
Article Figures & Data
Figures
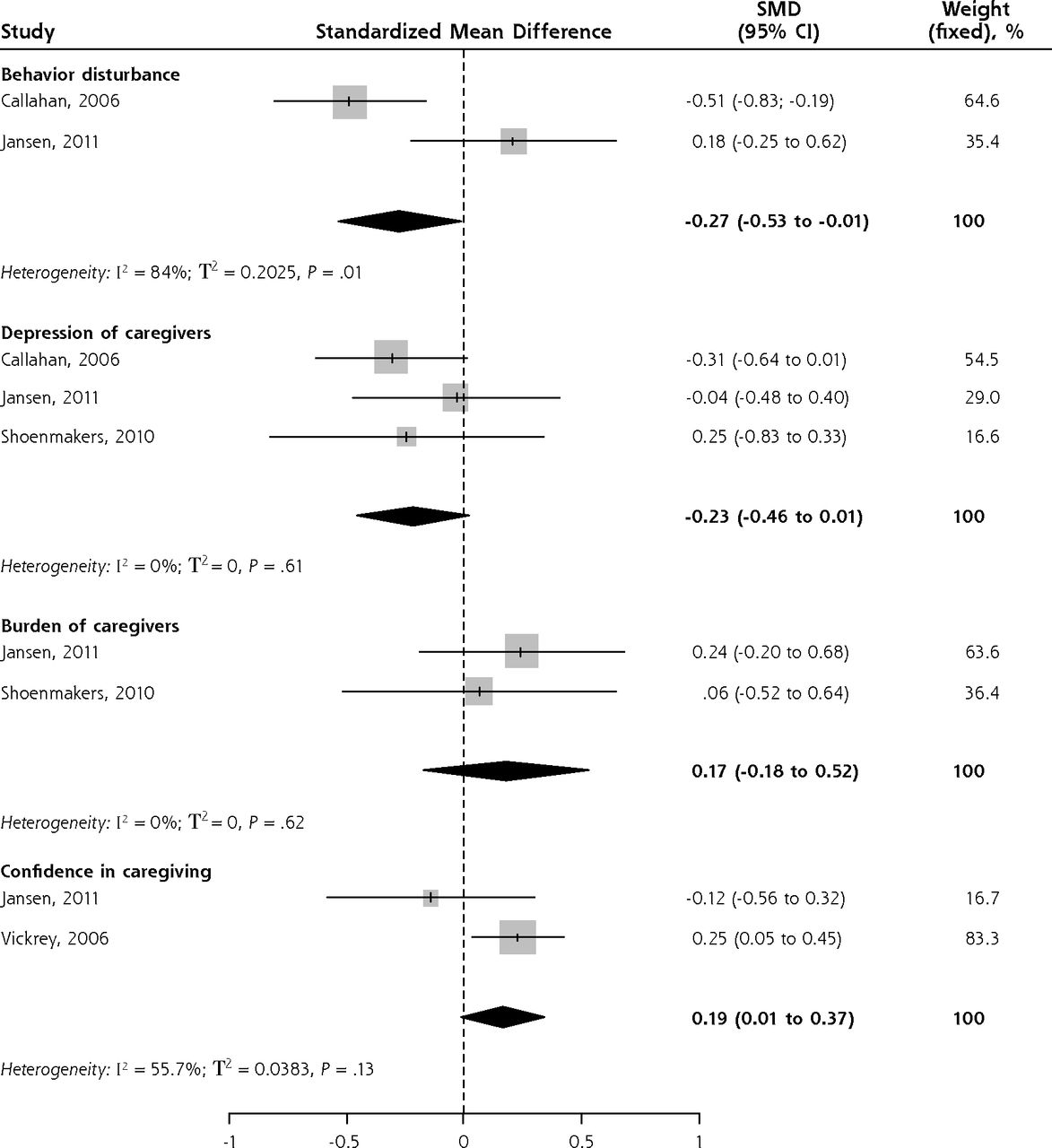
- Figure 1
Forest plot of standardized mean differences of case management vs control by subgroups.
Tables
Step 1. Identification of the needs by narrative synthesis and meta-analysis Narrative synthesis (main approach) Through a narrative synthesis, we developed an integrated interpretation of various primary studies from which conclusions may be drawn.47 This synthesis provides qualitative rather than quantitative data.48 We followed a narrative approach that includes textual description of studies on needs of the patient and caregiver, extraction of the needs and their grouping into categories based on their common features (eg, education on disease), and then transforming data into common rubrics (taxonomy development).37 We divided the identified needs into 3 categories: needs of the patient, needs of the caregiver, and needs common to both (needs of the dyad). Meta-analysis We performed a meta-analysis on quantitative studies only to determine the prevalence of the needs identified. Starting with the prevalence proportions extracted from each study, we used R 3.1.2 (The R Foundation) to calculate the pooled prevalence proportion and 95% confidence interval for each need.49 We employed random-effects models, since the studies were statistically and methodologically heterogeneous. The I2 statistic was used to measure heterogeneity. Considering the context (needs are generally evaluated in the observational studies) the meta-analysis included studies of different designs (eg, nonrandomized studies and surveys).50 Step 2. Description of case management Narrative description We described the main features of CM according to the definition of the Case Management Society of America,13 then mapped the various components of CM to the needs identified in Step 1 that they targeted. Step 3. Evaluation of case management effects by narrative synthesis and meta-analysis Narrative synthesis (main approach) We followed the same narrative synthesis approach as in Step 1 to develop a textual description of the effects of CM on the subcategories of needs: mapping the components of CM to the needs identified in Step 1 from the perspectives of the patients and their caregivers.37 Meta-analysis We then conducted a meta-analysis to explore the potential effects of CM on the identified needs where data were available. At this point, we included only randomized controlled trials at 12 months follow-up. Meta-analyses were conducted on the effects of CM on needs (eg, the need for confidence in caregiving) and on surrogate markers of needs (eg, behavior management as a surrogate for behavior disturbance of the patient and emotional support as a surrogate for depression and burden of the caregiver). To evaluate the intervention effect, we calculated the standardized mean differences between groups along with 95% confidence intervals, since different scales were used to measure the same outcome. To obtain missing data, we contacted the authors. Fixed-effects models were used because of the small sample size (2 in each outcome evaluation).50,51 CM = case management.
Characteristics Description Studies of Needs Studies of CM Continent/country: Americas, (16 studies) USA61,62,66,73,74,76,81,85,91,93,95,97 USA14–16 Canada84 Europe (21 studies) UK20,52,53,64,69,72,77,78,83,84,99 UK20 The Netherlands17,19,54,75,79,86 The Netherlands17,19 Sweden21,22,70 Sweden21,22 Norway97 Belgium18 Italy85 Oceania (5 studies) Australia65,67,88,98 … New Zealand71 Asia (7 studies) China68 … Hong Kong90,96 Singapore59 Japan82 Pakistan57 Turkey58 Africa (1 study) Tanzania55 … Multiple countries (3 studies) UK – Poland87 … USA - Canada56 Germany – UK – France – Poland – Spain – Luxembourg94 Type of studies 12 NRS74–86 5 RCTs14,16–19 11 quantitative descriptive studies87–97 2 NRS15,20 22 qualitative studies52–73 1 quantitative descriptive study21,22 1 mixed methods study98 Demographic characteristics of participants Age of patients (caregivers), mean, y 77 (58) 79 (61) Type of dementiaa Alzheimer’s disease, % 59.8 57.6 Vascular dementia, % 14.0 17.0 Early onset of dementia 3 studies53,54,88 Frontotemporal dementia 2 studies56,89 Severity of dementia Mild to moderate Mild to moderate CM = case management; NRS = nonrandomized studies; RCT = randomized controlled trial.
↵a All studies concerned mild-to-moderate dementia. Percentages given are percentages of patients in pooled study populations.
Categories of Need Description No. of Studies Needs of the patient/caregiver dyad Early diagnosis52–54,56,64–66,73,80,85,87–89 Need for early diagnosis (to understand the behavioral problems and gain timely access to resources). 13 Education/counseling54–52,59–68,72–75,79,80,82,85–89,92–97 Need for specific information on medical and interpersonal aspects of the disease, meaningful counseling on dealing with behavioral problems, guidelines on dementia before and after diagnosis. 32 Information about relevant services65,74,75,82,83,85,89,92,94,96,98 Need for an overview of available formal care services such as community psychiatric services, domestic help, caregivers’ support groups, and insurance. 11 Legal assistance66,85,93,97 Need for assistance with legal documents and advice on guardianship, power of attorney, etc. 4 Financial support/planning53,55,57,59,66,88,89,92,93,96,97 Need for assistance with access to financial programs that can help if the caregiver quits a job to take care of the patient and help deal with household and medication expenses. 11 Advance care planning85 Need for information on future care problems. 1 Care coordination/continuity of care/well-defined care pathway52–54,64,65,67,68,73,86,98 Need for continuity between the various health care services involved, access to services corresponding to the severity of the disease, support throughout the course of the disease from the same health care professionals, and coordination of medical and community services to optimize services and prevent overlap. 10 Access to family physicians trained in geriatrics52–54,66,86,88,92 Need for access to a family physician who has adequate knowledge of the disease, is sensitive to the concerns of patient and caregiver, can provide guidance on demen tia, and can follow patients with dementia and their caregivers. 7 Access to other health care professionals trained in geriatrics65,70,73,81,86–88 Need for access to health care professionals who know the disease, respond competently at disclosure of the diagnosis, and communicate test results clearly. 7 Needs of the patient Meaningful activities60,74,77–79,84,85,90,95 Need to take part in activities, join in with others, do things, and have company. 9 Assistance with ADL/IADL57,68,74,76,79,84,85,87,88,91,97 Need for help with ADL (commonly for bathing/dental care, dressing, and walking) and with IADL (commonly for housekeeping, meal preparation, and transportation). 11 Behavior management63,75,84,87,88,90,91,95,97 Need for pharmacologic and nonpharmacologic approaches to managing the behavioral spectrum of the disease, especially agitation and restlessness, verbal aggression, and anxiety. 9 Cognition management79,84,87,88,90 Need for pharmacologic and nonpharmacologic approaches to managing the cognitive spectrum of the disease. 5 Management of mood swings/depression77–79,84,90,93,97 Need for pharmacologic and nonpharmacologic approaches to managing depression. 7 Safety69,74,77,78,84,85,91,97 Need for help in managing fall and wander risk, ensuring home safety, and minimizing the risk of accidental self-harm. 8 Needs of the caregiver Emotional support53,57,59,62–64,74,80,95,97 Need for assistance with feelings of being alone, abandoned, helpless, exhausted, and mentally burdened. 10 Social support53,56,58,59,62,67,75,81,87,88,91,97 Needs to have social outlets such as time alone, social interaction with friends, opportunities to shop and to go out. 12 In-home support55,58,66,75,83,95 Need for help with house chores (eg, cleaning). 6 Capacity to provide care62,63,80,87,89,90,96,97 Need for training in communication skills and in strategies for handling maladaptive behaviors and. 8 Involvement in care planning65 Need to be included as an equal partner in formal and informal care planning. 1 ADL = activities of daily living; IADL = instrumental activities of daily living.
Note: Needs for help with urinary incontinence,66,84 help with sight and hearing problems,77,78,97 and culturally sensitive services61 are not presented in the table, since only a few studies evaluated these needs.
Categories of Need No. of Studies Pooled Proportion (95% CI) Variation Across Studies (I2), % Test of Heterogeneity (Q2), P value Needs of the patient-caregiver dyada Early diagnosis80,88,89 3 0.58 (0.43–0.72) 80.0 .007 Education/counseling on disease79,80,82,89,92,94–96 8 0.50 (0.35–0.65) 97.3 <0.001 Needs of the patientb Meaningful activities74,79,85 3 0.36 (0.05–0.85) 97.8 <0.001 Assistance with ADL/IADL74,79,85 3 0.22 (0.05–0.59) 95.5 <0.001 Needs of the caregivera In-home support75,83,95 3 0.23 (0.17–0.31) 17.7 0.30 Categories of Need Corresponding Components of Case Management Resultant Effects Needs of the patient/caregiver dyad Early diagnosisa Gathering information through the basic diagnostic battery to help family physicians establish a diagnosis21,22 Dementia diagnosis increased in primary care while remaining stable in specialty care21,22 Education/counseling on disease Holding interactive seminars and family meetings for patients and caregivers on relevant care issues16,17
Providing information by phone to caregivers17,18
Helping the patient and family understand the disease, prognosis, and rationale of treatment19,21,22
Exploring problematic home care situations18Caregivers understood medical treatment for behavior and depression: 78.4% vs 72.2% in usual care (P = .49)6
Perception of caregiver’s clarity in discussing patient’s care: 16.8% vs 21.3% of usual care (P = .01)16
100% of caregivers were satisfied with the ability of case managers to answer questions15
Educational material was relevant to the dyad situation in 95% of cases15
95% of caregivers were satisfied with quality of educational material provided15
A majority of caregivers were satisfied with information allowing them to understand the nature of the disease20
Caregiver knowledge about dementia was not improved (P = .19)16Information on relevant services Recommending caregiver resources—eg, Alzheimer’s Association, meals on wheels, and Safe Return program (for wandering)16
Helping with various services (day care, respite care)2097% of caregivers were satisfied with the information they received on community resources15
Caregivers were more aware of dementia-specific resources20Help with legal issues Educating caregivers on legal issues14,15 Not evaluated Financial support and planning Educating caregivers on dementia-related financial planning14–16 Not evaluated Advance care planning Advising on advance directives16
Interactive seminars for caregivers on evaluation of decision-making capacity16With CM, advance directives were discussed or completed and documented in 69.4% of cases, vs 44.4% in usual care (P = .001)16
Decision-making capacity improved in 34.2% of patients vs 9.7% in usual care (P = .001)16
90% of caregivers were satisfied with future planning15Care coordination, continuity of care, and a well-defined care pathway Communicating regularly with family physicians,14,15,17,19 maintaining written consultation notes,14,16 producing secure electronic updates,15 via web-based systems,14,16 and attending case conferences14,20
Connecting patients and their caregivers to support services16,17,19
Operating in conjunction with any services patient already had2070% to 82.8% of caregivers rated a new way of primary care delivery as very good/excellent14
88% of caregivers were satisfied with the care coordination provided17
100% of caregivers stated that intervention was efficient17
95% of caregivers were satisfied with the ability of case managers to link them with community resources15
The quality of patient’s health care improved (P = .003)16
1 study found no difference in interdisciplinary communication between intervention and usual care group (P = .5)18Access to health care professionals trained in geriatrics Case managers are trained in geriatrics/geropsychiatry,14–18,20 communicating the diagnosis to the families,14 skills in communicating with patients and their caregivers,17 dementia home care18
Involving a multidisciplinary team in patient care (eg, geriatrician, geriatric psychiatrist, and psychologist)14
Helping with access to health care professionals19
Referring to specialists if needed17,21,22Not evaluated Access to family physician trained in geriatrics No prior formal training of family physicians in geriatrics Not evaluated Needs of the patient Meaningful activities Providing patient exercise guidelines and resources (eg, group chair-based exercises)14,15 Not evaluated Assistance with ADL/IADL Advising on implementation of predictable routine of daily activities16
Providing nonpharmacologic protocols that include mobility management, personal care concerns14,15No effect14,18 Behavior management Arranging interactive seminars for caregivers on evaluation of acute behavior changes16
Providing specific protocols and nonpharmacologic interventions for repetitive behavior, agitation, aggression, delusions or hallucinations14–16
Providing drug therapy with anticholinesterase inhibitors and memantine14,16,21,2247.2% Received as much help as needed with behavioral problems vs 29% in usual care (P = .01)16
The rate of antidementia medication prescription by family physicians was increased from 42% to 86% and the rate of neuroleptic prescription decreased21,22Cognition management Assessing patients’ memory regularly14–16
Educating on communication14 and applying nonpharmacologic protocols that include communication techniques15No effect14 Management of mood swings/depression Providing a specific protocol of nonpharmacologic interventions on depression, with drug therapy as a backup14,15
Arranging interactive seminars for caregivers on managing depression in patients16No effect14,18 Safety Making recommendations on home safety and the Safe Return program (for wandering)16
Providing personal alarms18
Assessing the patient’s home situation19 Guiding the caregiver in organizing home care1827.3% of patients were enrolled in Safe Return vs 8.4% in usual care (P = .001)16 Needs of the caregiver Emotional support Providing support sessions focused on caregiver stress14,17;
Recommending nonpharmacologic protocols that includes stress management15In 2 studies, caregiver mood improved at 12 months (P = .03)14,18; another found no effect at 18 months(P = .33)14
Caregiver burden was not affected (P = .49)17,18Social support Recommending a caregiver support group16;
Organizing family meetings aimed at improving social support and relieving the primary caregiver17,21,22Caregivers’ support systems were adequate in 80.4% of cases vs 45% in usual care (P = .001)16
40.7% of caregivers received services vs 19.2% in usual care (P = .002)16
Caregivers were socially supported (P = .03)16In-home support Helping with home care,17,18 meals on wheels,16 and dinner services17 38.7% of caregivers received in-home help vs 28.9% in usual care (P = .02)16
100% of caregivers were satisfied with home help17Capacity to provide care Educating caregivers on coping skills14 Caregiver confidence and mastery were greater in CM (P = .001)16 Involvement in care planning Involving caregivers in individualized care plan and problem list development14–18,20–22 38.2% of caregivers were involved in care plan development vs 22.1% in usual care (P = .001)16
In 82.5% of cases, caregiver gave input on behavior issues vs 39% in usual care (P = .001)16
96% of caregivers were satisfied with discussion of patient’s health problems17ADL = activities of daily life; CM = case management; IADL = instrumental activities of daily living
↵a Only 1 of the studies on CM interventions enrolled patients not already diagnosed with dementia.21
Supplemental Appendix and Tables
Supplemental Appendix and Tables
Files in this Data Supplement:
- Supplemental data: Appendix & Tables - pdf file
The Article in Brief
Family Physician-Case Manager Collaboration and Needs of Patients With Dementia and Their Caregivers: A Systematic Mixed Studies Review
Vladimir Khanassov , and colleagues
Background Patients with dementia and their caregivers who already receive professional care still report unmet needs. This analysis of existing research sets out to determine whether case management (the collaboration of family physicians with case managers) responds to the needs of patients with dementia living in the community and their caregivers.
What This Study Found Case management addresses the majority of needs of dementia patients and caregivers. Some very frequent needs, such as early diagnosis, are still overlooked, and other needs, such as education/information, are well targeted.
Implications
- The authors call for future studies to evaluate the effects of case management on needs that are overlooked, specifically early diagnosis of dementia, legal issues, and financial issues. Integration of social workers into primary care to assist with financial and legal issues may be an avenue for future studies.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Collaboration and coordination of health and care services for older people with dementia by multidisciplinary health and care providers: a scoping review protocol
- Effectiveness of different post-diagnostic dementia care models delivered by primary care: a systematic review
- Improving Prediction of Dementia in Primary Care
- In This Issue: Confronting Constraints on Individual Behavior & Outcomes