
Article Figures & Data
Figures
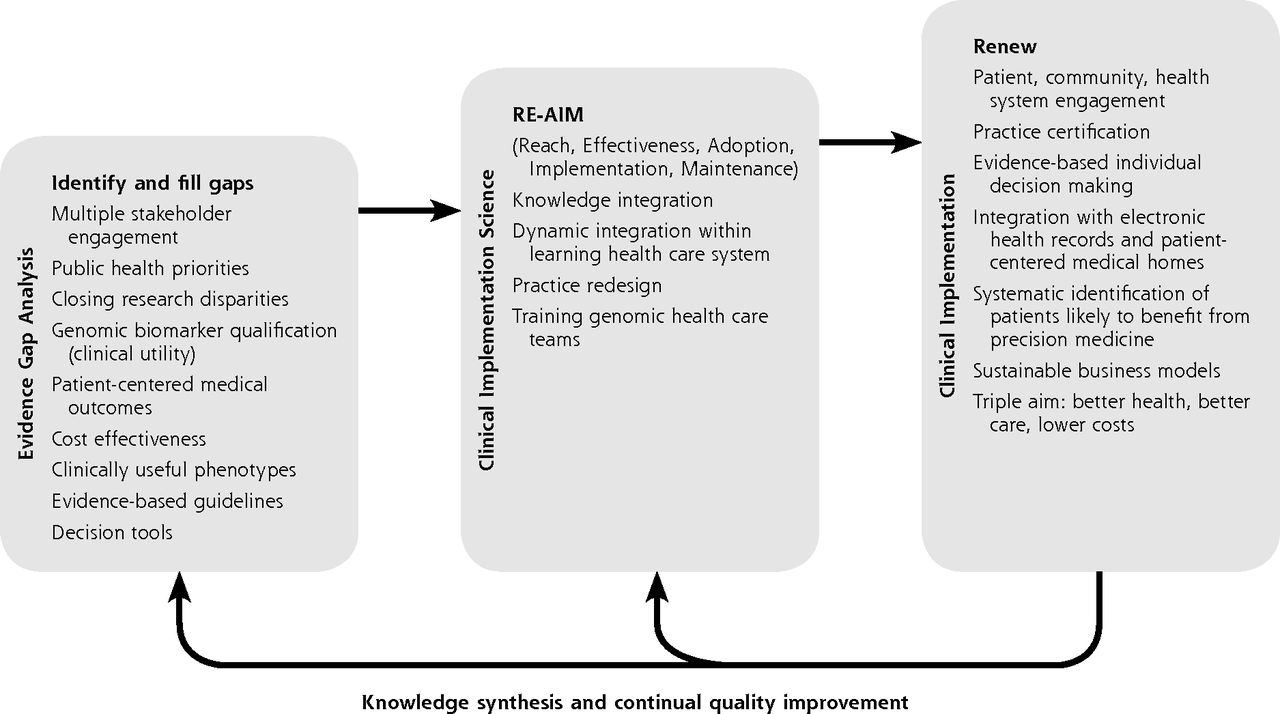
- Figure 1
Schematic roadmap for clinical implementation of genomic medicine in primary care.
Note: This roadmap depicts a planned process that begins and returns to gap analyses of the genomic medicine evidence base driven by clinical and public health priorities and the needs and values of health care professionals, patients, and multiple stakeholders. Generation of high-priority evidence with clinical utility is a prerequisite for clinical implementation (box 1). The systematic planning and evaluation of diffusion of genomic innovations can be accomplished using methods of clinical implementation science (box 2). Anticipating full clinical implementation enables planning and the development of systems to support continual quality improvement (box 3) and drive new knowledge acquisition to fill emerging evidence gaps and diffuse future innovations (return arrows).

Tables
Institute of Medicine Definition “Primary care is the provision of integrated, accessible health care services by clinicians who are accountable for addressing a large majority of personal health care needs, developing a sustained partnership with patients, and practicing in the context of family and community.” 4 Key features of primary care6,7 It is person rather than disease focused. This focus entails sustained relationships between patients and providers in primary care practices over time, often referred to as continuity.
It provides a point of first contact for whatever people might consider a health or health care problem. In properly organized health care systems, primary care ensures access to needed services.
It is comprehensive. By definition, it can encompass any problem. Many problems in primary care are ambiguous and defy precise diagnosis. Nonetheless, primary care meets a great majority of patient needs without referral.
It coordinates care. Primary care adopts mechanisms that facilitate the transfer of information about health needs and health care over time. Highly personalized solutions to patients’ problems can be implemented when sustained relationships permit deeper knowledge and understanding of individuals’ habits, preferences, and goals.
- Table 2
Challenges in Implementation of Genomic Medicine in Primary Care and Potential Solutions
Challenge Potential Solutions Limited evidence and conflicting interpretation of benefit/value Generate evidence of clinical utility of genomic medicine interventions in PCMH settings
Tailor needs for evidence against potential benefits and harms
Convene expert panels to develop primary care guidelines based on best evidence
Engage community-based practices to assist in developing evidence
Determine process outcomes of incorporating genomic information into EHRs
Publicize success widely
Organize consortia to conduct practice-based research trials of genotype-derived therapy when appropriateLack of institutional and clinician acceptance Carry out RE-AIM framework evaluation at the level of the PCMH or PCMH network (Figure 1)
Establish institutional advisory committee(s) involving senior leadership and partner with early adopter programs to evaluate evidence, recommend and monitor implementation—at health care centers, community or regional levels—consistent with principles of primary care (Table 1) and community values
Engage early adopters and clinical champions in demonstration efforts
Conduct pilot projects in early adopter PCMHs to develop results sufficient for follow-on funding
Obtain transinstitutional commitment at highest levels involving all relevant departments and stakeholders
Utilize internal pilot funding to catalyze initiation
Build clinician acceptance of clinical genetics professionals by judiciously integrating genetic counselors and/or geneticists in nongenetics clinical services throughout primary institution/clinic and affiliated institutions
Bring fragmented expertise for advancing genomic medicine under 1 transdisciplinary PCMH program or network
Harness institutional (clinic or affiliated health care center) quality improvement processes to assess valueLimited access to genomic medicine expertise and testing Use research-screening assays on site and confirm clinically actionable findings with rapid, cost-effective, CLIA-certified off-site testing if necessary
Establish or expand institutional CLIA-compliant genotyping to expand point-of-care testing, same-day service
Choose platform to assay multiple important genotypes simultaneously, reliably, and inexpensively
Invest in new equipment and personnel to ensure research quality is at the same level as the clinical laboratory; this effort requires institutional investment
Work with genetic counselors in PCMH teams to establish protocols for process and parameters of data returnLack of standards for genomic applications Develop agreed-upon framework or standards for evaluation of genomic medicine applications
Develop standardized order sets and process modification
Develop standards for analytic validity of whole-genome and whole-exome sequencing sufficient for clinical interpretation of the variants found by these methodsEHR integration of genomic results and CDS Enable access to actionable genomic information in the EHR through development of user-friendly decision-support algorithms for primary care clinicians
Establish a “usability lab” to test genomic medicine applications in the EHR and assess CDS tools
Allocate genomic medicine institutional funding to develop education and outreach to disseminate best practices incorporating family history and genomic information
Redesign EHR to include section dedicated to containing all relevant genotype results for each patient
Develop and link actionable drug-gene pair decision to electronic pharmaceutical ordering software at point-of-care adoption of pharmacogenomic testing
Establish interdisciplinary workgroup with genomic medicine, chronic care, and EHR team to create secure tools for EHR-based genomic decision support
Establish ordering protocols to prompt appropriate referrals to genetic counselors based upon type and indication of genomic testing orderedFollow-up of patients after genotyping Shift from relying on primary care clinician direct contact to PCMH/genomic medicine teams with permission of clinician
Analyze and address reasons for refusal to complete confirmatory testing, such as lack of coverage for testingOutreach to at-risk family members Clarify implications for family members and clinicians’ responsibilities toward family members
Explore ways to improve information to at-risk familiesConsent Ensure that informed consents for implementation projects conducted as research studies include returning results to patients and entering results into EHR
Conformance with standard of care and specific consent may not be needed
Consider implementation projects that might not require consent, such as results in established clinical pathways (tumor mutations and germline polymorphisms affecting treatment decisions) in partnership with medical subspecialists who have content-specific expertise
Develop standards for informed consent for extensive genotyping or sequencing, including whole-genome sequencing, and obtain it prospectively and combine with protocols for testing indications
Ensure that availability of personnel to manage consent/counseling is not rate limiting in initial implementationUnderstanding by patients, clinicians, public Conduct focus groups of patients, clinicians, and ancillary personnel to identify specific educational needs
Conduct genetic and genomic medicine campaign for patients, clinicians, and ancillary personnel based on focus group input
Survey retention of educational information by patients and clinicians and modify programs as needed
Conduct genotyping and/or sequencing and interpretation exercises with medical and other health profession students
Provide specific health care clinician education on when to order tests, and how to interpret results, and how to act on implications for family members and clinician’s responsibilities
Introduce pharmacogenomic lectures into health professionals’ training and continuing education
Provide clinical supervision to clinician trainees in use of pharmacogenomic testing, other genomic point-of-care testing
Include American Board of Family Medicine (and other boards) maintenance of certification self-assessment modules in genomic medicine
Development and dissemination of new educational objectives by the National Human Genome Research Institute Inter-Society Coordinating Committee for Practitioner Education in GenomicsLack of access to comparison “control” sequence data and banking resources Combine current PCMH’s small patient collections of reference sequences and make available to all centers
Prioritize funding for costly and time-consuming storage of viable tissues/biospecimens for DNA analyses
Biobank tissues/biospecimens for confirmatory clinical sequencing with patient identifiers
High-level institutional or PCMH network commitment to combine and organize multiple biorepositories for efficiency and ease of access while protecting patient privacyLack of research funding and reimbursement Until evidence is established for making genomic testing a new standard of care, consider research funding for testing in interim between discovery and adoption into PCMHs
Gradually change culture to convince health care community and patients of value of genomic medicine and need for reimbursement
Demonstrate cost of testing is not prohibitive and savings impact can be substantial
Provide institutional back-up for reimbursement to avoid charges to patients
Anticipate rises in interpretive and delivery costs as technology cost drops and enthusiasm increasesCDS = clinical decision support; CLIA = Clinical Laboratory Improvement Amendments; EHR = electronic health record; PCMH = patient-centered medical home; RE-AIM = reach, effectiveness, adoption, implementation, and maintenance.
Note: Challenges to clinical implementation identified by a National Human Genome Research Institute Genomic Medicine Colloquium representing 20 health care organizations and working groups in June 2011.16 Table adapted to the goal of integration of genomic medicine clinical implementation with primary care redesign.
The Article in Brief
Making Personalized Health Care Even More Personalized: Insights From Activities of the IOM Genomics Roundtable
Sean P. David , and colleagues
Background Genomic medicine may provide the greatest impact when systematically integrated with primary care, where most health care occurs, and where its delivery can be truly personalized. This report synthesizes insights from the Institute of Medicine Roundtable on Genomic-Based Research for Health and proposes a model for implementing genomic medicine into the patient-centered medical home (PCMH).
What This Study Found Implementation of clinical genomics into primary care and clinical practice has been limited because of critical evidence gaps, especially those related to clinical utility and applicability to diverse populations. A roadmap for integration could include three components: 1) evidence analysis and gap filling, 2) clinical implementation science, and 3) clinical implementation within a continuous improvement loop whereby clinical observations inform translational science and dissemination.
Implications
- To make personalized healthcare even more personal requires re-aiming translational pipelines towards more healing relationships in a continuously improving PCMH, which could enable realization of the primary care genomics partnership models envisaged by leaders in both fields.




{kind=link}