
Abstract
PURPOSE Positive effects have been reported after mindfulness-based interventions (MBIs) in diverse clinical and nonclinical populations. Primary care is a key health care setting for addressing common chronic conditions, and an effective MBI designed for this setting could benefit countless people worldwide. Meta-analyses of MBIs have become popular, but little is known about their efficacy in primary care. Our aim was to investigate the application and efficacy of MBIs that address primary care patients.
METHODS We performed a meta-analytic review of randomized controlled trials addressing the effect of MBIs in adult patients recruited from primary care settings. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and Cochrane guidelines were followed. Effect sizes were calculated with the Hedges g in random effects models.
RESULTS The meta-analyses were based on 6 trials having a total of 553 patients. The overall effect size of MBI compared with a control condition for improving general health was moderate (g = 0.48; P = .002), with moderate heterogeneity (I2 = 59; P <.05). We found no indication of publication bias in the overall estimates. MBIs were efficacious for improving mental health (g = 0.56; P = .007), with a high heterogeneity (I2 = 78; P <.01), and for improving quality of life (g = 0.29; P = .002), with a low heterogeneity (I2 = 0; P >.05).
CONCLUSIONS Although the number of randomized controlled trials applying MBIs in primary care is still limited, our results suggest that these interventions are promising for the mental health and quality of life of primary care patients. We discuss innovative approaches for implementing MBIs, such as complex intervention and stepped care.
- mindfulness-based interventions
- primary care
- meta-analysis
- randomized controlled trials
- complex interventions
- practice-base research
INTRODUCTION
There is growing recognition of the value of mindfulness-based interventions (MBIs) for clinicians and policy makers.1–7 One important challenge for psychosocial intervention is to confirm the efficacy found in randomized controlled trials (RCTs) in routine clinical practice, particularly in primary care,8–10 where accessibility and adherence to and implementation of MBIs in health systems may be enhanced.11–13 MBIs are considered complex interventions because their implementation takes into account behavior change in patients and health professionals, as well as their adaptation to setting and culture.14
Our objective was to perform, for the first time, a meta-analytic review of RCTs to investigate the application and efficacy of MBIs in primary care patients. We had several initial hypotheses14: (1) the number of well-designed studies in primary care is greater than that in other levels of care, because most patients receive long-term assistance here; (2) the clinical impact of MBIs in primary care patients is greater than that at other levels of the health system, because such patients adhere more to mindfulness programs; (3) the range of health conditions addressed by MBIs is larger in primary care (including health promotion in at-risk population and application in patients with multimorbidity),15 owing to unrestricted access to such care; and (4) as MBIs are complex interventions in primary care, their program contents are systematically adapted to patients’ local needs, services, culture, and epidemiology.
METHODS
We followed the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) for systematic reviews and meta-analyses16 and the recommendations of the Cochrane Collaboration.17 The protocol was registered with PROSPERO (International Prospective Register of Systematic Reviews), registration number CRD42013004133.
Eligibility Criteria
We included RCTs of MBIs for patients recruited in primary care that compared the intervention with a control condition. Only RCTs were included to reduce bias, as mindfulness interventions have been criticized for their nonspecific components, such as their group-supportive environment.18
We considered primary care services those that provide coordinated, accessible, comprehensive, and long-term health care services addressing a large majority of personal health care needs, and practices in the context of family and community.18 Only full-text articles in peer-reviewed scientific journals were included. No restrictions were applied regarding language, control group characteristics, follow-up, or type of data analysis.
The RCTs had to take place among adult patients aged 18 years or older from primary care. No restrictions were placed on existing diseases or conditions, sex, race, or profession.
We allowed any MBI that listed mindfulness as a key component, including mindfulness-based stress reduction (MBSR), mindfulness-based cognitive therapy (MBCT), or similar.2 We excluded any blended or mixed intervention having only a mindfulness component, such as acceptance and commitment therapy (ACT) and dialectical behavioral therapy (DBT) or similar. The control condition could have included usual treatment, placement on a waiting list, or any active control, such as other types of psychosocial interventions, pharmacotherapy, or placebo.
The outcomes measured for this analysis were clinical outcomes and patient-reported outcomes from any self-reported instrument used to measure mindfulness or any health-related variable (http://www.nihpromis.org/).
Search Strategy
We searched MEDLINE (via PubMed), Embase, PsycINFO, CINAHL (via EBSCO), LILACS, Scopus, and the Cochrane Central Register of Controlled Trials (CENTRAL). All searches were from database inception until September 4, 2014, where the medical subject heading (MH) term mindfulness was included. We combined controlled vocabulary and free-text terms; Table 1 shows the general search strategy, and Supplemental Appendix 1, available at http://www.annfammed.org/content/13/6/573/suppl/DC1, shows the specific search strategies for each database. Search results were imported into an electronic bibliography after the removal of duplicate citations. We also screened references in the included studies, performed citation tracking, and contacted other experts in the field for additional studies.
Search Strategy
Data Extraction and Coding
Two authors (M.M.P.D. and J.G-C.) screened citations for inclusion by examining the titles and abstracts. Disagreements were discussed with a third author (J.M-M.). Two reviewers (M.M.P.D. and J.G-C.) independently examined the full texts of the potentially relevant studies. Resolution for disagreement was reached through discussion with a third reviewer (J.M-M.). Each selected study was assessed independently by at least 2 authors (M.M.P.D., K.M., A.V., E.Z-O., Y.L-H., C.V., or J.G-C.), and the data were extracted using a predefined data extraction sheet. Any disagreement was referred to another author (J.M-M.) for resolution.
We coded the studies for year and country of publication; target patient and disorder or condition; age; percentage of women; MBI type and characteristics (number of sessions and length of intervention); level of administration (individual vs group); method of administration (human vs media); type of control condition; number of participants; setting for delivery; role of the health professional delivering the intervention; follow-up; completion rate; primary and secondary outcomes; and added contact after intervention.
Assessment of Study Quality
Risk of bias was assessed using the Cochrane Collaboration’s tool,19 considering those studies that met 3 or more criteria as high quality, and those that met fewer criteria as low quality.20 Quality of interventions was evaluated according to 3 criteria21: use of a treatment manual, provision of therapy by specifically trained therapists, and verification of treatment integrity during the study. Two reviewers (M.M.P.D. and J.M-M.) independently assessed these criteria, and any discrepancies were discussed with a third reviewer (J.G-C.) for consensus.
Data Synthesis
We calculated effect sizes, indicating the differences between the 2 groups and the 95% confidence intervals at posttest or follow-up.22,23 When necessary, combined outcomes were estimated using a pooled mean-effect size provided by the Comprehensive Meta-Analysis-2.0 program (Biostat Inc). We chose the Hedges g as the effect size measure because it adjusts accordingly for studies with a small sample size.24 It has been suggested that a g value of 0.0 to 0.40 can be considered small; 0.4–0.7, moderate; and greater than 0.7, large.17
Because considerable heterogeneity among studies was expected, the pooled effect size was calculated using the random effects model. We tested heterogeneity using the I2 statistic and 95% confidence intervals,25–28 assuming a value of 25% to indicate low heterogeneity; 50%, moderate; and 75%, high. We also calculated the Q statistic and the associated P value.
Subgroup analyses were conducted with the mixed effects model to evaluate possible differences according to the outcome (mental health or quality of life), type of intervention (MBSR or MBCT), time point of measurement (posttest, follow-up <6 months, follow-up >6 months), type of control condition (active or passive), type of clinical condition or disease (mental or somatic), use of intention-to-treat analysis (yes or no), study quality (high or low), and origin (Europe or rest of the world) as probable sources of heterogeneity. This model pools studies within the subgroups of the random-effects model and tests for significant differences between subgroups with the fixed-effects model.29 When subgroups had fewer than 3 trials, we did not analyze heterogeneity and risk of bias.
Publication Bias
We assessed publication bias through funnel plots.30–32 The test of Egger et al33 was used to contrast the null hypothesis with biased absences, and the trim and fill procedure of Duval and Tweedie32 provided the number of studies probably absent, allowing an estimate of the effect sizes taking publication bias into account. We also applied the rank correlation of Begg and Mazumdar34 to test whether the adjusted and observed effect sizes differed significantly.
All of the tests were 2 tailed, except for the bias-related tests, which were 1 tailed. We used a significance level of P <.05.
RESULTS
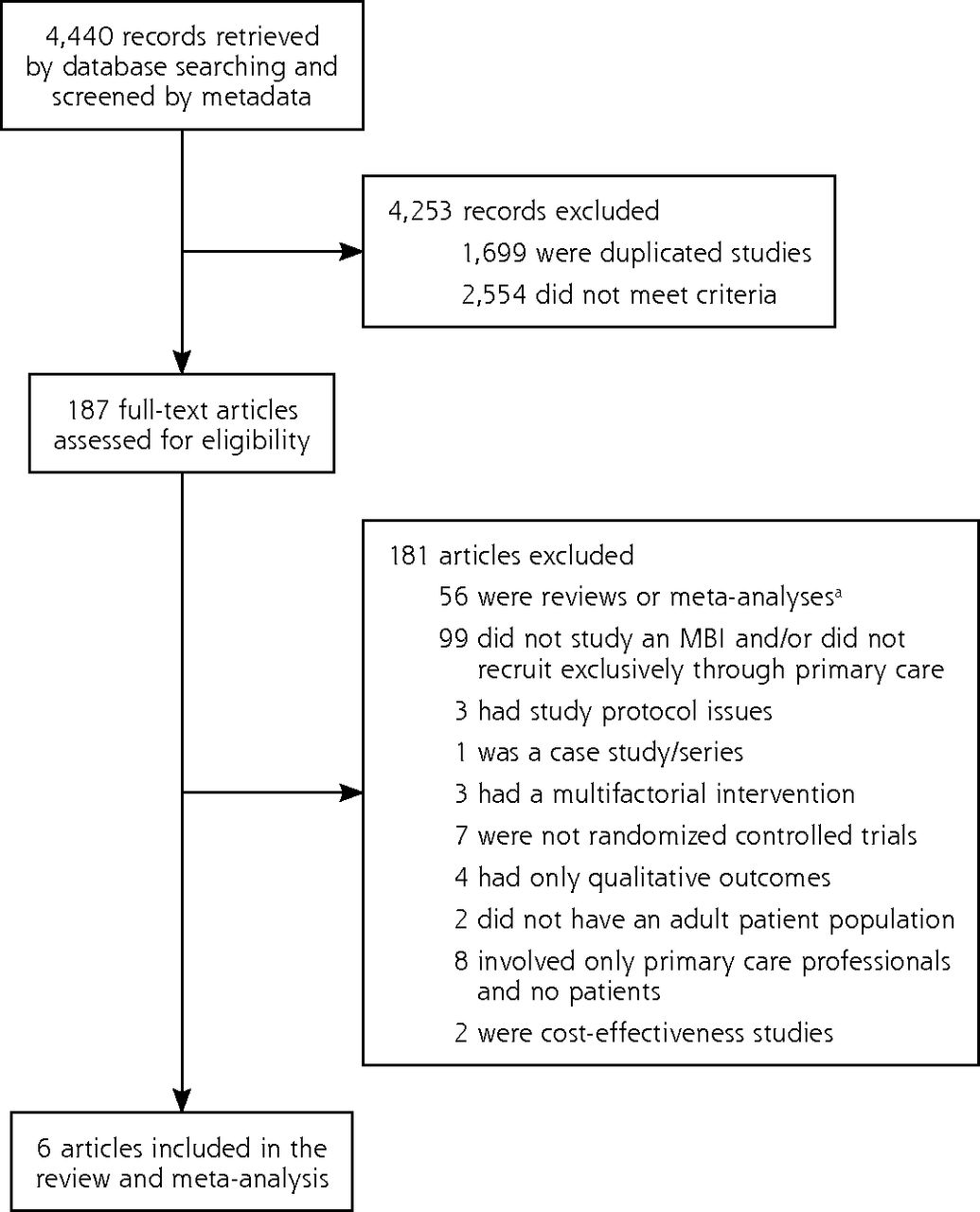
We identified 4,440 records. Ultimately, 6 RCTs were included4,35–39 (5 in English and 1 in Norwegian) representing a total of 553 participants (Figure 1). In the MBI group, 308 participants received the intervention for depression, chronic pain, and medically unexplained symptoms.

Flow diagram of article selection.
MBI = mindfulness-based intervention.
Note: An article may have been excluded for multiple reasons.
aReferences were fully screened to prevent missing studies.
Characteristics of Included RCTs
Table 2 shows the characteristics of the 6 included RCTs, 3 of which applied an MBSR-like program and 3 an MBCT-like program. All tested face-to-face group interventions and were published between 2005 and 2013. The mean age of participants ranged from 43.6 to 69.8 years, and their clinical conditions included chronic musculoskeletal pain, mood disturbance, chronic stress, chronic illness, and medically unexplained symptoms. Most of the trials used 8 sessions, with 1 session each week lasting an average of 2 hours. The control conditions used were wait lists, usual care, and massage or spirituality programs. Measures were collected from posttest to 15 months after intervention, and all outcomes were related to mental health or quality of life.
Characteristics of the Included Trials
Quality of Included RCTs
Two RCTs were considered high quality, and 4 were considered low quality (Table 2).19 Regarding the quality of the interventions, the use of a treatment manual was reported in all trials, therapist training in 3 trials, and treatment integrity in 1 trial. One trial met all criteria, 2 met 2 criteria, and 3 met 1 criterion for the quality of interventions.21
Outcomes
MBI was efficacious for improving general health (g = 0.48), with moderate heterogeneity (I2 = 59; P <.05) (Figure 2 and Table 3). We found no indication of publication bias (Appendix 2, available at http://www.annfammed.org/content/13/6/312/suppl/DC1). MBI was also efficacious for improving mental health (g = 0.56), with a high heterogeneity (I2 = 78; P <.01), and for improving quality of life (g = 0.29), with a low heterogeneity (I2 = 0; P >.05). After adjusting for publication bias (only 1 trial was imputed studies), the effect size for mental health outcomes declined slightly (g = 0.41). We identified no publication bias for quality of life.
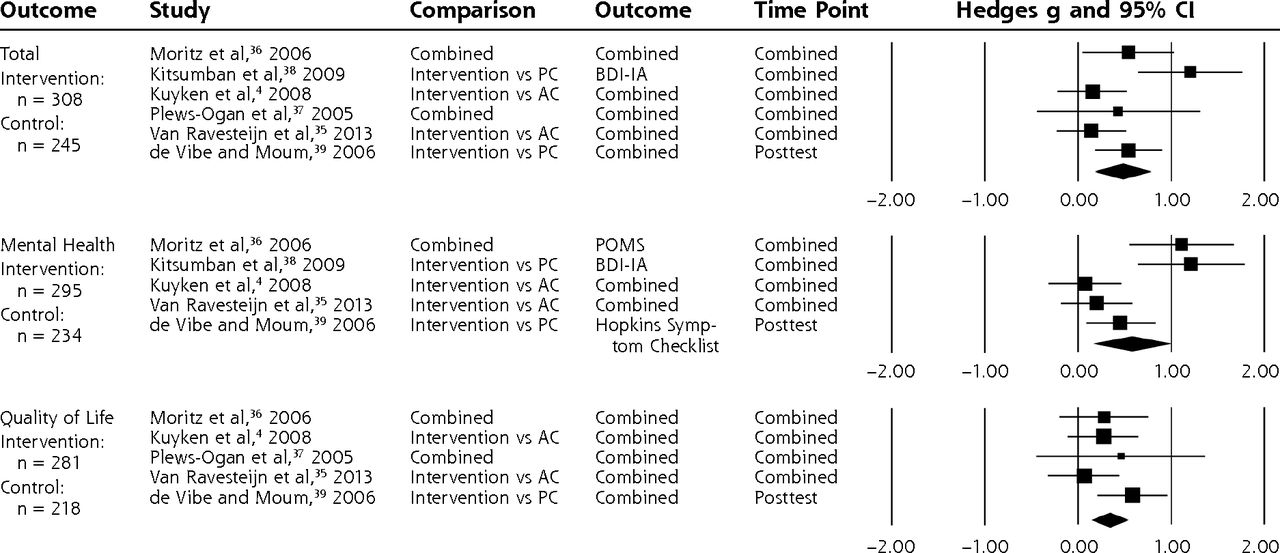
Forest plot for the effect size of mindfulness-based intervention on outcomes overall, and for mental health and quality of life outcomes individually.
AC = active control; BDI-IA = Beck Depression Inventory IA; POMS = Profile of Mood States; PC = passive control.
Combined Effect Sizes and Heterogeneity
We did not find any differences by outcome or intervention, but we did find differences according to the time point of outcome measurement (follow-up of less than 6 months had the greatest effect size, followed by posttest time point and follow-up of greater than 6 months) and type of control (effect size was much greater when MBI was compared with a passive control than with an active control). Heterogeneity was high for 4 characteristics: MBCT, active controls, passive controls, and mental disease. The test of Egger et al33 was significant, with a high risk of publication bias, for MBCT, follow-up of less than 6 months, and use of intention-to-treat analysis, whereas the test of Begg and Mazumdar34 was not significant for any factors. After adjustment, the effect size increased for the posttest time point, active controls, passive controls, and high risk of bias. We did not conduct any subgroup analyses based on the quality of interventions because of the small number of trials.
DISCUSSION
Findings in Context
We found 6 RCTs of MBIs conducted in primary care, which is low compared with the number conducted in secondary or tertiary care.2,3 This disparity may be due to the fact that research in primary care is still comparatively less developed.40
Our analysis showed a moderate effect size in favor of MBIs in primary care for mental health–related outcomes and quality of life, with a low risk of publication bias and a moderate level of heterogeneity. This effect size is similar to that observed across general clinical populations and other settings.2 Primary care could enhance compliance with and adherence to practice and improve the impact of these interventions,14 although this was not evident in our findings. We did not observe evidence that MBIs were explicitly adapted for primary care patients, which may explain lack of relatively greater benefit in this setting.41
Furthermore, the effect sizes for MBIs were similar to those found for pharmacologic and psychological therapies in primary care for such complex disorders as fibromyalgia.13 In subgroup analyses, we observed a large effect size when comparing MBIs with passive control conditions, but not when comparing them with active control conditions. Previous meta-analyses have shown similar results.2,35,42 Khoury et al2 observed a moderate effect size when comparing MBIs with wait list controls, but this effect was small when compared with active controls, and even smaller when including psychotherapy. The authors concluded that MBIs did not differ from cognitive behavior therapies or pharmacotherapy.2 In a meta-analysis of RCTs addressing the efficacy of MBIs against an active control group, Goyal et al3 found small effect sizes for improvements in anxiety, depression, and pain, which were similar to the effects of other active treatments such as cognitive behavior therapy, exercise, other behavioral therapies, or drugs.3 Small or moderate effect sizes for psychosocial interventions similar to pharmacotherapies were expected.43
When comparing the effect of MBI between end of the intervention and follow-ups longer than 6 months, the impact tended to decrease. Interestingly, the effect was greater at a follow-up of less than 6 months than at intervention end; however, this finding may be explained by the passive control used in these studies. In addition, we observed that the MBSR and MBCT models had similar effects (moderate), which supports the hypothesis that MBSR is no different from any other psychotherapeutic intervention. Heterogeneity, however, was significant and much larger than that for MBCT. On the other hand, benefit was greater for mental health outcomes than for quality of life outcomes, although the difference was not significant and heterogeneity was high when it came to mental health outcome, probably because of the different methods used to measure it. Similarly, although the difference was not significant, the impact of MBIs on mental disorders was larger than that on somatic conditions, which could be expected based on previous meta-analyses.2,43
The range of health conditions addressed by MBIs was large, but because of the limited number of studies, we were unable to compare efficacy with that in other levels of health care. MBIs have still not been tested among patients with multimorbidity, even though this population may be a potential target for these interventions.15
Most of the RCTs were classified as being of poor quality (only 2 had a high-quality score), and those with higher quality had a smaller effect size. An intention-to-treat analysis decreased the effect size, although the difference was not significant. Most of the interventions themselves were rated as having a low level of quality, although the importance of strictly following the treatment manual and integrity may be less strict in primary care implementation, and regarding complex interventions such as MBIs. Moreover, information about patient safety, regarding any unintended or adverse effect related to the interventions, has not been reported, although it is not clear whether these potential effects were presented or systematically addressed in the reviewed studies.44–46
Because MBIs have self-efficacy components that support life-long skills, such as self-awareness, emotional self-regulation, less worry and rumination, and meta-cognition,47 these interventions may have more sustainable effects on health in the long term, as shown in recent studies.48 Given limited long-term follow-up studies, the results from this and other reviews remain inconclusive,2,42,49 even though MBIs seem to maintain at least some of their effect size over time.3 Another key question is whether MBIs are cost-effective, and the preliminary results are promising.4,5
In the trials included in this meta-analysis, the contents of MBI programs were not adapted to primary care patients’ local needs, culture, or epidemiology; thus, future protocols should include this framework. Another key component when implementing primary care interventions is the stepped-care approach,14,50 but none of the trials addressed this issue, probably because of the uniformly strict adherence to the manual for MBI programs. On the other hand, when considering the implementation of complex interventions in primary care, professionals and researchers should be more flexible in adapting protocols to the context of this setting within the health system, for example, by using shorter protocols or self-help online interventions.51 Further studies should address this essential point; indeed, many are already including some of these issues, such as the ongoing PREVENT study (Mindfulness-Based Cognitive Therapy Compared With Maintenance Antidepressant Treatment in the Prevention of Depressive Relapse or Recurrence).52
Limitations
We did not include pediatric patients in our analysis, despite the potentially beneficial application of MBIs to this population,53,54 because primary care in many countries does not include children younger than 14 years of age.
Moreover, the number of RCTs applying MBIs in primary care patients is still limited, and our conclusions should be interpreted with caution because of the lack of statistical power. In addition, the overall quality of the included studies was generally low, as they were based on different comparators and outcomes, and had insufficient follow-up time points. Most of the patients were women; although expected in mind-body interventions, this unbalanced sex distribution may bias results. We found moderate levels of heterogeneity among trials, and they remained substantial after pointing out possible sources of variance, stratifying with the mixed effects model, and using combined outcomes with a pooled mean. As we have seen, the outcomes assessed respond to a wide variety of symptoms, from mental health to quality of life; however, heterogeneity seems to be concentrated in mental health outcomes. This pattern could be due to the different instruments used across trials. On the other hand, the comparisons with both active and passive controls showed significant differences between them, with high heterogeneity; therefore, another important part of heterogeneity could respond to differences in comparison groups according to the control used, as shown in previous studies.2
Implications for Practice
This meta-analysis is the first to address the efficacy of MBIs in primary care patients. There is still insufficient evidence to draw a conclusion about the effects of mindfulness interventions in this setting, and well-designed RCTs and translational studies in this context are needed. Our results, however, suggest that these psychosocial complex interventions are promising for this particular clinical population and level of care. Several questions remain unanswered, and future research protocols addressing the implementation of MBIs in primary care are greatly needed. Some recommendations, such as addressing MBIs as complex interventions, considering a stepped-care model, and evaluating adaptation of these interventions to the needs and culture of patients and primary care services and their implementation process could affect outcomes and should be tested in further studies. The use of active and similar comparators, the evaluation of the long-term cost-effectiveness of these programs, and a systematic search for potential adverse effects of MBIs also seem to be necessary, to refine these results and to generate more robust evidence on the impact of MBIs in primary care and the health system.
Acknowledgments
Dr Demarzo is grateful to the CNPq - Brazilian National Council for Research and Technology Development for his postdoctoral fellowship (Science Without Borders Programme). The authors are grateful to Dr Svein Gjelstad for his translation of the article from Norwegian.
Footnotes
Conflicts of interest: authors report none.
Supplementary materials: Available at http://www.AnnFamMed.org/content/13/6/573/suppl/DC1/.
- Received for publication November 28, 2014.
- Revision received June 19, 2015.
- Accepted for publication July 16, 2015.
- © 2015 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}