
Article Figures & Data
Figures
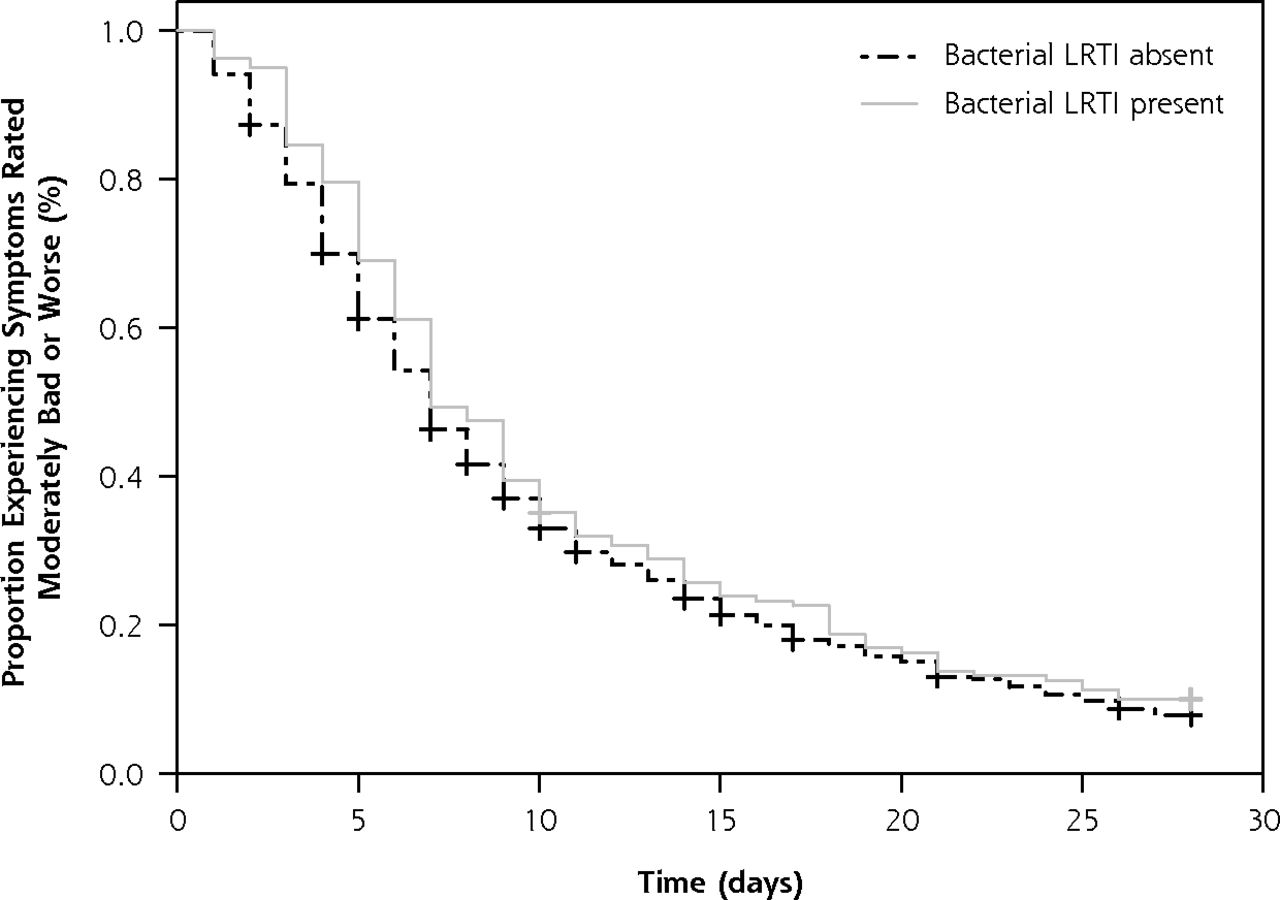
- Figure 1
Kaplan-Meier survival curve for the duration of symptoms rated moderately bad or worse in patients with LRTI.
LRTI = lower respiratory tract infection.
Tables
- Table 1
Baseline Characteristics of Patients With and Without Bacterial Lower Respiratory Tract Infection
Characteristic All Patients (N = 834) Bacterial LRTI Present (n = 162) Bacterial LRTI Absent (n = 672) P Valuea Missing No. (%) Age, mean (SD), y 51 (16) 52 (17) 51 (16) .450 0 (0.0) Male, No. (%) 345 (41) 69 (43) 276 (41) .724 0 (0.0) Current smoker, No. (%) 214 (26) 53 (33) 161 (24) .022 0 (0.0) Comorbidity (pulmonary,b cardiac,c diabetes mellitus), No. (%) 212 (26) 46 (29) 166 (25) .311 1 (0.1) Cough duration before index consultation, mean (SD), d 9 (7) 9 (7) 8 (7) .021 7 (0.8) Severity score (all symptoms), mean (SD)d 31 (14) 34 (14) 30 (14) .003 22 (2.6) Infiltrates on chest radiograph present, No. (%) 26 (3) 9 (6) 17 (3) .046 29 (3.5) Antibiotic use, No. (%)e 62 (7) 20 (12) 42 (6) .008 0 (0.0) COPD = chronic obstructive pulmonary disease; LRTI = lower respiratory tract infection.
↵a P value compared patients with and without bacterial LRTI.
↵b History of COPD, asthma, or other lung disease.
↵c History of heart failure, ischemic heart disease, or other heart disease.
↵d Score for 14 patients’ physician-recorded symptoms summed and scaled to range between 0 and 100 at day 1.
↵e Defined as patient reported intake of antibiotics (1 dose or more) for at least 5 days in the first 10 days after the index physician consultation.
Outcome Bacterial LRTI Present (n = 162) Bacterial LRTI Absent, (n = 672) Crude Analysis No. (95% CI) Adjusted Analysis No. (95% CI)a P Valueb Missing No. (%) Time to resolution of symptoms rated “moderately bad or worse,” median (IQR)d 7 (5–15) 7 (4–13) 0.89 (0.74–1.07)c 0.92 (0.77–1.11)c .375 1 (0.1) Symptom severity score on days 2 to 4 after consultation, mean (SD)d 1.86 (1.07) 1.67 (1.00) 0.19 (0.02–0.37)e 0.21 (0.04–0.38)e .014 3 (0.4) Duration of symptoms until complete resolution, median (IQR)d 15 (10–28) 13 (8–27) 0.88 (0.71–1.10)c 0.92 (0.74–1.15)c .471 1 (0.1) Worsening of illness, No. (%)d 44/162 (27) 114/660 (17) 1.79 (1.20–2.67)f 1.82 (1.21–2.74)f .004 12 (1.4) Duration of interference with normal activities/work, median (IQR)d 6 (1–10) 5 (0–9) 0.91 (0.76–1.09)c 0.91 (0.76–1.09)c .321 6 (0.7) IQR = interquartile range; LRTI = lower respiratory tract infection.
↵a Adjusted for age (for each year increase), current smoking, comorbidity, and cough duration before index consultation.
↵b For adjusted analysis.
↵c Hazard ratio.
d Each symptom was scored by the patient from 0 to 6, with 0 = no problem, 1 = very little problem, 2 = slight problem, 3 = moderately bad, 4 = bad, 5 = very bad, 6 = as bad as it could be.
↵d The great majority of these represent return visits with new or worsening symptoms, and only 2 patients required hospital admission (1 from the bacterial LRTI group and 1 from the nonbacterial LRTI group) within 4 weeks after the first consultation. No study-related deaths were noted.
↵e Difference.
↵F Odds ratio.
The Article in Brief
Disease Course of Lower Respiratory Tract Infection With a Bacterial Cause
Jolien Teepe , and colleagues
Background In cases of acute cough, it is often assumed that bacterial pathogens cause a different illness course than non-bacterial causes, but little is actually known about this. This study compares the illness course of lower respiratory tract infection (LRTI) in primary care patients with and without a bacterial pathogen.
What This Study Found The illness course of lower respiratory tract infection with a bacterial cause is generally mild, uncomplicated and similar to that of nonbacterial lower respiratory tract infection and does not warrant immediate prescribing of antibiotics. Among 834 adults with acute cough, 162 of whom were diagnosed with a bacterial infection, patients with acute bacterial LRTI had only slightly worse symptoms at day two to four after the first office visit and returned more often for a second consultation than those without bacterial LRTI, however, the differences were small and not clinically meaningful. There was no difference in resolution of symptoms rated moderately bad or worse between the groups.
Implications
- The authors conclude that because there appears to be no meaningful difference in the illness course of bacterial LRTIs, physicians can reassure patients that LRTI, even if bacterial, is a self-limiting condition. Rather than immediately prescribing an antibiotic, they recommend following a strategy of watchful waiting.
Supplemental Appendix
Supplemental Appendix: Lab Manual
Files in this Data Supplement:
- Supplemental data: Appendix - Lab Manual pages 1-10
- Supplemental data: Appendix - Lab Manual pages 11-13
- Supplemental data: Appendix - Lab Manual pages 13-34




{kind=link}