
Article Figures & Data
Figures
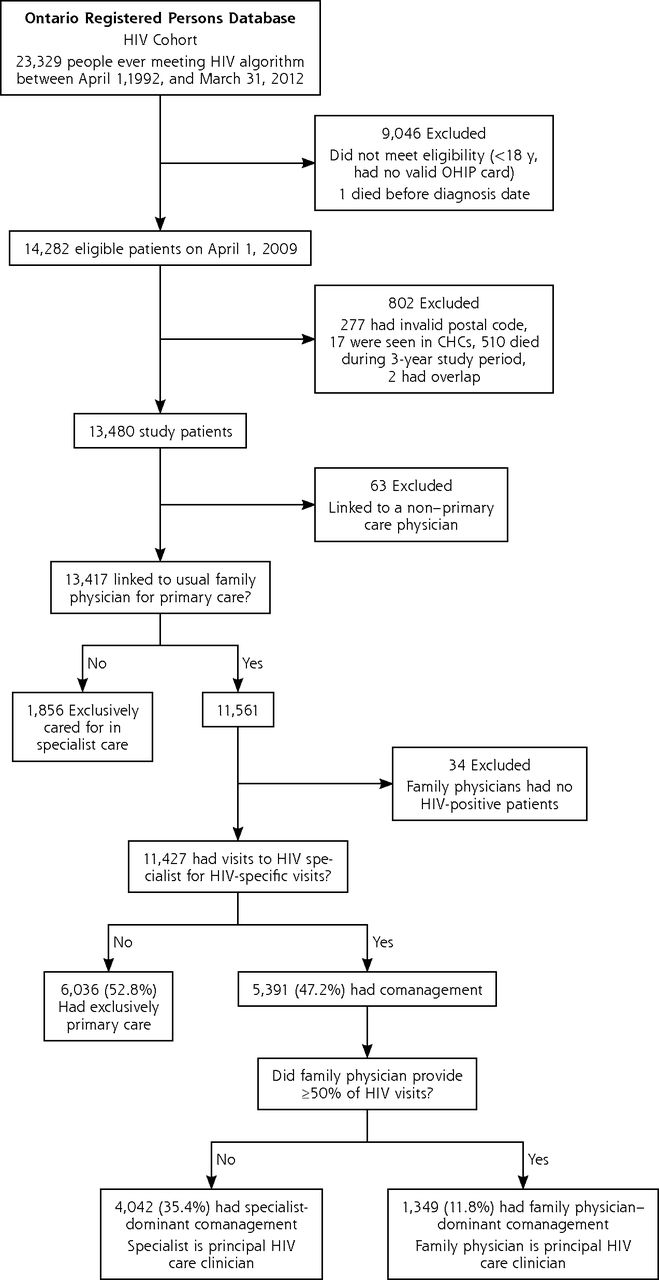
- Figure 1
Flow diagram of study participants.
CHC = community health center; HIV = human immunodeficiency virus; OHIP = Ontario Health Insurance Plan.
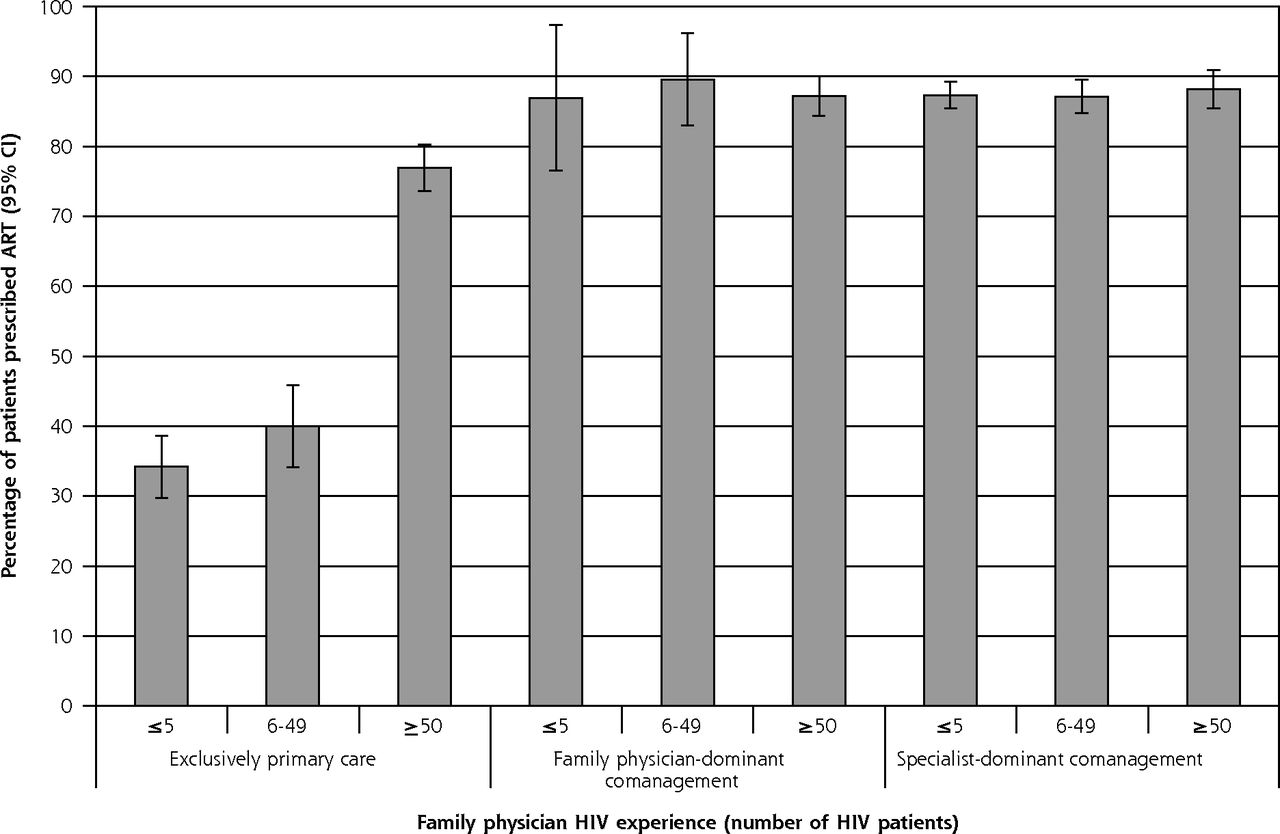
- Figure 2
Adjusted prevalence of receipt of ART among eligible patients by typology and family physician HIV experience.
ART = antiretroviral therapy; HIV = human immunodeficiency virus.
Notes: Percentage of patients with at least 1 ART prescription during study period, adjusted for all patient covariates and accounting for clustering by family physician. Error bars represent 95% CIs.


Tables
- Table 1
Characteristics of Patients Seen by Family Physicians Having Different Levels of HIV Experience
Characteristic ≤5 HIV Patients (n = 3,098) 6–49 HIV Patients (n = 1,987) ≥50 HIV Patients (n = 6,342) Total (N = 11,427) Patient characteristics Male sex, No. (%) 2,066 (66.7) 1,388 (69.9) 5,786 (91.2) 9,240 (80.9) Age, mean (SD), y 45.8 (12.0) 44.7 (10.6) 45.0 (9.6) 45.2 (10.5) Neighborhood income quintile, No. (%) Quintile 1 (lowest) 938 (30.3) 787 (39.6) 1,827 (28.8) 3,552 (31.1) Quintile 2 680 (21.9) 443 (22.3) 1,222 (19.3) 2,345 (20.5) Quintile 3 508 (16.4) 290 (14.6) 1,061 (16.7) 1,859 (16.3) Quintile 4 484 (15.6) 251 (12.6) 981 (15.5) 1,716 (15.0) Quintile 5 (highest) 475 (15.3) 204 (10.3) 1,174 (18.5) 1,853 (16.2) Missing 13 (0.4) 12 (0.6) 77 (1.2) 102 (0.9) Rurality index, No. (%) Major urban 2,437 (78.7) 1,835 (92.4) 6,042 (95.3) 10,314 (90.3) Non–major urban 527 (17.0) 122 (6.1) 244 (3.8) 893 (7.8) Rural 114 (3.7) 24 (1.2) 50 (0.8) 188 (1.6) Missing 20 (0.6) 6 (0.3) 6 (0.1) 32 (0.3) Immigrant status, No. (%) Canadian born 2,493 (80.5) 1,371 (69.0) 5,325 (84.0) 9,189 (80.4) Immigrant from Africa or Caribbean 327 (10.6) 432 (21.7) 474 (7.5) 1,233 (10.8) Immigrant from Europe or western nations 55 (1.8) 28 (1.4) 143 (2.3) 226 (2.0) Immigrant from other nations 223 (7.2) 156 (7.9) 400 (6.3) 779 (6.8) Mental health condition, No. (%) 1,302 (42.0) 850 (42.8) 2,555 (40.3) 4,707 (41.2) Comorbidity: ADG group, No. (%) High 867 (28.0) 502 (25.3) 1,393 (22.0) 2,762 (24.2) Medium 1,142 (36.9) 687 (34.6) 2,159 (34.0) 3,988 (34.9) Low 1,089 (35.2) 798 (40.2) 2,790 (44.0) 4,677 (40.9) Outpatient visits, mean (SD), No. 14.9 (15.2) 16.2 (21.6) 17.3 (13.8) 16.4 (15.8) Quality indicators, No. (%) Any ART prescription (n = 7,465) 1,402 (70.8) 1,037 (75.3) 3,324 (80.9) 5,763 (77.2) Colorectal cancer screening (n = 2,296) 260 (35.9) 140 (30.7) 505 (45.3) 905 (39.4) Cervical cancer screening (n = 1,946) 446 (50.7) 225 (41.1) 268 (51.5) 939 (48.3) Breast cancer screening (n = 513) 148 (54.8) 73 (57.0) 54 (47.0) 275 (53.6) Any emergency department visit 1,117 (36.1) 685 (34.5) 1,910 (30.1) 3,712 (32.5) Any hospital admission 372 (12.0) 212 (10.7) 579 (9.1) 1,163 (10.2) ADG = aggregated diagnosis group; ART = antiretroviral therapy; HIV = human immunodeficiency virus.
Note: Cell sizes containing 5 or fewer patients are not reported.
- Table 2
Hierarchical Logistic Regression Analysis of Receipt of ART, Cancer Screening, and Health Care Use
Variable Receipt of ART AOR (95% CI)a Colorectal Cancer Screening AOR (95% CI)a Cervical Cancer Screening AOR (95% CI)a Breast Cancer Screening AOR (95% CI)a Any ED Visit AOR (95% CI)a Any Hospital Admission Model of care delivery FP-dominant comanagement 2.04 (1.63–2.25) 1.25 (0.88–1.76) 0.77 (0.47–1.27) 3.90 (1.16–13.09) 1.11 (0.96–1.29) 2.16 (1.75–2.67) Specialist-dominant comanagement 2.23 (1.71–2.91) 0.88 (0.59–1.31) 0.72 (0.44–1.18 0.49 (0.13–1.79) 1.11 (0.94–1.31) 1.57 (1.22–2.02) Exclusively primary care (ref) 1.00b 1.00b 1.00 1.00 1.00 1.00b Family physician HIV experienceb ≤5 HIV patients 0.16 (0.12–0.21) 0.85 (0.56–1.29) 1.09 (0.70–1.69) 2.10 (0.84–5.27) 1.16 (0.98–1.37) 1.17 (0.89–1.53) 6–49 HIV patients 0.20 (0.15–0.27) 0.67 (0.42–1.08) 0.59 (0.35–0.99) 1.69 (0.58–4.91) 1.12 (0.92–1.37) 1.40 (1.02–1.91) ≥50 HIV patients (ref) 1.00 1.00 1.00 1.00 1.00 1.00 Interaction modelc FP HIV experience FP-dominant comanagementc ≤5 HIV patients 6.27 (2.40–16.34)b 0.98 (0.26–3.63) 1.45 (0.34–6.15) 0.08 (0.01–1.05) 0.65 (0.33–1.29) 1.24 (0.58–2.66) FP-dominant comanagementc 6–49 HIV patients 6.33 (2.92–13.71)b 1.17 (0.44–3.07) 0.67 (0.18–2.51) 0.09 (0.01–1.08) 0.85 (0.53–1.36) 0.70 (0.38–1.30) SP-dominant comanagementc ≤5 HIV patients 5.92 (4.10–8.57)b 0.76 (0.44–1.30) 0.96 (0.54–1.71) 0.87 (0.21–3.67) 0.90 (0.72–1.14) 0.87 (0.61–1.24) SP dominant comanagementc 6–49 HIV patients 4.54 (3.01–6.86)b 0.73 (0.39–1.38) 1.30 (0.67–2.53) 2.06 (0.41–10.36) 1.01 (0.77–1.32) 0.65 (0.43–0.98) Age, years 1.01 (1.00–1.01) 1.02 (1.00–1.04)b 0.98 (0.97–0.99)b 1.07 (1.01–1.12)b 0.99 (0.98–0.99)b 1.02 (1.02–1.03)b Sex, female 0.88 (0.74–1.04) 1.05 (0.79–1.39) – – 1.07 (0.95–1.20) 0.97 (0.82–1.16) Neighborhood income quintile Quintile 1 (lowest) 1.42 (1.12–1.73) 0.95 (0.71–1.27) 0.95 (0.66–1.36) 0.45 (0.20–1.00) 1.15 (1.01–1.30) 1.12 (0.92–1.36) Quintile 2 1.05 (0.85–1.28) 0.88 (0.64–1.21) 0.98 (0.66–1.44) 0.32 (0.14–0.76) 1.00 (0.87–1.15) 1.02 (0.83–1.27) Quintile 3 0.96 (0.81–1.25) 1.15 (0.83–1.59) 1.18 (0.78–1.77) 0.79 (0.33–1.90) 0.95 (0.82–1.10) 0.96 (0.77–1.20) Quintile 4 1.09 (0.88–1.34) 0.86 (0.62–1.21) 1.09 (0.71–1.66) 0.68 (0.27–1.76) 0.90 (0.77–1.04) 0.88 (0.69–1.11) Quintile 5 (highest) (ref) 1.00b 1.00 1.00 1.00d 1.00b 1.00 Rurality indexd Non–major urban 1.35 (1.04–1.69) 0.95 (0.68–1.32) 0.91 (0.61–1.35) 0.54 (0.25–1.15) 1.49 (1.28–1.73) 1.41 (1.13–1.75) Rural 1.18 (0.75–1.88) 0.66 (0.34–1.30) 0.70 (0.31–1.58) 0.38 (0.10–1.54) 1.79 (1.31–2.44) 1.82 (1.22–2.70) Urban (ref) 1.00 1.00 1.00 1.00 1.00b 1.00b Immigrant statusb Immigrant from Africa or Caribbean 1.58 (1.24–1.99) 0.90 (0.60–1.34) 1.04 (0.81–1.33) 1.66 (0.90–3.09) 0.77 (0.67–0.90)b 0.80 (0.63–1.02)b Immigrant from Europe or western nations 0.78 (0.50–1.24) 1.69 (0.78–3.64) 0.57 (0.23–1.38) 0.40 (0.06–2.82) 0.61 (0.44–0.85) 0.67 (0.38–1.20) Immigrant from other country 1.29 (1.00–1.68) 0.97 (0.60–1.57) 0.69 (0.46–1.03) 0.68 (0.28–1.69) 0.71 (0.59–0.84) 0.66 (0.49–0.90) Canadian born (ref) 1.00b 1.00 1.00 1.00 1.00 1.00 Mental health diagnosis 0.81 (0.71–0.93)b 0.71 (0.58–0.87)b 0.93 (0.75–1.15) 1.23 (0.77–1.99) 1.37 (1.26–1.50)b 1.28 (1.12–1.46)b Comorbidity: ADG category High 0.69 (0.59–0.82) 1.55 (1.19–2.03) 1.33 (1.01–1.73) 1.84 (0.97–2.48) 3.31 (2.95–3.71)b 3.45 (2.90–4.11) Medium 0.88 (0.75–1.02) 1.54 (1.23–1.92) 1.62 (1.27–2.08) 2.31 (1.27–4.21) 1.59 (1.43–1.76) 1.60 (1.35–1.91) Low (ref) 1.00b 1.00b 1.00b 1.00b 1.00 1.00b ADG = aggregated diagnosis group; AOR = adjusted odds ratio; ART = antiretroviral therapy; ED = emergency department; FP = family physician; ref = reference group.
↵a Adjusted for all listed patient covariates and interaction term of model of care delivery.
↵b Statistically significant (P for overall test of effect <.05).
↵c Family physician experience.
↵d P = .06.
Note: Analyses account for family physician cluster.
- Table 3
Mean Quality Indicators for Each Model of Care Delivery and Family Physician Level of HIV Experience
Model of Care Delivery and Family Physician HIV Experience Colorectal Cancer Screening % (95% CI) Cervical Cancer Screening % (95% CI) Breast Cancer Screening % (95% CI) Any ED Visit % (95% CI) Any Hospital Admission % (95% CI) Exclusively primary care ≤5 HIV patients 39 (32–47) 56 (50–62) 66 (56–77) 33 (30–35) 7 (6–9) 6–49 HIV patients 34 (25–43) 41 (32–50) 61 (44–79) 32 (28–36) 9 (7–11) ≥50 HIV patients 43 (36–50) 54 (45–63) 49 (22–68) 29 (27–32) 6 (5–7) Family physician–dominant comanagement ≤5 HIV patients 44 (14–75) 59 (27–91) 37 (0–90) 26 (13–39) 18 (7–28) 6–49 HIV patients 43 (22–63) 26 (4–49) 35 (0–81) 31 (22–39) 13 (7–19) ≥50 HIV patients 49 (40–58) 48 (36–59) 79 (60–97) 32 (28–35) 13 (11–15) Specialist-dominant comanagement ≤5 HIV patients 30 (25–35) 47 (42–52) 46 (35–56) 33 (30–35) 10 (9–11) 6–49 HIV patients 25 (19–31) 39 (33–46) 61 (47–76) 34 (31–37) 9 (7–11) ≥50 HIV patients 40 (31–49) 49 (35–57) 31 (7–56) 32 (28–35) 10 (8–12) HIV = human immunodeficiency virus; ED = emergency department.
Note: Analyses are adjusted for patient age, sex, income quintile, rurality, immigrant status, aggregated diagnosis group category, presence of a mental health condition, and experience category of the family physician, and account for clustering by family physician.
The Article in Brief
A Population-Based Study Evaluating Family Physicians' HIV Experience and Care of People Living With HIV in Ontario
Claire Kendall , and colleagues
Background Antiretroviral therapy (ART) for HIV infection has reduced death and disease and shifted the care needs of people living with long-term HIV. Early studies found that clinicians with more training and/or experience in HIV provided higher quality of care, but as the disease and treatments become less novel and complex, quality of HIV care between generalist and specialist physicians has become more similar. This 4-year study explores whether the HIV experience of family physicians effects the association between model of care delivery and the quality of care for people living with HIV.
What This Study Found Family doctors who take care of more HIV-positive patients in their regular practice are more likely to follow antiretroviral therapy protocols than other family doctors. Among more than 13,000 HIV-positive patients, the majority saw family physicians exclusively for their care. Those who saw a family physician with the highest level of HIV experience were almost twice as likely to receive ART than those seeing less experienced family physicians. Cancer screening and health service use were not influenced by family physician HIV experience. The influence of family physician HIV experience appears to be mitigated by having an HIV specialist in the model of care.
Implications
- The authors conclude that to ensure adequate ART prescribing, care delivery models for people with HIV should include either an HIV specialist or a family physician with considerable HIV experience.




{kind=link}
{kind=link}