
Article Figures & Data
Figures
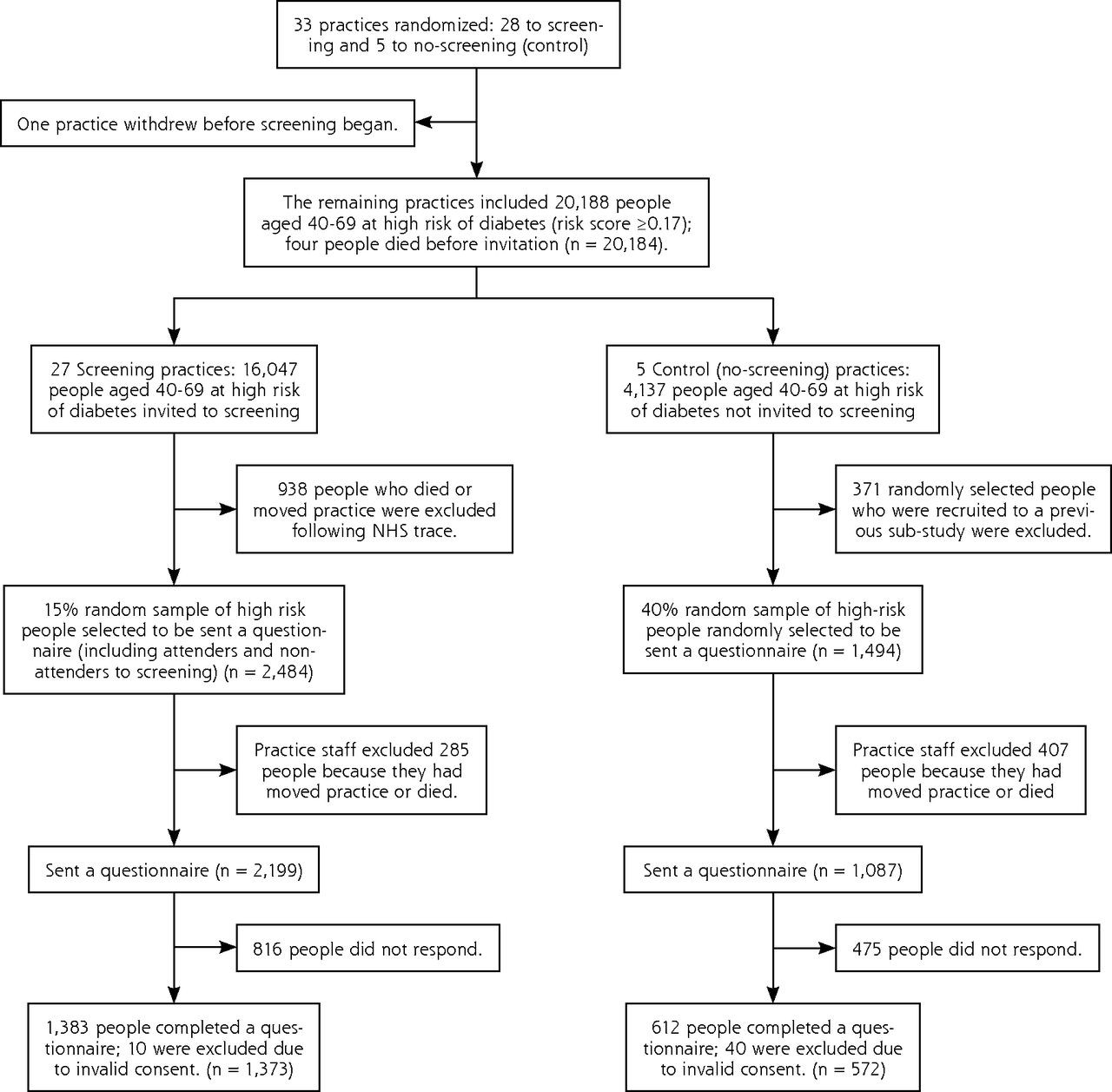
- Figure 1
Practice and participant flow in the ADDITION-Cambridge diabetes screening trial.
Tables
- Table 1
Baseline Practice and Patient Characteristics in the ADDITION-Cambridge Screening Trial; Data are Median (Inter-quartile Range) Unless Otherwise Indicated
Screening Group No-Screening Control Groupa Practices n = 27 n = 5 Practice list size 6,610 (5,144–9,966) 8,827 (8,694–10,986) Crude prevalence of diabetes, % 2.9 (2.5–3.5) 3.2 (3.0–3.4) Physician full-time equivalents 3.5 (2.5–5.0) 4.5 (4.0–5.0) Index of Multiple Deprivation scoreb 11.7 (6.9–11.6) 15.7 (9.1–15.7) Participants n = 1,373 n = 572 Age, years 60 (54–65) 60 (54–65) Men, n (%) 839 (61.1) 360 (62.9) BMI, kg/m2 29.4 (27.7–32.3) 29.6 (27.8–32.2) Cambridge diabetes risk score 0.36 (0.25–0.52) 0.38 (0.25–0.56) Prescribed anti-hypertensive medication, n (%) 654 (47.6) 298 (52.1) Prescribed steroids, n (%) 68 (5.0) 17 (3.0) -
BMI = body mass index.
-
↵a There were no statistically significant differences between groups.
-
↵b The Index of Multiple Deprivation combines a number of indicators, chosen to cover a range of economic, social and housing issues, into a single deprivation score for each small area in England. This allows each area to be ranked relative to one another according to their level of deprivation. A high Index of Multiple Deprivation score indicates a high level of deprivation.
-
- Table 2
Impact of Screening on Cardiovascular Morbidity and the Prescription of Cardioprotective Drugs in the ADDITION-Cambridge Trial at 7-year Follow-up
Screening Group No-screening Control Group Odds Ratio (95%CI)a Cardiovascular morbidity, n (%) Self-reported cardiovascular eventsb 142 (12.4) 67 (13.5) 0.90 (0.71–1.15) Self-reported hypertension 809 (60.9) 352 (63.4) 0.90 (0.75–1.08) Self-reported dyslipidemia 502 (41.2) 254 (48.3) 0.75 (0.64–0.88) Prescribed medication, n (%) Antihypertensive drugs 853 (72.5) 369 (74.7) 0.89 (0.73–1.10) ACE inhibitors 546 (46.4) 244 (49.4) 0.89 (0.75–1.06) Lipid lowering drugs 507 (43.1) 244 (49.4) 0.78 (0.63–0.95) Antiplatelet drugs 335 (28.5) 185 (37.5) 0.67 (0.53–0.83) Glucose lowering drugs 97 (8.3) 48 (9.7) 0.84 (0.57–1.21) - Table 3
Impact of Screening on Self-rated Health Status and Self-reported Health Behaviors in the ADDITION-Cambridge Trial at 7-year Follow-up
Screening Group No-screening Control Group Intervention Effect (95%CI)a Self-rated health status Mean SF-8 physical health summary score (scale 0 to 100), score (SD) 47.4 (9.8) 47.8 (10.3) −0.33 (−1.80 to 1.14) Mean SF-8 mental health summary score (scale 0 to 100), score (SD) 51.8 (8.6) 52.2 (8.1) −0.38 (−1.33 to 0.57) Mean EQ-5D score (scale −0.3 to 1.0), score (SD) 0.87 (0.16) 0.87 (0.15) 0.002 (−0.02 to 0.02) Mean EuroQol visual acuity score (scale 0 to 100), score (SD) 74.5 (16.5) 73.7 (17.2) 0.80 (−1.28 to 2.87) Self-reported health behavior Current smoker, n (%) 143 (10.5) 61 (10.7) 0.97 (0.72–1.32) Alcohol consumption (units per week), mean (SD) 8.2 (11.9) 8.1 (11.1) 0.14 (−1.07 to 1.35) 1 or more portions fresh fruit per day, n (%) 627 (46.4) 249 (43.8) 1.11 (0.93–1.33) 1 or more portions green leafy vegetables per day, n (%) 339 (25.2) 117 (20.7) 1.28 (0.99–1.66) 1 or more portions other vegetables per day, n (%) 382 (28.5) 142 (25.1) 1.19 (0.99–1.43) 5 or more portions oily fish per week, n (%) 27 (2.1) 10 (1.8) 1.14 (0.61–2.11) 5 or more portions meat products per week, n (%) 104 (7.8) 51 (9.1) 0.84 (0.64–1.11) 1 or more portions whole meal (brown) bread per day, n (%) 414 (30.8) 167 (29.9) 1.04 (0.89–1.22) Total physical activity (MET-hours per week), mean (SD) 45.1 (51.3) 44.6 (51.9) 0.50 (−4.08 to 5.07) Vigorous activity (MET-hours per week), mean (SD) 16.2 (31.7) 15.3 (32.5) 0.89 (−2.09 to 3.86) Walking activity (MET-hours per week), mean (SD) 22.6 (21.1) 21.2 (21.0) 1.35 (−1.17 to 3.86) Sedentary time (hours per day), mean (SD) 5.3 (2.7) 5.4 (2.8) −0.11 (−0.32 to 0.09) Number of hospital admissions in past 3 months, mean (SD) 0.11 (0.37) 0.13 (0.44) 0.85 (0.58–1.25)b Number of family physician consultations in past 3 months, mean (SD) 1.1 (1.3) 1.2 (1.5) 0.93 (0.78–1.12)b Number of nurse consultations in past 3 months, mean (SD) 0.8 (1.7) 0.8 (1.7) 1.04 (0.79–1.36)b -
SF-8 = 8-item short form health survey; EQ-5D = EuroQual measure of health outcome; MET = Metabolic equivalents of physical activity.
-
↵a Beta coefficients (95% CI) for continuous outcomes (representing the mean difference between groups) and odds ratios (95% CI) for categorical outcomes, accounting for clustering by general practice.
-
↵b Negative binomial regression (appropriate for over-dispersed count data) was used to compare the number of hospital admissions, family physician consultations, and nurse consultations. The effect sizes can be interpreted as ratios of incidences.
-
The Article in Brief
Long-Term Effect of Population Screening for Diabetes on Cardiovascular Morbidity, Self-Rated Health, and Health Behavior
Simon J. Griffin , and colleagues
Background Many organizations recommend population screening for diabetes. This study assesses the long-term effects of such screening.
What This Study Found At the population level, screening high risk individuals for diabetes appears to have limited impact on cardiovascular disease, self-rated health status and health behavior. In a study of 18,875 individuals aged 40 to 69 years at high risk of diabetes, 2.9 percent of those eligible for screening were diagnosed with diabetes. After seven years, there were no significant differences between the screening and control groups in terms of reported heart attack or stroke, self-rated health status, physical activity, smoking status or alcohol consumption. Diabetes screening did not have a negative effect on self-rated functional status or health utility and did not lead to unhealthy behaviors due to false reassurance or to an increase in health service use.
Implications
- The authors see no long-term beneficial effect of screening for type 2 diabetes at the population level. They conclude that a single round of screening may be associated with benefits among the minority whose previously undiagnosed diabetes is detected, but it appears unlikely to affect the health of the population as a whole.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Development and validation of a diabetes mellitus and prediabetes risk prediction function for case finding in primary care in Hong Kong: a cross-sectional study and a prospective study protocol paper
- An Interrupted Time Series Analysis to Determine the Effect of an Electronic Health Record-Based Intervention on Appropriate Screening for Type 2 Diabetes in Urban Primary Care Clinics in New York City
- Long term impact of screening for type 2 diabetes mellitus - a commentary on new evidence
- In This Issue: Developing and Amplifying the Effectiveness of the Primary Care Workforce