Consolidated Standards of Reporting Trials.
Tables
Collaborative communication Eliciting patient knowledge and motivation Closing the loop (teach back) Setting the agenda Reviewing laboratory numbers Action plans Assessing patient motivations Exploring ambivalence Disease-specific knowledge Basics of study conditions Monitoring control Medication management Medication adherence Assessing patient knowledge and motivation Addressing barriers to adherence Working with primary care clinicians Taking notes during a visit Checking understanding Offering help Advocating for a patient’s agenda Community and clinic resources Behavior health Physical activity and healthy eating Smoking cessation Social determinants of health Characteristic All Participants (N = 441) Study Arm Usual Care (n = 217) Health Coaching (n = 224) Demographic characteristics Clinic site, % (No.) Clinic site A 75.3 (332) 76.0 (165) 74.6 (167) Clinic site B 24.7 (109) 24.0 (52) 25.4 (57) Age, mean (SD), y 52.7 (11.1) 52.9 (11.5) 52.6 (10.7) Sex (female), % (No.) 55.3 (244) 52.2 (127) 58.5 (117) Married/long-term relationship, % (No.) 53.1 (234) 57.1 (124) 49.1 (110) Born in the United States, % (No.) 25.6 (113) 24.9 (54) 26.3 (59) Years in United States, mean (SD)a 18.2 (11.2) 17.9 (11.9) 18.5 (10.4) Primary language, % (No.) English 27.7 (122) 26.7 (58) 28.6 (64) Spanish 68.7 (303) 69.5 (151) 67.9 (152) Other 3.6 (16) 3.7 (8) 3.6 (8) Race/ethnicity, % (No.) Asian 4.1 (18) 5.1 (11) 3.1 (7) African American 19.0 (84) 18.4 (40) 19.6 (44) Latino or Hispanic 70.1 (309) 71.0 (154) 69.2 (155) White 2.5 (11) 2.3 (5) 2.7 (6) Other 4.3 (19) 3.2 (7) 5.4 (12) Working status, % (No.) Full time 18.6 (82) 16.1 (35) 21.0 (47) Part time 25.6 (113) 26.3 (57) 25.0 (56) Homemaker 13.8 (61) 17.1 (37) 10.7 (24) Unemployed 16.1 (71) 16.1 (35) 16.1 (36) Retired/disabled/SSI/other 25.9 (114) 24.3 (53) 27.2 (61) Education, % (No.) ≤5th grade 22.7 (100) 23.1 (50) 22.3 (50) 6th to 8th grade 21.1 (93) 20.7 (45) 21.4 (48) Some high school 13.4 (59) 12.4 (27) 14.3 (32) High school graduate or GED 17.7 (78) 16.6 (36) 18.8 (42) Some college 15.6 (69) 19.4 (42) 12.1 (27) College graduate 9.5 (42) 7.8 (17) 11.2 (25) Income, % (No.) ≤$5,000 34.0 (150) 31.3 (68) 36.6 (82) $5,000–$10,000 24.3 (107) 25.3 (55) 23.2 (52) $10,000–$20,000 29.5 (130) 29.0 (63) 29.9 (67) ≥$20,000 12.2 (54) 14.2 (31) 10.2 (23) Number of PCP visits in year before study, mean (SD) 5.4 (3.9) 5.5 (4.3) 5.4 (4.1) Clinical characteristics BMI, mean (SD), kg/m2 31.4 (6.7) 31.4 (6.3) 31.5 (7.0) HbA1c, mean (SD), %b 9.9 (1.5) 10.0 (1.4) 9.8 (1.5) LDL cholesterol, mean (SD), mg/dLb 147.0 (35.6) 147.8 (34.1) 146.3 (36.9) SBP, mean (SD), mm Hgb 159.4 (15.4) 160.9 (16.8) 157.7 (13.5) Uncontrolled at baseline, % (No.) For 1 condition 72.6 (320) 73.3 (159) 71.9 (161) For 2 conditions 23.6 (104) 23.5 (51) 23.7 (53) For 3 conditions 3.9 (17) 3.2 (7) 4.5 (10) For HbA1c 35.8 (158) 33.6 (73) 37.9 (85) For SBP 43.5 (192) 46.5 (101) 40.6 (91) For cholesterol 51.9 (229) 49.8 (108) 54.0 (121) -
BMI = body mass index; GED = general equivalency diploma; HbA1c = hemoglobin A1c; LDL = low-density lipoprotein; PCP = primary care provider; SBP = systolic blood pressure; SSI = supplemental security income.
-
↵a For the 328 participants born outside the United States.
-
↵b Includes only patients qualifying for the study on this measure (158 for HbA1c, 218 for LDL, and 192 for SBP).
-
Characteristic All Participants (N = 441) Clinic Site Clinic Site A (n = 332) Clinic Site B (n = 109) P Value Demographic characteristics Age, mean (SD), y 52.7 (11.1) 52.3 (11.3) 54.0 (10.5) .18 Sex (female), % (No.) 55.3 (244) 53.3 (177) 61.5 (67) .14 Born in the United States, % (No.) 25.6 (113) 6.0 (20) 85.3 (93) <.001 Primary language, % (No.) <.001 English 27.7 (122) 7.8 (26) 88.1 (96) Spanish 68.7 (303) 89.5 (297) 5.5 (6) Other 3.6 (16) 2.7 (9) 6.4 (7) Race/ethnicity, % (No.) <.001 Asian 4.1 (18) 3.3 (11) 6.4 (7) African American 19.0 (84) 1.8 (6) 71.6 (78) Latino or Hispanic 70.1 (309) 90.7 (30) 7.3 (8) White 2.5 (11) 1.5 (5) 5.5 (6) Other 4.3 (19) 2.7 (9) 9.2 (10) Working status, % (No.) <.001 Full time 18.6 (82) 22.0 (73) 8.3 (9) Part time 25.6 (113) 28.0 (93) 18.3 (20) Homemaker 13.8 (61) 16.9 (56) 4.6 (5) Unemployed 16.1 (71) 13.6 (45) 23.9 (26) Retired/disabled/SSI/other 25.9 (114) 19.5 (65) 44.9 (49) Education, % (No.) <.001 ≤5th grade 22.7 (100) 29.6 (98) 1.8 (2) 6th to 8th grade 21.1 (93) 27.1 (90) 2.8 (3) Some high school 13.4 (59) 11.1 (37) 20.2 (22) High school graduate or GED 17.7 (78) 14.2 (47) 28.4 (31) Some college 15.6 (69) 9.9 (33) 33.0 (36) College graduate 9.5 (42) 8.1 (27) 13.8 (15) Income, % (No.) .52 ≤$5,000 34.0 (150) 33.7 (112) 34.9 (38) $5,000–$10,000 24.3 (107) 23.8 (79) 25.7 (28) $10,000–$20,000 29.5 (130) 31.0 (103) 24.8 (27) ≥$20,000 12.2 (54) 11.4 (38) 14.7 (16) Clinical characteristics BMI, mean (SD), kg/m2 31.4 (6.7) 30.6 (4.7) 34.0 (10.2) <.001 HbA1c, mean (SD), %a 9.9 (1.5) 9.8 (1.4) 10.3 (1.9) .17 LDL cholesterol, mean (SD), mg/dLa 147.0 (35.6) 147.3 (36.7) 145.2 (28.9) .75 SBP, mean (SD), mm Hga 159.4 (15.4) 158.3 (13.5) 160.9 (17.5) .25 Number of PCP visits in year before study, mean (SD) 5.4 (4.1) 5.2 (3.5) 6.1 (5.5) <.05 Number of coach interactions, mean (SD) 12.4 (7.4) 14.1 (6.7) 7.6 (7.2) <.001 Total time interaction, mean (SD), min 540.8 (307.6) 621.1 (281.1) 305.5 (258.7) <.001 Number of interactions by topic/activity addressed, mean (SD) Medications 9.3 (6.0) 11.0 (5.4) 4.1 (4.6) <.001 Reviewing clinical values and goals 7.4 (4.6) 8.4 (3.9) 4.5 (5.2) <.001 Discussing lifestyle changes 7.4 (5.0) 9.1 (4.3) 2.1 (2.2) <.001 Agenda setting 5.7 (4.3) 7.1 (4.1) 1.7 (1.9) <.001 Navigational support 5.1 (5.1) 6.4 (5.3) 1.5 (1.8) <.001 Action plans for behavior change 4.2 (3.2) 5.1 (2.9) 1.6 (2.3) <.001 Facilitating communication with PCP 3.3 (3.8) 4.0 (4.1) 1.1 (1.5) <.001 Closing the loop (teach back) 5.3 (3.6) 6.1 (3.3) 2.8 (3.4) <.001 Patient-reported quality of health-coaching interactions, mean (SD)b 3.3 (0.7) 3.4 (0.5) 2.8 (0.9) <.001 Patient-reported trust in health coach, mean (SD)c 4.1 (0.5) 4.1 (0.5) 3.9 (0.7) <.005 -
BMI = body mass index; GED = general equivalency diploma; HbA1c = hemoglobin A1c; LDL = low-density lipoprotein; PCP = primary care physician; SBP = systolic blood pressure; SSI = supplemental security income.
-
↵a Includes only patients qualifying for the study on this measure (158 for HbA1c, 218 for LDL cholesterol, and 192 for SBP).
-
↵b On a scale of 1 to 5, where 5 = best.
-
↵c On a scale of 1 to 5, where 5 = high.
-
- Table 4
Primary Composite and Condition-Specific Outcomes by Study Arm, for Total Sample and by Clinic Site
Outcome Health Coaching, % (No./n) Usual Care, % (No./n) Difference, % (95% CI) P Value Total sample Composite (primary)a 46.4 (90/194) 34.3 (57/166) 12.1 (2 to 23) .02 Composite (secondary)b 34.0 (66/194) 24.7 (41/166) 9.3 (1 to 19) .05 HbA1c goal achievedc 48.6 (36/74) 27.6 (16/58) 21.0 (5 to 39) .01 Cholesterol goal achievedd 42.7 (41/96) 32.0 (24/75) 10.7 (−4 to 25) .15 SBP goal achievede 23.8 (19/80) 28.9 (22/76) −5.1 (−9 to 19) .46 Clinic site A Composite (primary)a 49.7 (73/147) 32.8 (42/128) 16.9 (5 to 29) .01 Composite (secondary)b 36.1 (53/147) 24.2 (31/128) 11.9 (1 to 23) .03 HbA1c goal achievedc 52.3 (34/65) 29.4 (15/51) 22.9 (5 to 41) .01 Cholesterol goal achievedd 41.8 (33/79) 25.4 (16/63) 16.4 (1 to 32) .04 SBP goal achievede 25.5 (12/47) 31.9 (15/47) −6.4 (−11 to 25) .49 Clinic site B Composite (primary)a 36.2 (17/47) 39.5 (15/38) −3.3 (−17 to 24) .76 Composite (secondary)b 27.7 (13/47) 26.3 (10/38) 1.4 (−18 to 20) .89 HbA1c goal achievedc 22.2 (2/9) 14.3 (1/7) 7.9 (−31 to 46) .69 Cholesterol goal achievedd 47.1 (8/17) 66.7 (8/12) −19.6 (−18 to 56) .29 SBP goal achievede 21.2 (7/33) 24.1 (7/29) −2.9 (−18 to 24) .78 -
HbA1c = hemoglobin A1c; HDL = high-density lipoprotein; LDL = low-density lipoprotein; SBP = systolic blood pressure.
-
Note: Analyses used missing-at-random (nonimputed) data. See statistical analysis in Methods section for details.
-
↵a Achieved target for control of 1 or more of specific conditions for which patient was uncontrolled at baseline.
-
↵b Achieved target for control of all conditions for which patient was uncontrolled at baseline.
-
↵c Goal was <8.0%.
-
↵d Goal for diabetic patients was LDL cholesterol <100 mg/dL or non–HDL cholesterol <130 mg/dL if triglycerides >400 mg/dL, and for nondiabetic patients was LDL cholesterol l<130 mg/dL or non–HDL cholesterol <160 mg/dL if triglycerides >400 mg/dL.
-
↵e Goal was <130 mm Hg for diabetic patients and <40 mm Hg for nondiabetic patients.
-
- Table 5
Secondary Condition-Specific Outcomes by Study Arm, for Total Sample and by Clinic Site
Outcome Health Coaching Usual Care Difference Between Arms (95% CI) P Value n Baseline, Mean (SD) 12 Months, Mean (SD) DIM n Baseline, Mean (SD) 12 Months, Mean (SD) DIM Total sample HbA1c, % 74 9.8 (1.5) 8.6 (2.0) −1.2 58 9.9 (1.4) 9.4 (2.0) −0.5 −0.7 (−1.4 to 0.0) .06 LDL, mg/dL 95 147.2 (36.3) 119.3 (52.8) −27.9 73 143.4 (33.2) 125.4 (39.1) −18.1 −9.8 (−21.6 to 2.0) .10 SBP, mm Hg 80 157.3 (13.8) 148.7 (16.5) −8.6 76 160.5 (16.4) 150.3 (18.2) −10.2 1.6 (−7.6 to 4.4) .59 Clinic site A HbA1c, % 65 9.8 (1.5) 8.5 (2.0) −1.3 51 9.8 (1.4) 9.3 (2.0) −0.6 −0.7 (−1.4 to −0.0) .04 LDL, mg/dL 79 148.2 (38.3) 122.6 (55.1) −25.6 62 145.0 (35.0) 130.5 (37.6) −14.5 −11.1 (−23.9 to 1.7) .09 SBP, mm Hg 47 154.9 (10.5) 144.8 (12.5) −10.0 47 160.5 (15.1) 148.5 (18.9) −12.0 2.0 (−5.1 to 9.0) .59 Clinic site B HbA1c, % 9 10.2 (1.4) 9.5 (2.1) −0.7 7 10.5 (1.5) 10.1 (1.7) −0.5 −0.2 (−2.9 to 2.5) .89 LDL, mg/dL 16 142.8 (29.4) 103.6 (37.8) −39.2 11 136.9 (29.2) 98.6 (36.9) −38.4 −0.8 (−31.3 to 29.6) .96 SBP, mm Hg 33 160.7 (15.8) 154.1 (19.9) −6.6 29 160.6 (19.2) 153.2 (17.0) −7.4 0.8 (−10.0 to 11.6) .88 -
DIM = difference in means; HbA1c = hemoglobin A1c; LDL = low-density lipoprotein; SBP = systolic blood pressure.
-
Note: Analyses used missing-at-random (nonimputed) data. See statistical analysis in Methods section for details.
-
The Article in Brief
Health Coaching by Medical Assistants to Improve Control of Diabetes, Hypertension, and Hyperlipidemia in Low-Income Patients: A Randomized Controlled Trial
Rachel Willard-Grace , and colleagues
Background Health coaching can give people with chronic illnesses the knowledge, skills, and confidence to manage their conditions. This study tests the effectiveness of health coaching by medical assistants to improve indicators of health among low-income patients with uncontrolled diabetes, high blood pressure, and high cholesterol levels.
What This Study Found Health coaching by medical assistants is a promising way to improve indicators of health for people with common chronic conditions. In this study, almost twice as many patients who received health coaching achieved their diabetes goals. At the larger study site, health coached patients were more likely to achieve their cholesterol goals. There was no significant difference in the proportion of patients meeting their blood pressure goals.
Implications
- Medical assistants can successfully serve as health coaches to improve health indicators for some common chronic conditions.
- The medical assistant health coaching model may help solve barriers of time, resources and cultural concordance faced by many primary care practices seeking to implement self-management support.
Annals Journal Club
Mar/Apr: Impact of Medical Assistants as Health Coaches
The Annals of Family Medicine encourages readers to develop a learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club and sharing the results of your discussions in the Annals online discussion for the featured articles. RADICAL is an acronym for Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. The word radical also indicates the need to engage diverse participants in thinking critically about important issues affecting primary care and then acting on those discussions.1
HOW IT WORKS
In each issue, the Annals selects an article or articles and provides discussion tips and questions. We encourage you to take a RADICAL approach to these materials and to post a summary of your conversation in our online discussion. (Open the article online and click on "TRACK Discussion: Submit a comment.") You can find discussion questions and more information online at: http://www.AnnFamMed.org/site/AJC/.
CURRENT SELECTION
Article for Discussion
- Willard-Grace R, Chen EH, Hessler D, et al. Health coaching by medical assistants to improve control of diabetes, hypertension, and hyperlipidemia in low-income patients: a randomized controlled trial. Ann Fam Med. 2015;13(2):130-138.
Discussion Tips
This article investigates the impact of in-clinic health coaching by medical assistants using data from a randomized controlled trial of low-income patients in safety net primary care clinics in San Francisco. The study considers the effectiveness of this model on control of hemoglobin A1c, systolic blood pressure, and LDL cholesterol and explores potential factors in implementation.
Discussion Questions
- What question is asked by this study and why does it matter?
- How does this study advance beyond previous research and clinical practice on this topic?
- How strong is the study design for answering the question?
- How well does the study follow the CONSORT guidelines? (www.consort-statement.org)
- To what degree can the findings be accounted for by:
- How patients were selected, excluded, or lost to follow-up?
- How the main variables were measured?
- Confounding (false attribution of causality because 2 variables discovered to be associated actually are associated with a 3rd factor)?
- Chance?
- How the findings were interpreted?
- "Contamination" between intervention and control groups? How might this possibility be avoided in the study design?
- What are the main study findings?
- How comparable is the study sample to similar patients in your practice? What is your judgment about the transportability of the findings?
- What contextual factors are important for interpreting the findings? How strong are the methods for assessing contextual factors affecting implementation?
- How might this study change your practice? Policy? Education? Research?
- What might be the financial impact of implementing a similar model? At what level do the costs accrue? At what level are the benefits likely to appear over time? (eg patient, practice, health care system, community?)
- What other in-clinic interventions may lead to similar results?
- Who the constituencies are for the findings, and how they might be engaged in interpreting or using the findings?
- What are the next steps in interpreting or applying the findings?
- What researchable questions remain?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals Journal Club: It's time to get RADICAL. Ann Fam Med. 2006;4(3):196-197 http://annfammed.org/content/4/3/196.full.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Primary Care Practice Characteristics Associated With Medical Assistant Staffing Ratios
- Effectiveness of non-pharmacological strategies in the management of type 2 diabetes in primary care: a protocol for a systematic review and network meta-analysis
- Lay Health Coaching to Increase Appropriate Inhaler Use in COPD: A Randomized Controlled Trial
- Advanced practice nurses, registered nurses and medical practice assistants in new care models in Swiss primary care: a focused ethnography of their professional roles
- Making Inroads in Addressing Population Health in Underserved Communities With Type 2 Diabetes
- Barriers and Facilitators to Expanding Roles of Medical Assistants in Patient-Centered Medical Homes (PCMHs)
- Delivery of Health Coaching by Medical Assistants in Primary Care
- A Qualitative Study of How Health Coaches Support Patients in Making Health-Related Decisions and Behavioral Changes
- What Happens After Health Coaching? Observational Study 1 Year Following a Randomized Controlled Trial
- Impact of Medical Assistants as Health Coaches
- In This Issue: Developing and Amplifying the Effectiveness of the Primary Care Workforce