
Abstract
PURPOSE Epidemiological studies have identified a trend in the development of depressive and anxiety disorders following a diagnosis of sleep apnea. The relationship between sleep apnea and subsequent panic disorder, however, remains unclear.
METHODS Using a nationwide database, the Taiwan National Health Insurance Research Database, patients with sleep apnea and age-, sex-, income-, and urbanization-matched control patients who did not have sleep apnea were enrolled between 2000 and 2010. Patients with a prior diagnosis of panic disorder before enrollment were excluded. The 2 cohorts were observed until December 31, 2010. The primary endpoint was occurrence of newly diagnosed panic disorder.
RESULTS A total of 8,704 sleep apnea patients and 34,792 control patients were enrolled. Of the 43,496 patients, 263 (0.60%) suffered from panic disorder during a mean follow-up period of 3.92 years, including 117 (1.34%) from the sleep apnea cohort and 146 (0.42%) from the control group. The Kaplan-Meier analysis revealed a predisposition of patients with sleep apnea to develop panic disorder (log-rank test, P <.001). After multivariate adjustment, the hazard ratio for subsequent panic disorder among the sleep apnea patients was 2.17 (95% confidence interval, 1.68–2.81; P <.001).
CONCLUSIONS Sleep apnea appears to confer a higher risk for future development of panic disorder.
INTRODUCTION
Obstructive sleep apnea is a common disorder characterized by repeated episodes of apnea and hypopnea during sleep owing to complete or partial collapse of the upper airway.1 Subsequent to apnea/hypopnea, patients with sleep apnea will be awakened by the resulting hypoxemia so that they can resume breathing. Some patients may awake up feeling like they are choking or suffocating, thereby increasing their sense of stress. In the past decade obstructive sleep apnea has been found to be linked to a variety of cardiovascular diseases, neurocognitive dysfunction, and behavioral disorders.2,3
Patients with sleep apnea may also have substantial comorbid mental disorders, such as depression, anxiety, bipolar disorder, schizophrenia, post-traumatic stress syndrome, and substance abuse.4 Panic disorder is an extreme pole of anxiety disorder with features of recurrent panic attacks. There are, however, few studies addressing the relationship between sleep apnea and panic disorder, and most of these studies are small or lack an appropriate control group.5–9 A crossover study enrolling 12 patients with panic disorder who also had obstructive sleep apnea showed that they benefited from continuous positive airway pressure (CPAP) therapy, which decreased the panic attacks and reduced the use of alprazolam, suggesting an interaction of both diseases.10 We therefore undertook this nationwide population-based study to elucidate the relationship of sleep apnea and subsequent panic disorder.
METHODS
Database
The National Health Insurance (NHI) is a mandatory universal health insurance program that since 1995 provides comprehensive medical service to almost all Taiwanese citizens. The National Health Research Institute in Miaoli (Taiwan) (http://nhird.nhri.org.tw/en) is in charge of the Taiwan NHI program and maintains the entire insurance claims database, namely, the National Health Insurance Research Database (NHIRD). The NHIRD consists of detailed health care data of more than 99% of the entire Taiwan’s 23 million population.11 The data used in this study were retrieved from the Longitudinal Health Insurance Database 2000 (LHID2000), comprised of approximately 1,000,000 randomly sampled persons who were alive in 2000; all the registration files and medical claims for the reimbursement of these individuals were collected from 1995 to 2010. The released database has been validated by the National Health Research Institute to be representative of the whole Taiwanese population11 and is among the largest population-based databases in the world; it is a resource for many published studies in Taiwan.12 Each patient’s personal identifiable information has been encrypted by the National Health Research Institute using a consistent code, allowing linkage of claims belonging to individuals within this database.
Study Sample and Control
The study was exempt from full review by the Institutional Review Board of Taipei Veterans General Hospital because the data sets consisted of de-identified secondary data. In this study, we enrolled adult patients (aged 20 years and older) who had newly diagnosed sleep apnea (International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes 780.51, 780.53, 780.57) during 2000 to 2010 as the study cohort (sleep apnea cohort).13 The date of enrollment was defined as the date when sleep apnea was initially diagnosed. An age-, sex-, monthly income-, and urbanization-matched group of patients who did not have sleep apnea served as the control group and were randomly selected from the same data sets. In both groups, patients with a medical history of panic disorder (ICD-9-CM codes 300.01, 300.21) before enrollment were excluded.
Variables
In this research, general data, such as age, sex, monthly income, and urbanization were retrieved and matched between groups. According to past studies, risk factors for panic disorder14 and major comorbid conditions3 linked to sleep apnea, including hypertension, coronary artery disease, cerebrovascular disease, asthma, chronic obstructive pulmonary disease, chronic kidney disease, dyslipidemia, paralysis, irritable bowel syndrome, mitral valve prolapse, premenstrual syndrome, hyperthyroidism, diabetes mellitus, drug abuse, cancer, bipolar disorder, obsessive-compulsive disorder, depression, phobia, and post-traumatic stress disorder, were assessed in our analyses. The Charlson comorbidity index, representative of baseline comorbidity profile, was also calculated and incorporated into the analysis.15
Matching
The control group of patients without sleep apnea was selected at a ratio of 4 control patients per 1 patient with sleep apnea by means of incidence density sampling.16 The control group was matched for each individual’s age, sex, monthly income, urbanization, and enrollment year. Matching for the age and year of enrollment was allowed within a tolerance range (±1 year). For the control group, the start date of follow-up was defined as the first date of clinical visit to a medical facility in the enrollment year.
Main Outcome Measures
The endpoint of the study was defined as occurrence of panic disorder. All enrollees were observed from the date of enrollment until the first diagnosis of panic disorder or, if they were free of panic disorder, until they died, withdrew from national health insurance, or reached the study end date of December 31, 2010.
Statistical Analysis
Extraction, matching, and computation of data were performed using the Perl programming language (version 5.12.2). A Microsoft SQL Server 2012 (Microsoft Corp) was used for data linkage, processing, and sampling. Statistical analysis was performed using SPSS 18.0 software (SPSS, Inc). All data were expressed as means plus or minus standard deviations or as a percentage unless otherwise stated. Comparison between 2 groups was made by independent Student’s t tests for continuous variables or Pearson’s χ2 test for categorical variables, as appropriate. Survival analysis was performed using the Kaplan-Meier method, with significance based on the log-rank test. A Cox proportional hazard model was used for multivariate adjustment. To better elucidate sleep apnea as a dependent risk factor for panic disorder, we performed multivariate adjustments in 5 different models. The hazard ratios were obtained after adjusting age and sex in model 1 and further adjustment for monthly income, urbanization, and outpatient visits in model 2. In models 3 through 5, additional adjustments were made for psychiatric comorbidities, all comorbidities (as listed in Table 1), and the Charlson comorbidity score. Statistical significance was inferred at a 2-sided P value of <.05.
Demographic and Clinical Characteristics of Patients
RESULTS
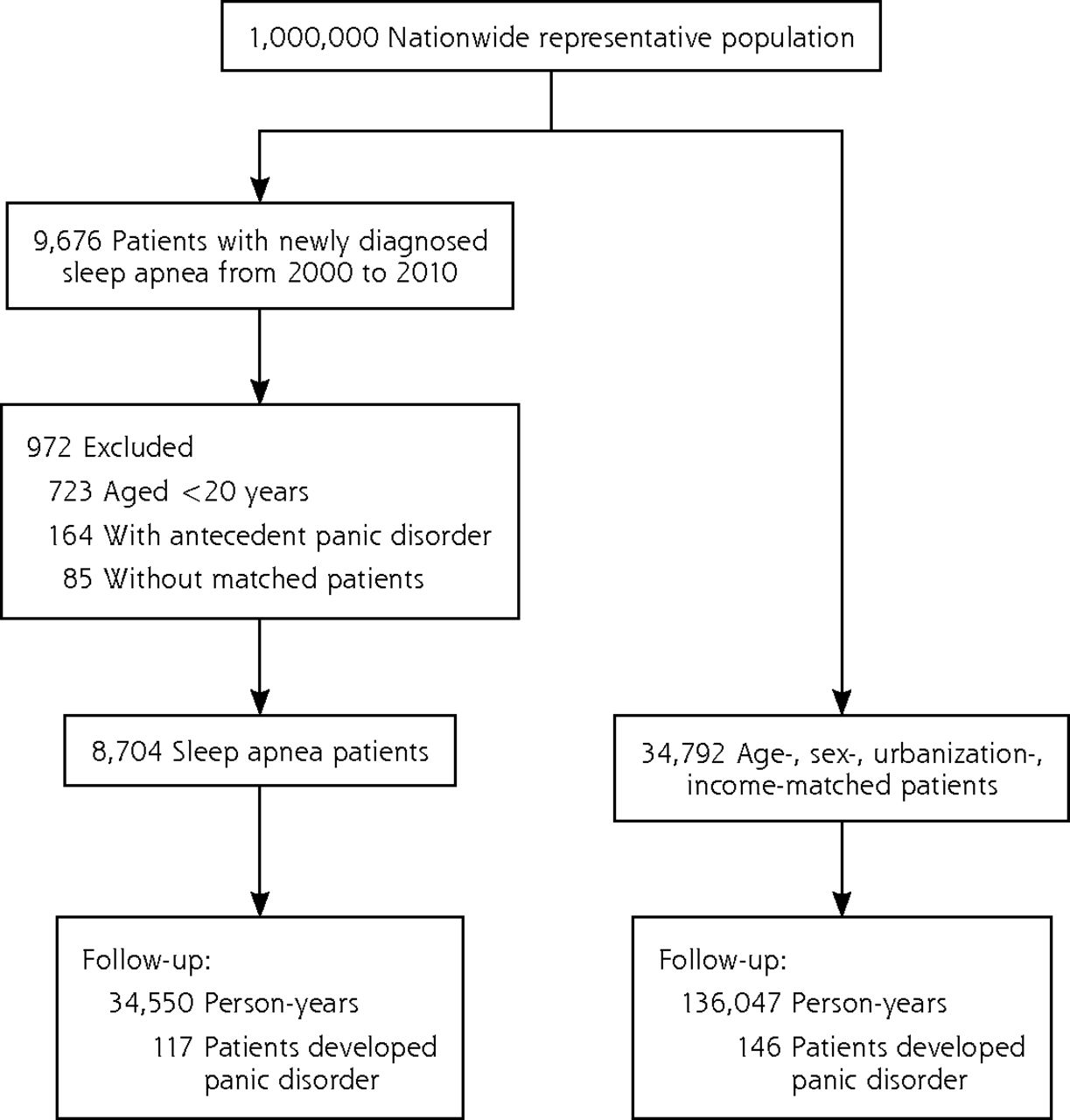
Figure 1 displays a flowchart of enrollment and follow-up. The basic characteristics of the sleep apnea cohort and the control group are shown in Table 1. Compared with the control group, the sleep apnea cohort had higher percentages of comorbidities, higher Charlson comorbidity scores, and more medical visits in the past year. During a mean follow-up period of 3.92 years, there were more panic disorder events among the sleep apnea cohort as compared with the control group (117 [1.34%] vs 146 [0.42%]; P <.001]. Sleep apnea patients had a significantly higher risk for incident panic disorder than the comparison group (log-rank test, P <.001, Figure 2). Incidences in the sleep apnea cohort and the control group were 33.86 and 10.73 persons per 10,000 person-years, respectively (P <.001). Comparing groups with and without panic disorder, those patients with incident panic disorder were predominately female (54.37%) and had a higher percentage of hypertension, coronary artery disease, cerebrovascular disease, asthma, chronic obstructive pulmonary disease, chronic kidney disease, dyslipidemia, irritable bowel syndrome, mitral valve prolapse, hyperthyroidism, diabetes mellitus, bipolar disorder, obsessive-compulsive disorder, depression, and phobia.
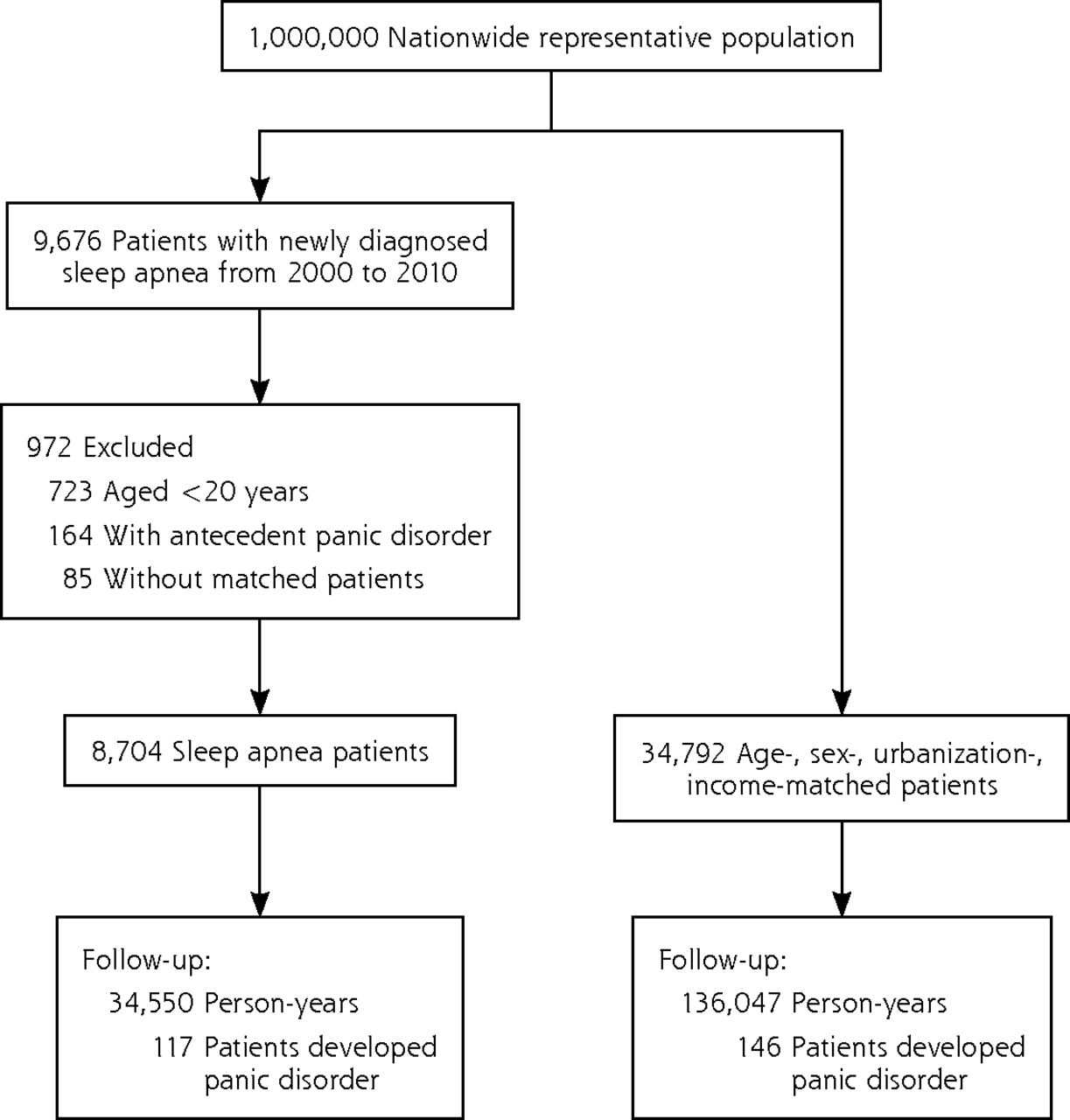
Flow diagram summarizing the process of enrollment and follow-up.
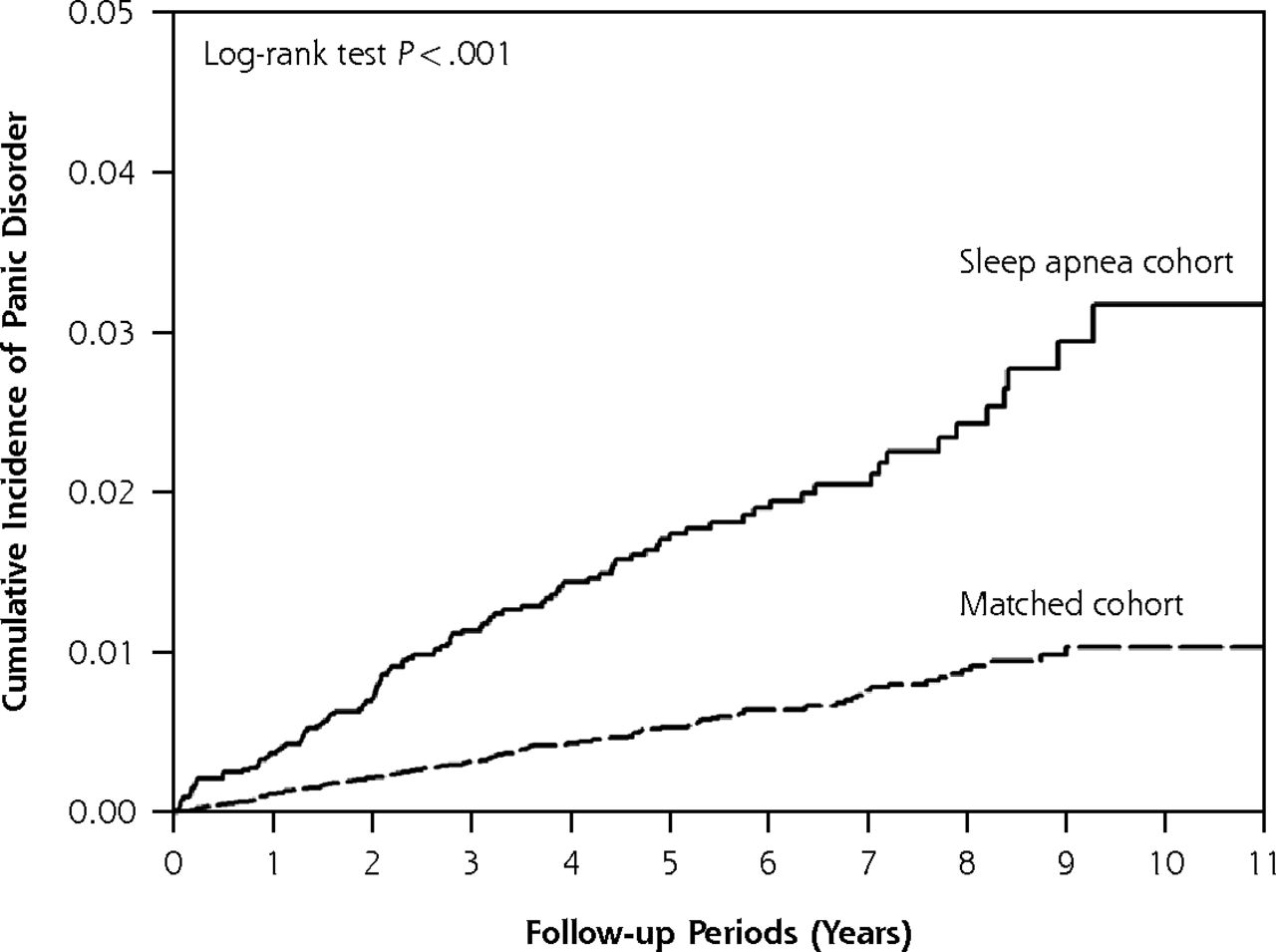
Cumulative incidence of panic disorder in patients with sleep apnea and the matched cohort.
Multivariate analysis in 5 different models consistently indicated that sleep apnea was independently associated with incident panic disorder (Table 2). The fully adjusted hazard ratio in the model 5 was 2.17 (95% CI, 1.68–2.81; P <.001). The subgroup analyses are presented in Figures 3 and 4 of the Supplemental Appendix (http://www.annfammed.org/content/13/4/325/suppl/DC1). It is noteworthy that the hazard ratios of all sleep apnea models were statistically significantly higher in their counterparts devoid of a given comorbidity, suggesting an independent role of sleep apnea in development of panic disorder.
Serial Multivariate Adjustment Showing Sleep Apnea as a Risk Factor for Incident Panic Disorder
DISCUSSION
In this study, we are able to show that sleep apnea is an independent risk factor for incident panic disorder. Considering the linkage of sleep apnea to important health consequences, our findings may further broaden the spectrum of its comorbidities. To our knowledge, this cohort study is the largest probing into this issue. In contrast with other published literature,5–9 this study addressed the temporal relationship between sleep apnea and panic disorder and provided an appropriate control group for comparison as well.
Sleep apnea has been reported to be associated with several mental disorders, including depression, anxiety, posttraumatic stress disorder, psychosis, and bipolar disorders.4,17 Interestingly, psychological symptoms may correlate with the degree of hypoxia in such patients and can be improved after CPAP therapy.18,19 Patients with coexisting sleep apnea and mental disorders responded less well to antipsychotic medications than did those who did not have sleep apnea.20 Thus, identifying patients with overlapping diagnoses of mental disorders and sleep apnea would help to improve their treatment outcomes through more aggressive pharmacotherapy and CPAP therapy.
There have been few studies addressing the relationship of sleep apnea and panic disorder; most were case reports,5–7 one was a cross-sectional study8 and one was a small-scale case-control study,9 which has not allowed for a solid conclusion. Our results, derived from a large-scale database, provide a closer look at the relationship of the 2 disorders. Based on our results, sleep apnea conferred a higher risk for panic disorder, even after a relatively short follow-up period (3.9 years) in an older population (age 47.9 years on average). In a randomized crossover study,10 Takaesu et al has shown that CPAP therapy could significantly reduce the frequency of panic attacks, the panic disorder severity scale score, and the use of alprazolam for panic attack in 12 patients with obstructive sleep apnea and panic disorders.
Given that panic disorder in this population may be attenuated after CPAP treatment, the actual prevalence of panic may be higher than found in our current study, a possibility that may further strengthens our conclusion. Moreover, evidence so far favors the inference that the association between sleep apnea and panic disorder results primarily from an influence in one direction (ie, from a history of sleep apnea to first panic attack). The possibility of a bidirectional relationship between sleep apnea and panic attacks awaits further exploration.
The link between sleep apnea and panic disorder could be explained in several ways. Frequent arousals from sleep (sleep fragmentation), awakening with feelings of choking or suffocating, and daytime sleepiness have been proposed as mechanisms of anxiety in obstructive sleep apnea.21 Additionally, episodes of apnea/hypopnea resulting in intermittent hypoxemia (and possibly hypercapnia) may facilitate oxidative stress-related functional deterioration and central nervous system injury, thereby increasing the risk of panic disorder.22,23 Functional and structural neuroimaging studies show that sleep apnea alters brain structure with time, leading to a decrease in gray matter in the hippocampus, frontal lobe, and the anterior cingulate cortex.24–26 Damage to similar regions are also seen in the patients with panic disorders.27–30 Lastly, hypercapnia may play a role based on the evidence that panic attack can be provoked by inhalation of carbon dioxide.31
The strengths of our study are its nationwide, population-based study design and that all respiratory and psychiatric practices were covered in the database, which allowed us to trace all cases of newly diagnosed sleep apnea and panic disorder. Additionally, the large sample size in our study offered substantial statistical power for detecting real, even subtle, differences between the 2 cohorts. Because participation in the NHI is mandatory, and all Taiwanese can use medical care with low copayment, the follow-up of each patient was completed with the lowest referral bias.
There are several limitations in our study. First, diagnoses of sleep apnea and panic disorder that rely on administrative claims data recorded by physicians or hospitals may be less accurate than diagnoses made in a clinical, prospective setting. Sleep apnea is often underdiagnosed, possibly generating a misclassification bias. Even so, the nondifferential misclassification bias was toward the null; if the misclassification were corrected, then our positive conclusion would be strengthened, that is, our results would be more significant. Alternatively, some patients with panic disorder might not have used health care, either before or after enrollment, and therefore might not have appeared in the claims data sets as having panic disorder, which may provide a source of bias. Second, patients’ body mass index and smoking history, which may affect the propensity to obstructive sleep apnea, were not available in the database. Third, we could not further classify sleep apnea into obstructive type or central type, because the 2001 version of the ICD-9-CM coding did not separate the 2 subtypes of sleep apnea. Even so, obstructive sleep apnea was reported to be the predominant (>90%) type of sleep apnea by Bixler et al,32 which is compatible with the our results (>99%) in a previous study.13 Finally, the external validity of our findings may be a concern because our patients were almost all Taiwanese. Generalization of our results to non-Asian populations needs further verification.
Sleep apnea may be a risk factor for panic disorder. Clinicians should be aware of panic disorder as a comorbid condition in sleep apnea patients. Future prospective research is needed to confirm our finding and elucidate the possible underlying mechanisms.
Footnotes
↵* Vincent Yi-Fong Su and Yung-Tai Chen contributed equally to this manuscript.
Conflicts of interest: authors report none.
Supplementary materials: Available at http://www.AnnFamMed.org/content/13/4/325/suppl/DC1/
- Received for publication November 19, 2014.
- Revision received November 22, 2015.
- Accepted for publication May 22, 2015.
- © 2015 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}