
Abstract
PURPOSE We aimed to determine the impact of transitional care interventions (TCIs) on acute health service use by patients with congestive heart failure in primary care and to identify the most effective TCIs and their optimal duration.
METHODS We conducted a systematic review and meta-analysis of randomized controlled trials, searching the Medline, PsycInfo, EMBASE, and Cochrane Library databases. We performed a meta-analysis to assess the impact of TCI on all-cause hospital readmissions and emergency department (ED) visits. We developed a taxonomy of TCIs based on intensity and assessed the methodologic quality of the trials. We calculated the relative risk (RR) and a 95% confidence interval for each outcome. We conducted a stratified analysis to identify the most effective TCIs and their optimal duration.
RESULTS We identified 41 randomized controlled trials. TCIs significantly reduced risks of readmission and ED visits by 8% and 29%, respectively (relative risk = 0.92; 95% CI, 0.87–0.98; P = .006 and relative risk = 0.71; 95% CI, 0.51–0.98; P = .04). High-intensity TCIs (combining home visits with telephone followup, clinic visits, or both) reduced readmission risk regardless of the duration of follow-up. Moderate-intensity TCIs were efficacious if implemented for a longer duration (at least 6 months). In contrast, low-intensity TCIs, entailing only followup in outpatient clinics or telephone follow-up, were not efficacious.
CONCLUSIONS Clinicians and managers who implement TCIs in primary care can incorporate these results with their own health care context to determine the optimal balance between intensity and duration of TCIs. High-intensity interventions seem to be the best option. Moderate-intensity interventions implemented for 6 months or longer may be another option.
INTRODUCTION
Congestive heart failure (CHF) imposes an increasingly heavy burden on health care systems, most of which can be attributed to numerous hospital readmissions and emergency department (ED) visits.1–3 Multiple exacerbations of CHF result in frequent use of acute health care services by these patients, known as revolving door users. After discharge, 25% of patients are readmitted within the first 30 days,4,5 and 50% within the first 6 months.6,7
This frequent use of health care services is mainly due to lack of understanding of a treatment plan, nonadherence to medical therapy, unawareness of CHF symptom exacerbation, and irregular follow-up.8–12 Lack of coordination and communication between hospitalists and primary care physicians (PCPs) has been documented.13,14 PCPs too often do not receive discharge summaries,15 and when they do receive them, the summaries often lack appropriate documentation of medication indication and advice for follow-up. It is therefore difficult for PCPs to plan an appropriate follow-up after hospital discharge.16
To address these issues, transitional care interventions (TCIs) have been implemented with a common objective of reducing the rate of hospital readmission and ED visits.2,17–19 Coordination of appropriate transition plans is now one of the suggested domains that should be measured when assessing patient-centered medical homes.20 TCIs comprise a broad range of time-limited health services including patient or caregiver education on self-management, discharge planning, structured follow-up, and coordination among health care professionals involved in the transition, including PCPs.2,17,18,21
To date, a few systematic reviews have been published on TCIs.22–24 It has been shown that the interventions decrease hospital admissions after 12 months of follow-up.22 These reviews, however, were unable to determine the most efficacious TCI.22,24 They did not include all types of TCIs22,23; furthermore, a substantial number of RCTs on these interventions have been published since the publication of the reviews (26 since that by Phillips et al24). We therefore conducted a systematic review and meta-analysis to determine the impact of TCIs on the rate of all-cause readmission and ED visits by patients with CHF, and to identify the most effective TCIs and their optimal duration.
METHODS
A systematic review and meta-analysis, conducted according to Cochrane recommendations, allowed us to integrate and summarize the results of a large number of studies.25 The protocol was approved and funded by the Canadian Institutes of Health Research (KRS-250478). We used the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) framework26 for reporting the results.
Eligibility Criteria
Trials were eligible for inclusion if they had a randomized controlled design and enrolled patients with CHF discharged from inpatient departments to home. The trials had to compare some form of TCI with usual care, and had to collect data on all-cause readmission and all-cause ED visits (Supplemental Appendix 1, available at http://www.annfammed.org/content/13/6/562/suppl/DC1.)
Information Sources and Search
A librarian specializing in systematic reviews conducted the literature search. We performed a systematic search of 4 databases (MEDLINE, PsycINFO, EMBASE, and Cochrane Database of Systematic Reviews) for articles published between 1995 (beginning of TCI) and February 6, 2014. The key words were “heart failure,” “transition,” “care planning,” and “discharge” (Supplemental Appendix 2, available at http://www.annfammed.org/content/13/6/562/suppl/DC1). We also screened reference lists of included articles to look for potential additional interventions. All companion articles of the included studies were searched.
Study Selection
We used a 2-step approach to study selection. First, 2 reviewers (I.V., V.K.) independently examined the references (titles and abstracts) based on the eligibility criteria. Second, full texts of the selected references were retrieved, read, and selected based on the eligibility criteria. At each step, differences in coding were resolved by consensus.
Data Collection Process and Items
Information was extracted from each study by 2 researchers (Melanie Le Berre, PT, MSc, and Martin Beauchamp, Aux Nurse) independently and included author, publication date, country, components of the intervention, health care professionals involved, frequency and duration of follow-up, study design, duration of the study, and participant characteristics such as sample size, mean age, percentage of males, and severity of CHF. Outcomes were extracted at the final follow-up and at various follow-up periods. Any discrepancies were resolved through consensus.
Risk of Bias in Individual Studies
The quality of the studies was assessed independently by 2 reviewers (V.K. and Quan Nha Hong, PhD[C]) using a validated tool for the critical appraisal of experimental studies, the Downs and Black scale,27 which had demonstrated a high validity (r = .90) and interrater reliability (r = .75).28 Particular attention was paid to randomization generation, allocation concealment, the blinding of participants and/or outcome assessors, and loss to follow-up. We categorized quality as higher (≥20 = very good, 15 to 19 = good) or lower (11 to 14 = fair, ≤10 = poor).29 Interrater reliability was calculated using the interrater correlation coefficient.30 Any disagreement was resolved by consensus.
Summary Measures
As recommended in the review of complex interventions,31 and in line with our protocol, 3 experts in the areas of integrated care, care management, and systematic reviews (I.V., V.K., and Ian Shrier, MD, PhD) developed a taxonomy by consensus to classify TCI into homogeneous groups of interventions. To develop the taxonomy, we first looked at the included interventions and described them in detail, before examining the results of the studies. Second, we examined the extant literature, including other systematic reviews, to identify key components of interventions and their link with intensity. On the basis of this literature review, the 2 key elements were home visits, usually by a home nurse, and frequency of monitoring. Indeed, direct contact and, in particular, home visits,32,33 led to a reduction of readmissions, whereas phone calls did not.33 Home visits reinforced self-management (better understanding of the disease and adherence to treatments).34 Home visits also eliminated transportation to the physicians’ offices and pharmacies, among the main contributors to readmission of older patients.34 Repeat visits also had an impact on long-term outcomes.35 The included interventions were then classified as low, moderate, or high in intensity (Table 1).
Classification System for Intensity of Transitional Care Interventions
Synthesis of Results
We conducted a meta-analysis using Review Manager 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration) to determine the differences between the TCI group and the usual care group in their risks of readmission and ED visits at the last provided follow-up time. Relative risks (RRs) and their 95% CIs were calculated to estimate the mean effect size. We also calculated the number needed to treat to estimate the clinical importance of a TCI. If more than 1 publication described the same study, it was treated as 1 study. If 1 publication studied multiple interventions, each intervention was included in the meta-analysis. We used random-effects models, as we expected the different interventions to vary in their effects. Meta-analyses were performed on an intention-to-treat basis when possible. The I2 statistic was used to measure heterogeneity.36 We contacted authors for additional data to conduct the meta-analysis when it was required.
Risk of Bias Across Studies
To determine if there were any reporting biases in our included studies, we created a funnel plot, plotting the study standard errors vs the logarithm of the risk ratios, as per the Cochrane recommendations.25
Additional Analyses
We performed subgroup analyses to explore the effect on risk of readmission attributable to intensity of TCI, severity of CHF, and mean age of participants. To further investigate the most effective combination of intervention characteristics, we conducted a stratified analysis on the interaction between intervention intensity and duration. The stratification was conducted on a 6-level categorical variable: low intensity and 6 months or shorter; moderate intensity and 6 months or shorter; high intensity and 6 months or shorter; low intensity and longer than 6 months; moderate intensity and longer than 6 months; and high intensity and longer than 6 months.
To assess the robustness of our intervention effect estimates, we conducted sensitivity analyses, excluding possible outlier studies, cluster-randomized trials, TCIs with additional components, and RCTs with lower methodologic quality.
RESULTS
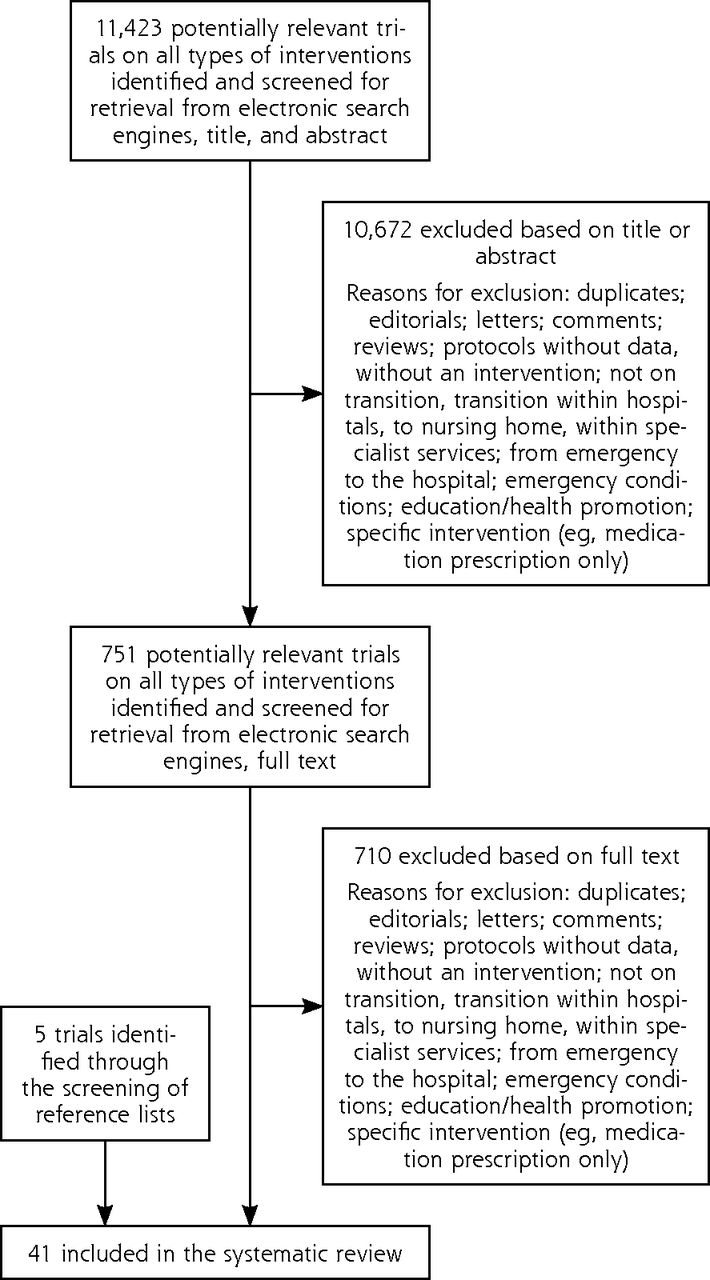
Out of 11,423 references, 41 RCTs and a total of 43 interventions were included in the review,8–10,35,37–73 including 5 trials identified through the screening of reference lists43,44,51,56,62 (Figure 1, Table 2, and Supplemental Appendix 3, available at http://www.annfammed.org/content/13/6/562/suppl/DC1; 3 companion articles were identified81–83).
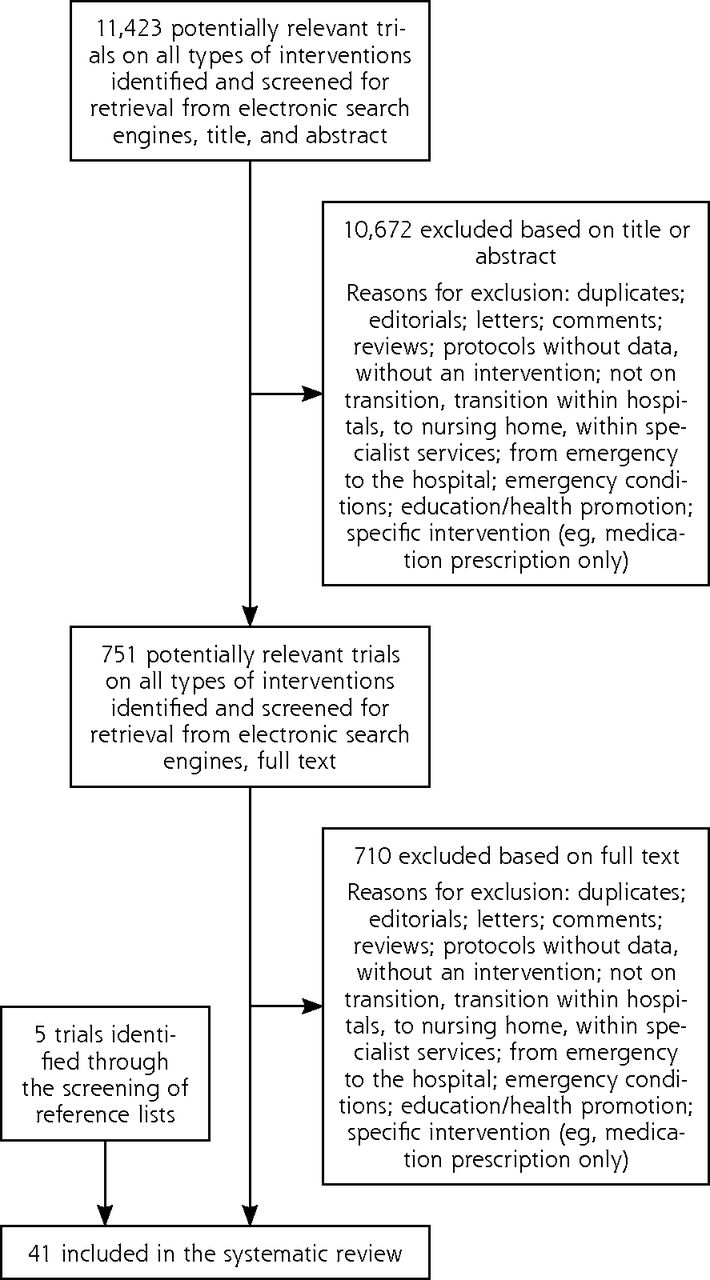
Trial selection flowchart.
Summary Characteristics of Included Trials
The length of follow-up ranged from 1 to 24 months postdischarge. The mean age of patients ranged from 57.9 to 81.0 years, and 65.6% of patients were men.
Usual care was sparsely described in the studies. It consisted of predischarge education on CHF self-management and usual follow-up with the family physician or cardiologist as required.
TCI Characteristics
TCIs included predischarge education for patients (on CHF management, nonpharmacologic strategies, and medication management, usually given by a specialized CHF nurse using written or video material), a discharge plan (including a medication review, individualized care plan development, and a discharge letter sent to the family physician or cardiologist), and structured, proactive, and prearranged follow-up. The trials were nearly evenly split by the intensity of their TCI: 13 studied low-intensity interventions; 14, moderate-intensity interventions; and 16, high-intensity interventions (Table 3). Some interventions had additional components: a nurse visiting the hospital in cases of readmission,35,72 and patients having access to a nurse either during office hours59,64 or at all times.45,63
Intensity of Included Transitional Care Interventions
Risk of Bias in Individual Trials
Overall, 35 trials were of higher quality (very good or good) (Supplemental Appendix 4, available at http://www.annfammed.org/content/13/6/562/suppl/DC1). Six were of fair quality.9,42,43,49,52,71 None of the trials were of poor quality. The interrater correlation coefficient was strong (0.79; 95% CI, 0.63–0.88; P <.0001).30
Blinding of participants was not possible because of the nature of the interventions. Sixteen RCTs described blinding of outcome assessors* and 5 reported some level of allocation concealment.8,10,55,62,66 Loss to follow-up was acceptable (less than 20%) in 35 RCTs.
Effect on All-Cause Hospital Readmission
Forty-three interventions provided data on all-cause readmission; a forest plot of their results is shown in Figure 2. The meta-analysis showed a significant reduction in the relative risk of readmission with a TCI as compared with usual care (RR = 0.92; 95% CI, 0.87–0.98), indicating that TCI reduces the risk of readmission by an average of 8%. The number needed to treat was 52, meaning that 52 patients had to receive the TCI for 1 patient to benefit (1 less readmission to occur).
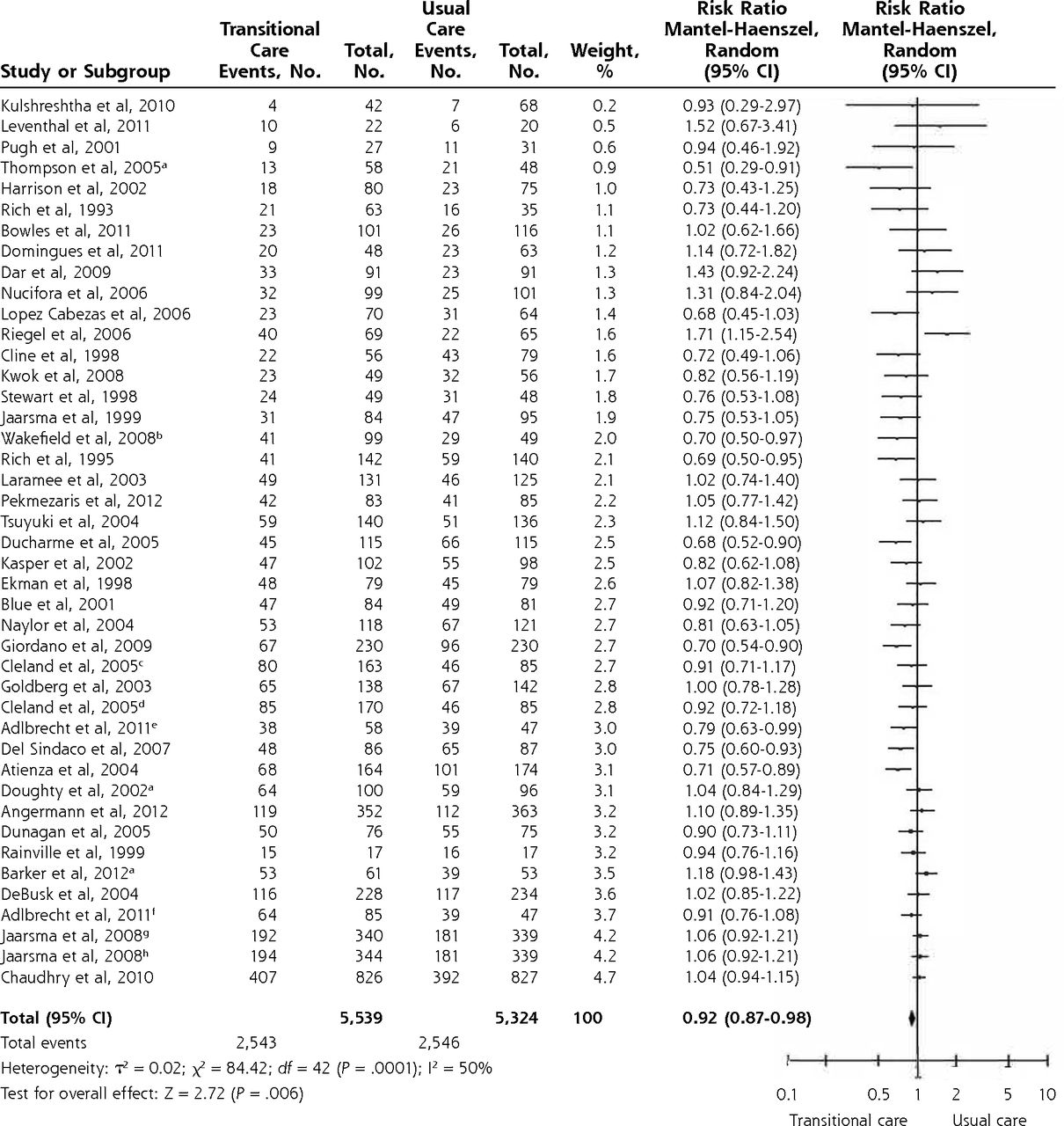
Forest plot for all-cause readmission (presented by weight).
Note: Percentage of patients with events: 45.9% in the incidence group and 47.8% in the control group.
aCluster randomization.
bTelephone and video telephone follow-up.
cTelecare.
dTelephone follow-up.
eIntervention guided by N-terminal pro-B-type natriuretic peptide.
fMultidisciplinary intervention.
gFollow-up in clinic.
hFollow-up in clinic and monthly contact with the nurse.
Effect on All-Cause ED Visits
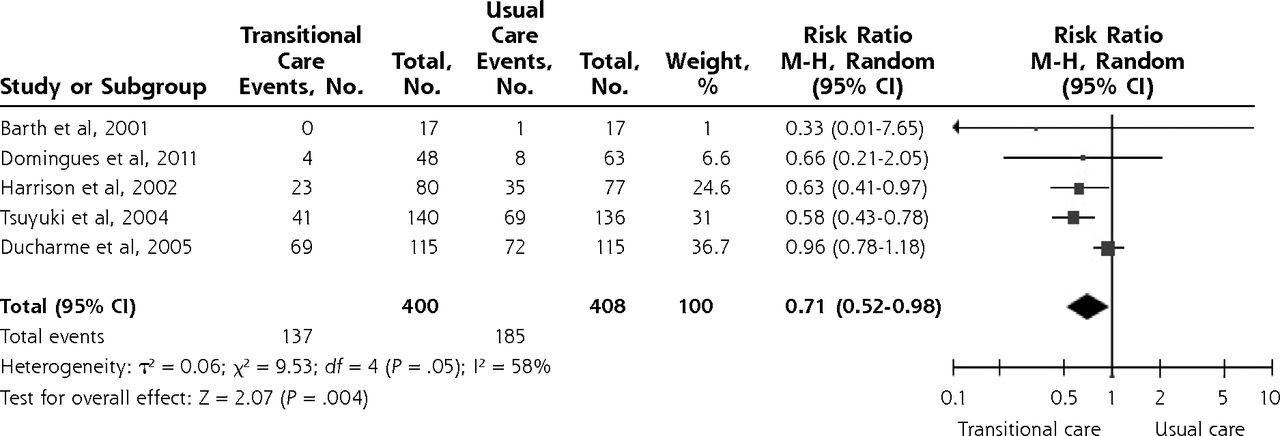
Five trials provided data on all-cause ED visits43,53–56; a forest plot of their results is shown in Figure 3. The meta-analysis showed a significant 29% reduction in the risk of ED visits for TCI as compared with usual care (RR = 0.71; 95% CI, 0.52–0.98). The number needed to treat was 9, meaning that 9 patients had to receive the TCI for 1 patient to benefit (1 less ED visit to occur).

Forest plot for all-cause emergency department visits (presented by weight).
Note: Percentage of patients with events: 34.3% in the intervention group and 45.4% in the control group.
M-H = Mantel-Haenszel
Additional Analyses
The results of the exploratory subgroup analyses suggested that high-intensity interventions are efficacious at reducing the risk of readmission (RR = 0.86; 95% CI, 0.78–0.94), and that they are most efficacious in a population with mean age of 75 years and older (RR = 0.83; 95% CI, 0.76–0.92) (Supplemental Appendix 5, available at http://www.annfammed.org/content/13/6/562/suppl/DC1). To further investigate the effects of intervention characteristics on readmission risks, and to find the most effective combination of characteristics, we conducted a stratified analysis on the interaction between intervention intensity and duration. Results showed that the different intensity and duration combinations do in fact have significantly different mean effects on the relative risk of readmission (P = .003) (Table 4). High-intensity interventions continued to be associated with a reduced risk of readmission regardless of their duration, and interventions of moderate intensity seemed to decrease the risk if they lasted longer than 6 months. Neither moderate-intensity, short-duration interventions, nor any of the low-intensity interventions significantly reduced the risk of readmission.
Summary of Intervention Intensity- and Duration-Stratified Analysis
Because of the small number of studies, we could not carry out further analyses on the risk of ED visits.
The results of the sensitivity analyses are presented in Supplemental Appendix 6 (available at http://www.annfammed.org/content/13/6/562/suppl/DC1). We did not detect any differences in the estimated mean effects when omitting outlier studies, cluster trials, trials with additional components, and those having lower methodologic quality. Lastly, according to the Fisher exact test, the quality of the study and the TCI intensity were independent of one another (P = .66). Overall, the main findings were robust in sensitivity analyses.
Risk of Bias Across Studies
There was no appearance of a systematic asymmetry in the funnel plot (plotting the study standard errors vs the logarithm of the risk ratios) (Supplemental Appendix 7, available at http://www.annfammed.org/content/13/6/562/suppl/DC1). We therefore have no reason to believe that any reporting biases exist in our trials.
DISCUSSION
Providing TCI to patients with CHF discharged to home showed mean 8% and 29% risk reductions of all-cause readmission and ED visits, respectively. TCI was far more efficacious in decreasing ED visits than in reducing hospital readmission: the number needed to treat was only 9 patients to avoid an ED visit vs 52 to avoid a readmission. These results are in line with previous reviews of studies of older CHF patients receiving comprehensive discharge planning plus postdischarge support.22,24 In contrast to previous meta-analyses,21,24,74 we further identified more efficacious interventions and optimal intervention durations. Our results suggest that high-intensity TCIs need be sustained for only a short duration (6 months or less) to be effective at reducing the risk of readmission, while moderate-intensity interventions need to be of a longer duration (more than 6 months) to have a similar effect. It is therefore essential to provide individualized TCI to patients, and to triage patients for high-intensity or moderate-intensity intervention; risk stratification may help in guiding triage.75
In contrast to a meta-analysis by Feltner et al,21 we found that follow-up in the outpatient clinic only, that is, the usual postdischarge arrangement, does not improve the outcomes studied. Similarly, telephone follow-up used in isolation—the most frequently reported type of TCI (11 RCTs)—was not efficacious. In all cases, low-intensity TCI should be avoided.
A key element of TCI is follow-up of patients by a PCP within a week after discharge. It is well known that early physician follow-up postdischarge and physician continuity are associated with better outcomes among patients with CHF.76 Advanced access scheduling for discharged patients is one means for enabling timely follow-up after discharge.77 Successful communication between hospitals, in particular cardiologists, and PCPs is also of paramount importance. Hospitals need to notify PCPs of patients discharged and send the summary for return visits. As the information on many discharge summaries is often inadequate for PCPs to manage continuity of care,16,78 however, the quality of these summaries needs to be improved, in particular the documentation of drug indications and follow-up.16
Several limitations of this review should be mentioned. Because of resource constraints, we were not able to include articles in languages other than English and French. An objective measure of intensity that takes into account TCI type (face to face vs remote) as well as the number of contacts would have been more appropriate, but not all the studies systematically reported the number of contacts. Patient characteristics, including diagnosis, comorbidities, and severity of CHF, were missing in some studies. Future studies on TCI should exhaustively describe interventions, including the number of contacts, the components of the intervention (eg, use of medications, self-management) as well as patient characteristics (eg, receipt of diagnostics). Our study is also limited by a lack of published studies on “oldest-old” patients (those aged 85 years and older), who frequently have multiple comorbidities and functional and cognitive impairments,79 and who represent the fastest growing segment of the population.80 The effect of the TCI might differ for this group, so future studies should consider this population. Furthermore, had more studies been available, we could have adjusted the meta-analyses for mean age of patients, as well as follow-up duration. The vast majority of included studies reported comorbidities; therefore, we could not conduct analyses exploring relationships between CHF, comorbidities, and TCIs. Future systematic reviews on TCI for patients with multiple comorbidities are needed.
In conclusion, providing TCI to CHF patients reduces readmission and ED visits. High-intensity interventions, regardless of intervention length, seem to be the best option. Moderate-intensity interventions implemented for long duration may be another option. Clinicians and managers who implement TCI in primary care can incorporate these findings with the health care context to determine the optimal balance between intensity and duration of interventions.
Acknowledgments
We would like to thank Ian Shrier, MD, PhD, for his advice on meta-analyses and development of taxonomy; Muriel Gueriton, specialized librarian, for the literature search; Pierre Pluye, MD, PhD, and Quan Nha Hong, PhD(C), for assistance with the methodologic quality assessment; Geva Maimon, PhD, biostatistician, for assistance with the stratified analysis; and research assistants Melanie Le Berre, PT, MSc, and Martin Beauchamp, Aux Nurse, for assistance with study selection.
Footnotes
Conflicts of interest: authors report none.
Funding support: This study was funded by the Canadian Institutes of Health Research (KRS-250478).
Previous presentation: Preliminary results of this study were presented as an oral presentation at the North American Primary Care Research Group Conference; November 21-25, 2014; New York, New York.
Supplementary materials: Available at http://www.AnnFamMed.org/content/13/6/562/suppl/DC1/.
- Received for publication January 25, 2015.
- Revision received June 30, 2015.
- Accepted for publication July 10, 2015.
- © 2015 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Primary care Adherence To Heart Failure guidelines IN Diagnosis, Evaluation and Routine management (PATHFINDER): a randomised controlled trial protocol
- The Impact of Telephonic Follow-Up Within 2 Business Days Postdischarge on 30-Day Readmissions for Patients With Heart Failure
- Impact of team-based community healthcare on preventable hospitalisation: a population-based cohort study in Taiwan
- Effects of Transitional Care on Hospital Readmission and Mortality Rate in Subjects With COPD: A Systematic Review and Meta-Analysis
- Patient Perceptions on Facilitating Follow-Up After Heart Failure Hospitalization
- In This Issue: Multilevel Effects