
Abstract
The purpose of this quasi-experimental design study was to examine the effectiveness of the behavioral health Screening, Brief Intervention, and Referral to Treatment (SBIRT) program at a community health center. The study group was twice as likely (25.3%) to have depression and substance abuse diagnosed compared with the control group (11.4%) (P <.001). Referral rates for the study group were more likely to occur (12.4%) compared with referral rates for the control group (1.0%) (P <.001); however, the kept appointment rates by patients for behavioral health problems referrals remained low for both groups. SBIRT was effectively utilized in a community health center, resulting in increased rates for diagnosis of behavioral health problems and referrals of patients.
INTRODUCTION
Although problems related to mental health and substance abuse are major social and public health concerns associated with sizable individual and social costs,1,2 these conditions remain underdiagnosed in primary care settings.3,4
Despite screening recommendations for depression and substance abuse, few studies have examined the efficacy of screening in community health centers.5 The purpose of this study is to examine the effectiveness of the Screening, Brief Intervention, and Referral to Treatment (SBIRT) program in a federally qualified community health center (FQHC) as prescribed by the Substance Abuse and Mental Health Services Administration (SAMHSA).
METHODS
Using a quasi-experimental design, we undertook a prospective, continuous quality improvement study of a screening program for behavioral health by evaluating outcome data.
The research hypothesis considered whether using the SBIRT screening process would result in improved identification of medical patients who might require intervention, referral, and treatment for the key indicators of depression, alcohol abuse, and substance abuse when compared with similar patients in a control setting.
Specifically, the study setting involved the Ohio North East Health Systems (ONE Health), a FQHC operating 6 primary care facilities in northeast Ohio. ONE Health draws from a target population in which more than 90% are at or below 200% of the federal poverty level.6
To compare the effectiveness of implementing SBIRT in this setting, we selected 2 facilities operated by ONE Health: the Youngstown Health Center was designated as the intervention site, and the Warren Health Center was chosen as the control site. Both facilities are in urban settings and are federally designated as medically underserved and health professional service areas. The sites serve a predominantly low-income population in which uninsured Medicaid and Medicare patients make up 85.5% of the medical users at the intervention site and 86.8% at the control site.
Before SBIRT implementation, the medical and clerical staff at the Youngstown Health Center received 3 educational sessions to learn about the SBIRT concept, referral process, and screening tools, and to develop motivational interviewing skills. Training sessions were conducted with the support of the Institute for Research, Education and Training in Addictions (http://ireta.org/). Clinicians were not given a participation incentive, but were updated on data collection and effectiveness of the program. The Warren Health Center maintained its standard practices of relying on clinicians’ discretion of behavioral health matters. For referrals we established off-site behavioral health partnerships with local mental health and substance abuse clinicians. Behavior health clinicians were not given a participation incentive, but they were updated on data collection and effectiveness of the program; they were unaware, however, of the nature of any ongoing studies. The Warren Health Center maintained its standard practices of relying on clinicians’ discretion with regard to evaluation, intervention, and referrals of behavioral health matters.
During the study period (February through August 2013), 2,482 medical patients, aged 18 years and older, were screened for depression, alcohol, and substance use. The screening tool, consisting of 5 dichotomous questions adapted from the Oregon Health & Science University’s SBIRT program,7 was introduced as a vital sign and added to the routine intake process. Screening was self-administered. Those eliciting positive responses were given appropriate, quanitifiable standardized tests: the Drug Abuse Screening Test (DAST), Alcohol Use Disorders Identification Test (AUDIT), and the Patient Health Questionnaire (PHQ-9). Results were recorded in the electronic health record (EHR) Next Gen Automated EHR (http://www.nextgen.com) and if indicated by a standardized recommendation scale, clinicians performed a brief intervention, made a behavioral health referral, and/or initiated pharmacotherapy. All activities were recorded and documented in the EHR.
Data Analysis
Summary data were collected from the EHR through specific fields for the various steps of SBIRT. Data collection included patient demographics; dichotomous screening results; a diagnosis of depression, alcohol, or substance abuse; and provider intervention. Additional data included the number of referrals made to behavioral health specialists and appointments kept by patients referred for subsequent treatment. We used Pearson χ2 tests to compare outcome measures across the control and intervention sites within the ONE Health system.
RESULTS
During the 6-month study period, 2,761 eligible patient visits occurred at the intervention site, and 2,482 patients self-administered the SBIRT screening tool (90%). Also during this period 1,685 comparable patients visited the control site and did not participate in the screening. Differences between uninsured Medicare and Medicaid patients at the 2 sites were not significant.
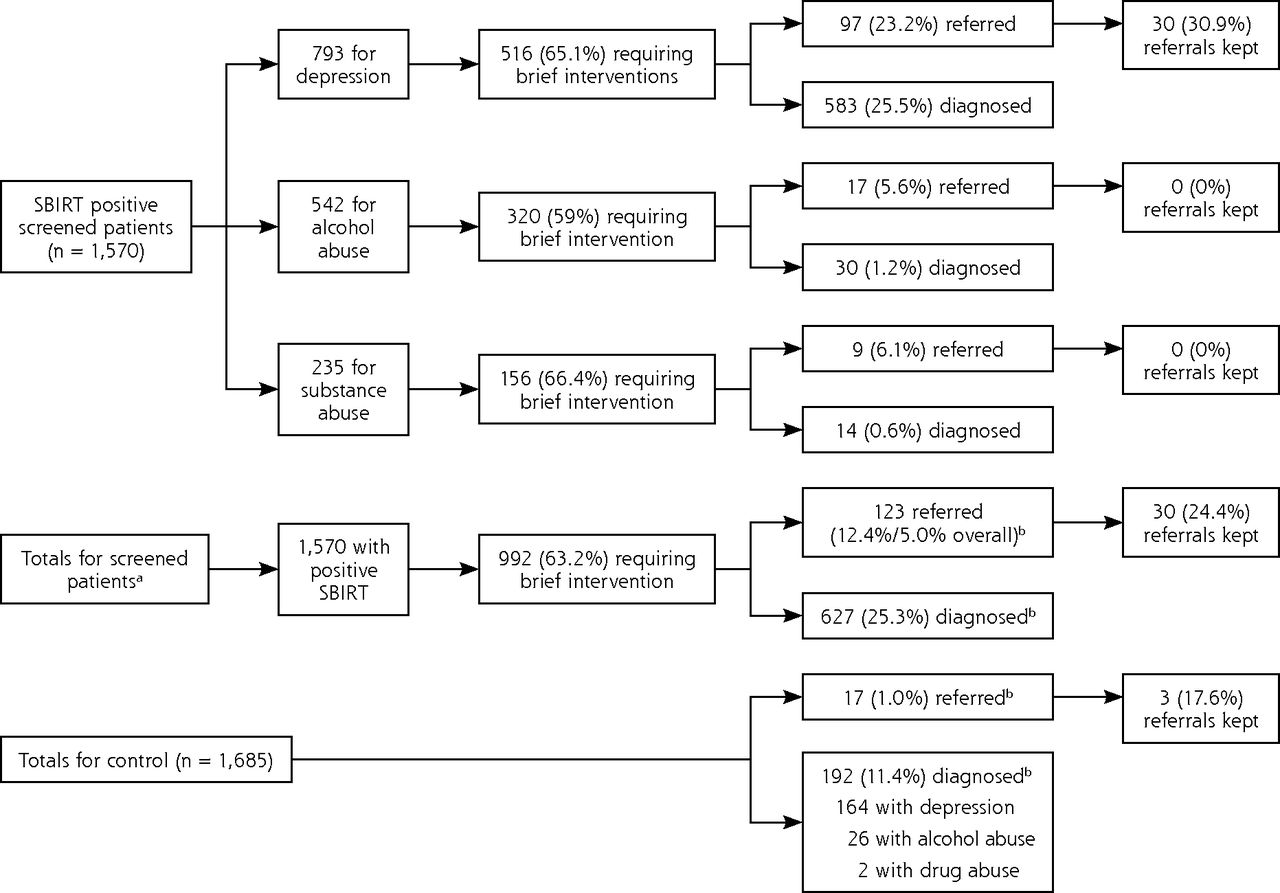
Figure 1 provides results for the 2 sites. Compared with 11.4% of the control site patients, 25.3% of the SBIRT intervention site patients had positive findings for depression, alcohol, or substance use (P <.001). Referral rates for treatment and counseling at the test site significantly exceeded the rates for the control site (12.4% vs 1.0%, respectively; P <.001). Kept referral appointment rates of 24.4% for the intervention site and 17.6% for the control site were similar.
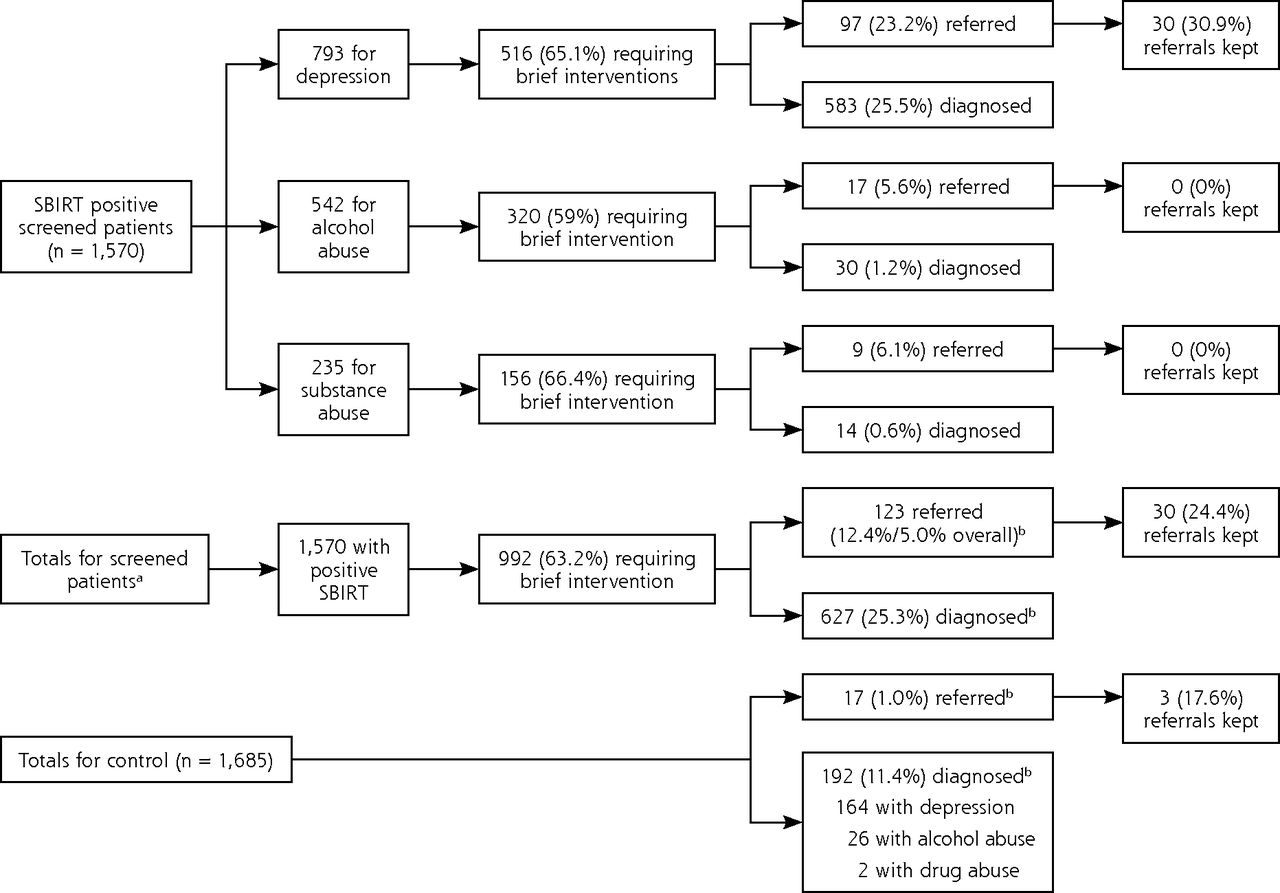
SBIRT intervention: brief interventions and referrals by type of screening.
SBIRT = Screening, Brief Intervention, and Referral for Treatment.
aOf 2,761 eligible patients; 2,482 patients received the SBIRT screening.
bP <.001 for rate comparison.
DISCUSSION
Results suggest that in a primary outpatient clinic SBIRT is effective in identifying patients at risk for depression, alcohol, and substance use and increasing referrals for patients who are at increased risk. This effect is similar to that found in a variety of clinical settings implementing SBIRT in their practices.8
Although the referral rates were greater at the test site, the rates of kept referral appointments were low at both sites. Because the most common reason for noncompliance is the lack of health coverage,9 provision of an on-site, integrated behavioral health service in an FQHC setting, where sliding fee schedules are available, should improve the kept referral appointment rates.
The study results are encouraging, however findings are limited in that they are based on a quasiexperimental study of the first 6 months of SBIRT implementation at a single community health center so the long-term impact of the findings is not yet known.
Despite these limitations, the findings support a behavioral health-screening program in the primary care setting to improve identification and diagnosis. Although recent reports broadly indicate low efficacy of a brief intervention for drug use found through screening in the primary care setting,10,11 it is still important to identify patients who test positive for behavioral health problems so proper and timely referrals can be made. Additionally, the findings support integration of primary health care with behavioral health services, especially within community health centers, where there are major unmet health needs within the population.12,13 Indeed, the overall lack of effective referrals to outside agencies could be improved with immediate access of behavioral health services and reduced health care costs for poor and uninsured patients.
Footnotes
-
Conflicts of interest: authors report none.
-
Funding support: Provided by the Ohio North East Health Systems, Inc.
- Received for publication July 29, 2014.
- Revision received January 30, 2015.
- Accepted for publication February 14, 2015.
- © 2015 Annals of Family Medicine, Inc.




{kind=link}