
Abstract
PURPOSE Dementia case management (CM) in primary care is a complex intervention aimed at identifying the various needs of patients with dementia and their caregivers, as well as the organization and coordination of care. A key element of CM is the collaboration of family physicians with case managers. We conducted a systematic mixed-studies review to identify the needs of the patient-caregiver dyad and the effects of CM.
METHODS We searched MEDLINE, PsycINFO, and EMBASE up to October 2014, regardless of the study design. Our main outcomes were needs of patients and their caregivers and the effects of CM on these needs. We used narrative syntheses to develop a taxonomy of needs and to describe the effects of CM on those needs. We used meta-analysis to calculate the prevalence of needs and the standardized mean differences to evaluate the effects of CM on the needs identified.
RESULTS Fifty-four studies were included. We identified needs of the patient-caregiver dyad and needs of the patient and caregiver individually. CM addressed the majority of the identified needs. Still, some very common needs (eg, early diagnosis) are overlooked while other needs (eg, education on the disease) are well addressed. Fully establishing the value of CM is difficult given the small number of studies of CM in primary care.
CONCLUSIONS There is good evidence that case managers, in collaboration with family physicians, have a pivotal role in addressing the needs of the patient-caregiver dyad.
INTRODUCTION
The proportion of people with dementia is growing dramatically. According to the US Alzheimer’s Association, by 2030, 50% of Americans aged 65 years and older will be diagnosed with dementia.1 In Canada in 2011, 747,000 Canadians lived with cognitive impairment.2 Today, the combined costs are $33 billion per year,1 and they are projected to increase to $872 billion by 2038.3,4 Worldwide, dementia is the main contributor to disability-adjusted life years (11.2%), representing a greater burden than cerebral vascular accident (9.5%), heart disease (5.0%), or cancer (2.4%).5
People with dementia need help with challenging changes in behavior, memory, physical disability, and mood.6 The main source of help is family caregivers, who often suffer from the burdens of caregiving and from depression and health problems.7 It has been shown that early intervention makes the greatest difference in management of symptoms.1 The World Health Organization states that it would be challenging to intervene without effective involvement of primary care.8 Dementia case management (CM) interventions are becoming a central component of primary health care organizations in North America and Europe.9–12 According to the Case Management Society of America, case management is “a collaborative process of assessment, planning, facilitation, care coordination, evaluation, and advocacy for options and services to meet an individual’s and family’s comprehensive health needs through communication and available resources….”13 Case managers are health care professionals who provide follow-up, coordinate individual care, and liaise with other health care services. They work in collaboration with family physicians, specialists, or both.14–22
Over the last few years, several systematic reviews have found that the evidence of CM’s effects on service use and clinical outcomes is weak.23–28 None of them specifically focused on the needs of patients and caregivers, however.23–28 Patients with dementia and their caregivers who already receive professional care still report unmet needs.29 Moreover, they feel that their own opinion is not taken into account.30 In line with the patient-centered care paradigm,31,32 it is important to identify the needs felt by the patient and the caregiver33–35 and to determine the extent to which CM interventions respond to their needs.36
We conducted a systematic review to answer the following research question: Does the collaboration of family physicians with case managers respond to the needs of patients with dementia and their caregivers living in the community?
METHODS
We conducted a systematic mixed-studies review by including studies with diverse designs (quantitative, qualitative, and mixed methods).37 This type of review has been deemed appropriate for the study of complex interventions.38 It overcomes the issue of a partial picture that results from relying on a single type of research in isolation, assists in the critical analysis of interventions from the viewpoint of participants targeted,39 and enables a single review to answer a number of questions (eg, identifying needs and evaluating how well they have been met).40 It produces research more useful for decision makers and maximizes the use of review results (maximizes the conversion of knowledge to action) by enhancing their utility and impact.39
Inclusion Criteria
To be included in our review, studies had to meet the following criteria:
They had to deal with community-dwelling patients of any age with any type of dementia and/or their informal caregivers.
They had to concern collaboration between a family physician and a case manager that comprises a comprehensive needs and health assessment, planning of services and their coordination, monitoring, and regular proactive follow-up.13,41
They had to focus on primary medical care, defined as a range of community settings where family physicians intervene (patients’ homes and offices).42
They could be of any type or design.
Their outcomes could be the effects of CM on any type of need expressed by patients, expressed by caregivers, or measured.
Search Strategy and Study Selection
In accordance with PRISMA statement standards,43 a literature search was conducted by a specialized librarian; publications in English, French, or Russian listed in MEDLINE, PsycINFO, or EMBASE, published before October 2014, were searched (Supplemental Appendix 1, available at http://annfammed.org/content/14/2/166/suppl/DC1). Given the objectives of our review, 2 search strategies were applied in parallel: 1) studies of the needs of community-dwelling patients with dementia and their caregivers, and 2) studies of CM (Supplemental Figure, available at http://annfammed.org/content/14/2/166/suppl/DC1). Based on the eligibility criteria, relevant titles, abstracts, and full-text articles were selected independently by 1 author (V.K.) and a research assistant (Martin Beauchamp).
Quality Assessment
The quality of the studies was assessed independently by 1 author (V.K.) and one outside reviewer (Quan Nha Hong, MSc) using the validated Mixed Methods Appraisal Tool designed for the critical appraisal of studies with diverse designs.44–46 Studies were scored on their internal and external validity (eg, representativeness of the sample, randomization). Studies were included without regard to their quality. We performed a sensitivity analysis (with a potential score of 0 or 1) to assess the impact of lower-quality studies on the results.
Data Extraction and Synthesis
Two reviewers (V.K. and Beauchamp) independently extracted and coded data; discrepancies were resolved through consensus. We used a 3-step approach to synthesize the findings:
We defined a need as a perceived state of deprivation communicated by patients or their caregivers.6 The prevalence was extracted if it was reported. Needs expressed in other domains measured by instruments were also searched (eg, domains of quality of life).6 We used a narrative synthesis approach to develop a taxonomy of the needs and meta-analysis to evaluate their prevalence.
A narrative synthesis approach was applied to describe the key components of CM.
A narrative synthesis was used to describe CM effects on the needs (mapping of CM components to the needs identified in Step 1) and a meta-analysis to estimate their effects.
Narrative synthesis was the main analytical approach we used, while meta-analyses were performed to explore the observed effects (Table 1).
Description of Synthesis
RESULTS
Fifty-four studies were included in the review: 46 on the needs of patients and their caregivers52–98 and 8 on CM (Supplemental Figure, available at http://annfammed.org/content/14/2/166/suppl/DC1). The characteristics of the included studies are presented in Table 2, and Supplemental Appendixes 2 and 3, available at http://annfammed.org/content/14/2/166/suppl/DC1.
Summary Characteristics of Included Studies
Identification of Needs
Three main categories of need were identified and are presented in Table 3: needs of the patient-caregiver dyad, needs of the patient, and needs of the caregiver. Many needs are common to patients and caregivers. The needs reported by the largest number of studies are needs of the dyad: for education or counseling on the disease (32 studies) and early diagnosis (13 studies).
Needs of Community Dwelling Patients With Dementia and Their Caregivers
Meta-analyses showed that 58% (95% CI, 43%–72%) of caregivers were in favor of early dementia diagnosis, 50% (95% CI, 35%–65%) were in need of education on the disease, and 23% (95% CI, 17%–31%) needed in-home support (Table 4). Needs for meaningful activities that patients could participate in and assistance with daily activities were reported by 36% (95% CI, 5%–85%) and 22% (95% CI, 5%–59%) of patients with dementia respectively.
Meta-Analysis of Needs of Patients and Their Caregivers
Description of Care Management
A key component of CM apparent in the studies we examined was close collaboration between case managers and family physicians (Supplemental Appendix 3, available at http://annfammed.org/content/14/2/166/suppl/DC1). The case managers involved were nurses specialized in care of the elderly.14–18,20 They were responsible for the coordination of treatment plans and for providing services. Through phone calls, web-based interactions, and case discussions, case managers communicated regularly with family physicians to inform them about patient and caregiver health conditions and needs.14–22 The role of family physicians was to develop care plans, provide medical treatment, and to modify care plans based on updates from case managers.
We mapped the components of CM to the needs identified from the perspectives of the patients and their caregivers (Table 5). To meet the needs of the patient-caregiver dyad, case managers performed the prediagnostic work-up to assist family physicians with diagnosis.21,22 They provided education on the disease, prognosis, treatment,16,17,19,21,22 and problematic home situations.18 They counseled on available resources/services,16,20 legal and financial issues, and advance directives.14–16 Finally, case managers coordinated medical and community services via electronic, written, and case conference discussion.14–17,19,20
Mapping of Components of Case Management to Needs and Their Effects on the Needs
To meet the needs of patients, case managers applied, in collaboration with family physicians, non-pharmacologic and pharmacologic protocols for management of daily activities,14–16 behavior distress,14–16,21,22 cognition,14–16 mood,14–16 and home safety.16,18,19
To meet the needs of caregivers, case managers provided support sessions and non-pharmacologic interventions for stress management14,15,17 and coping skills.14 They also developed care plans14–18,20–22 and coordinated home care services16–18 and social services.16,17,21,22
Evaluation of the Effects of Care Management
CM was able to address almost all identified needs (Table 5). The number of diagnoses made by family physicians working with case managers increased while the rate of diagnosis by specialists without case managers remained stable.21,22 CM led to better education on the disease15,16,20 and provision of sufficient information on dementia-specific community resources.15,20 No effect on the understanding of medical treatment and knowledge of dementia was shown in 1 study, however.16 CM proved to establish good coordination of health care services, continuity, and quality of care,14–17 except in 1 study.18
CM also better addressed the needs of patients. More patients received non-pharmacologic behavioral protocols.16 Acetylcholinesterase inhibitors were more frequently prescribed by family physicians working with case managers, while neuroleptics prescription decreased.21,22 More patients were enrolled in the Safe Return program.16
CM also showed effects on the needs of caregivers. Caregivers’ confidence with care increased.16 Their decision-making capacity improved,15,16 as did satisfaction with social support,16 and in-home help (eg, cleaning services).16,17 Moreover, caregivers were actively involved in care-plan development and regular discussion of the patient’s health problems.16,17
The effects on the needs for early diagnosis, financial and legal aspects of the disease, and meaningful activities were not studied. CM was not found to have any effect on patients’ daily activities, cognition and depression.
A meta-analysis of the effects of CM (Figure 1 and Supplemental Appendix 4, available at http://annfammed.org/content/14/2/166/suppl/DC1) showed a significant decrease in behavioral disturbance of patients as a result of psychosocial interventions along with acetylcholinesterase inhibitors (standardized mean difference [SMD] −0.27, 95% CI, −0.53 to −0.01, P = .04)14,17 and a significant increase of confidence in caregiving (SMD 0.19, 95% CI, 0.01–0.37, P = .04) due to the education in coping skills.16,17 The effect on depression of caregivers was uncertain (SMD −0.23, 95% CI, −0.46 to 0.01, P = .06),14,17,18 and there was no effect on caregivers’ burden (SMD 0.17, 95% CI, −0.18 to 0.52, P = .34).
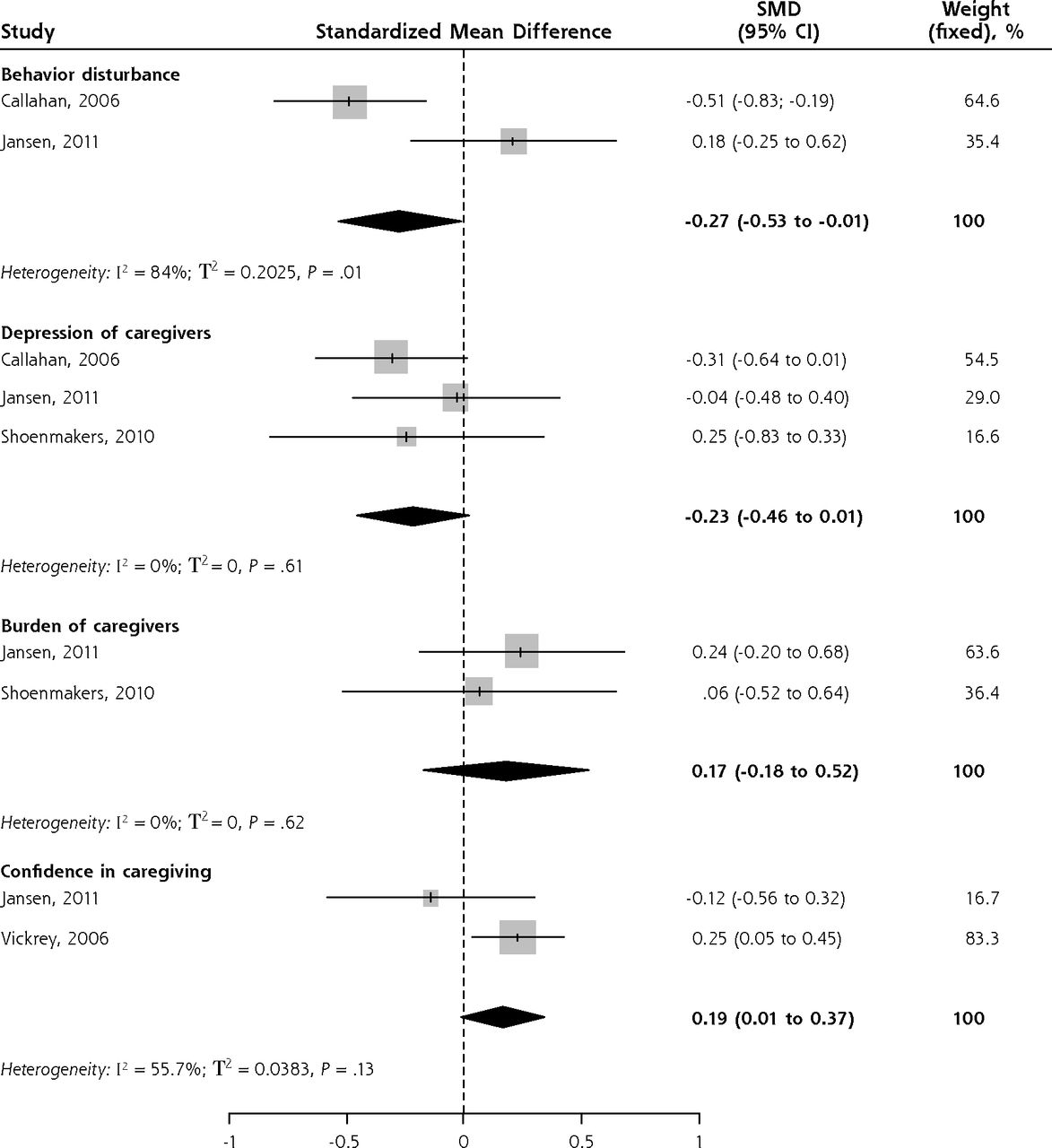
Forest plot of standardized mean differences of case management vs control by subgroups.
Quality of Evidence
Almost all studies (43 studies) of the needs of the dyad and all 8 studies of CM proved to be of high quality. The majority of RCTs clearly described the randomization, blinding, and drop-out rate. Most non-randomized and quantitative descriptive studies (surveys) reported adequate sampling strategies and measurements. Qualitative studies clearly described their inclusion and exclusion criteria, methods of analysis, and contexts. Exclusion of studies of lower quality did not change the overall results (Supplemental Appendix 5, available at http://annfammed.org/content/14/2/166/suppl/DC1).
DISCUSSION
This is the first systematic mixed-studies review conducted to evaluate whether CM meets the needs of patients with dementia and their caregivers. The main novelty of our review is that we first identified the needs from the perspectives of patients and their caregivers and only then evaluated whether CM targeted their needs and led to the desired outcomes. Our systematic review showed that CM addressed most needs of patients and caregivers. It also demonstrated that some very common needs (eg, early diagnosis) are still overlooked, while other needs (eg, education/information) are well targeted.
The most frequently reported need was early diagnosis of dementia. The impact of CM on this important need, however, has not been evaluated. While there is no consensus among health care professionals on the early diagnosis of dementia,100–103 our systematic review suggests that patients and their caregivers would like to receive an early diagnosis. Early diagnosis of dementia does not necessarily change the disease’s course,104 but it prompts health care professionals to identify the needs earlier and thus sustain the quality of life for both the patient and the caregiver.105 Moreover, it may positively affect appropriate medication prescription, decrease levels of caregiver burden and depression, and diminish the risk of early placement in a long-term care facility.106,107
The second most frequently reported need was education and counseling on the disease. This finding is in line with those of previous research, which has showed that most unmet needs were related to a lack of knowledge about the existing services, progression of dementia, and management of behavioral problems.29,79,108,109 Unlike early diagnosis, this need seems to be well targeted and appropriately addressed by CM.
Identification of the needs of patients and their caregivers is the basis for the development of interventions sensitive to these needs.6 CM focuses on integration of medical and community services to deliver patient-centered care according to the specific needs of individual patients.13 The key element of CM is the collaboration of case managers with family physicians. Regular communication between case managers and family physicians is essential to the patient-centered care targeting these vulnerable populations; it allows family physicians to make timely modifications of their care plans.
Formal training of case managers in care of the elderly is a valuable asset to the care.14–18,20 Case managers specialized in dementia care can assess needs promptly and follow up regularly. For instance, they are better able to evaluate the needs of patients with regards to daily activities and orient them to the appropriate services (eg, mobility improvement programs).14–16 They also assess the needs for information and support and guide the patient-caregiver dyad to the appropriate services (eg, the Alzheimer Society or the Alzheimer’s Association).15,16,20 Moreover, as the first point of contact for the dyad, they appear to be more easily reachable than family physicians.14–18,20–22 Our previous studies demonstrated that the effectiveness of CM depends on a small caseload, regular and proactive follow-up, and transparent communication among health care professionals.110,111
Limitations
As in any systematic review, we may have missed studies that we should have included. It is unlikely, however, that we missed large studies, as the literature search was comprehensive and included publications in 3 languages (English, French, and Russian). The meta-analysis of the effects of CM was conducted on a limited number of available studies, but it was exploratory; its conclusion should be considered with caution. The limited number of available studies on CM in which family physicians collaborate with case managers necessarily limited our review.
Future Research
Future studies are needed to evaluate the effects of CM on the needs that are overlooked—early diagnosis of dementia, legal issues, and financial issues. An avenue for some future studies could be the integration of social workers into primary care to assist with financial and legal issues of the dyad.16 Family physicians and researchers should perceive the needs of the dyad as unique features of patient-centered outcomes research related to primary care.
Acknowledgments
The authors would like to thank Alina Dyachenko, biostatistician, St Mary’s Research Center, McGill University, for her assistance with statistical analysis; Muriel Gueriton, specialized librarian, Solidage, McGill University - Université de Montréal Research Group on Frailty and Aging, for her assistance with literature search; Quan Nha Hong, McGill University, for assistance with the methodological quality assessment; research assistant Martin Beauchamp for assistance with study selection; Daniëlle Jansen, Birgitte Schoenmakers, and Richard Fortinsky for sharing the data.
Footnotes
Conflicts of interest: authors report none.
Previous presentation: The study was conducted by the first author as a scholarly project at the Family Medicine residency program of the McGill University; St. Mary’s hospital, Montreal, Canada. The preliminary results have been presented at the North American Primary Care Research Group (NAPCRG) conference, New York, New York, November 22 – 25, 2014, and received the Patient Choice Award http://www.annfammed.org/content/13/3/286.full.
Supplementary materials: Available at http://www.AnnFamMed.org/content/14/2/166/suppl/DC1/.
- Received for publication June 6, 2015.
- Revision received October 15, 2015.
- Accepted for publication November 8, 2015.
- © 2016 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Collaboration and coordination of health and care services for older people with dementia by multidisciplinary health and care providers: a scoping review protocol
- Effectiveness of different post-diagnostic dementia care models delivered by primary care: a systematic review
- Improving Prediction of Dementia in Primary Care
- In This Issue: Confronting Constraints on Individual Behavior & Outcomes