
Article Figures & Data
Figures
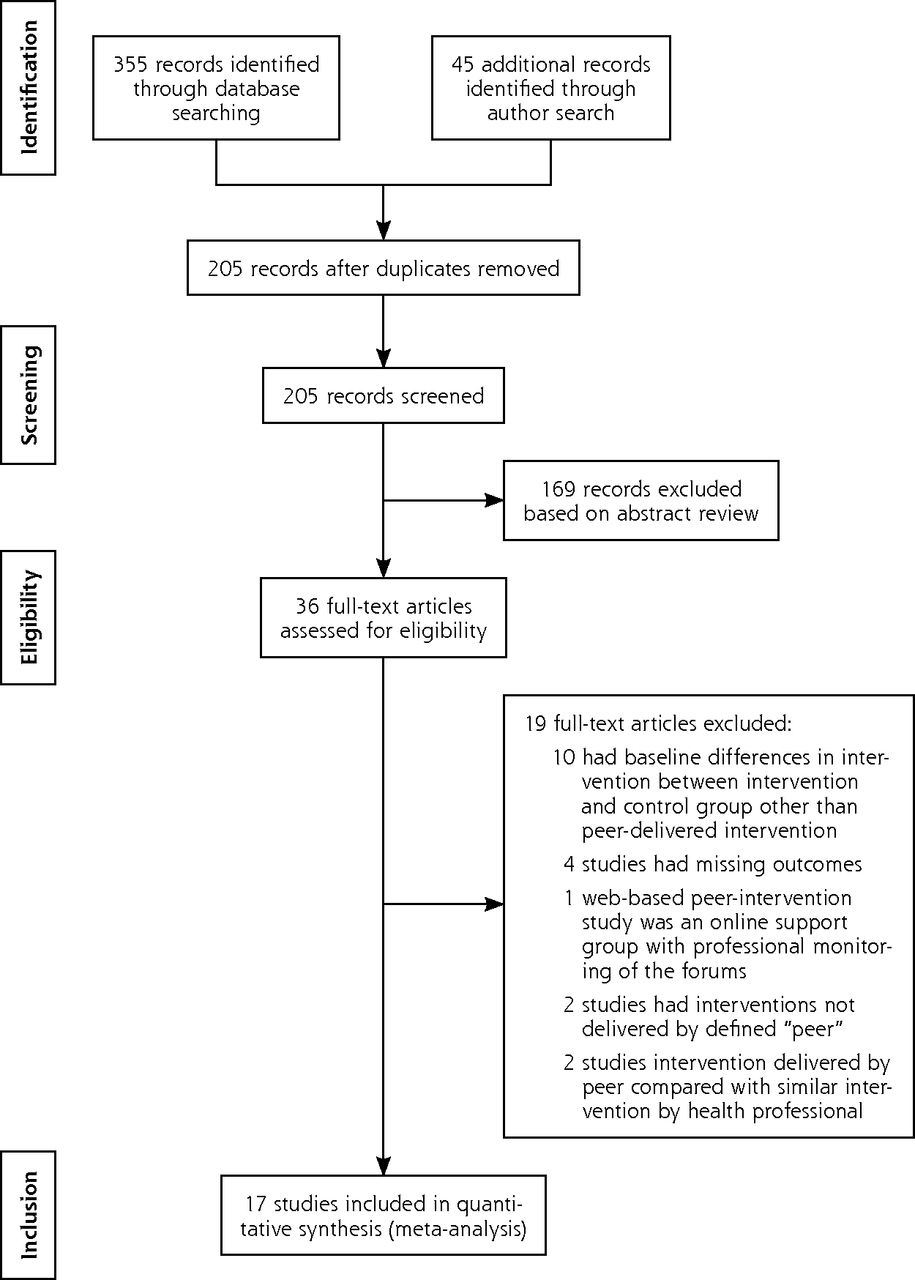
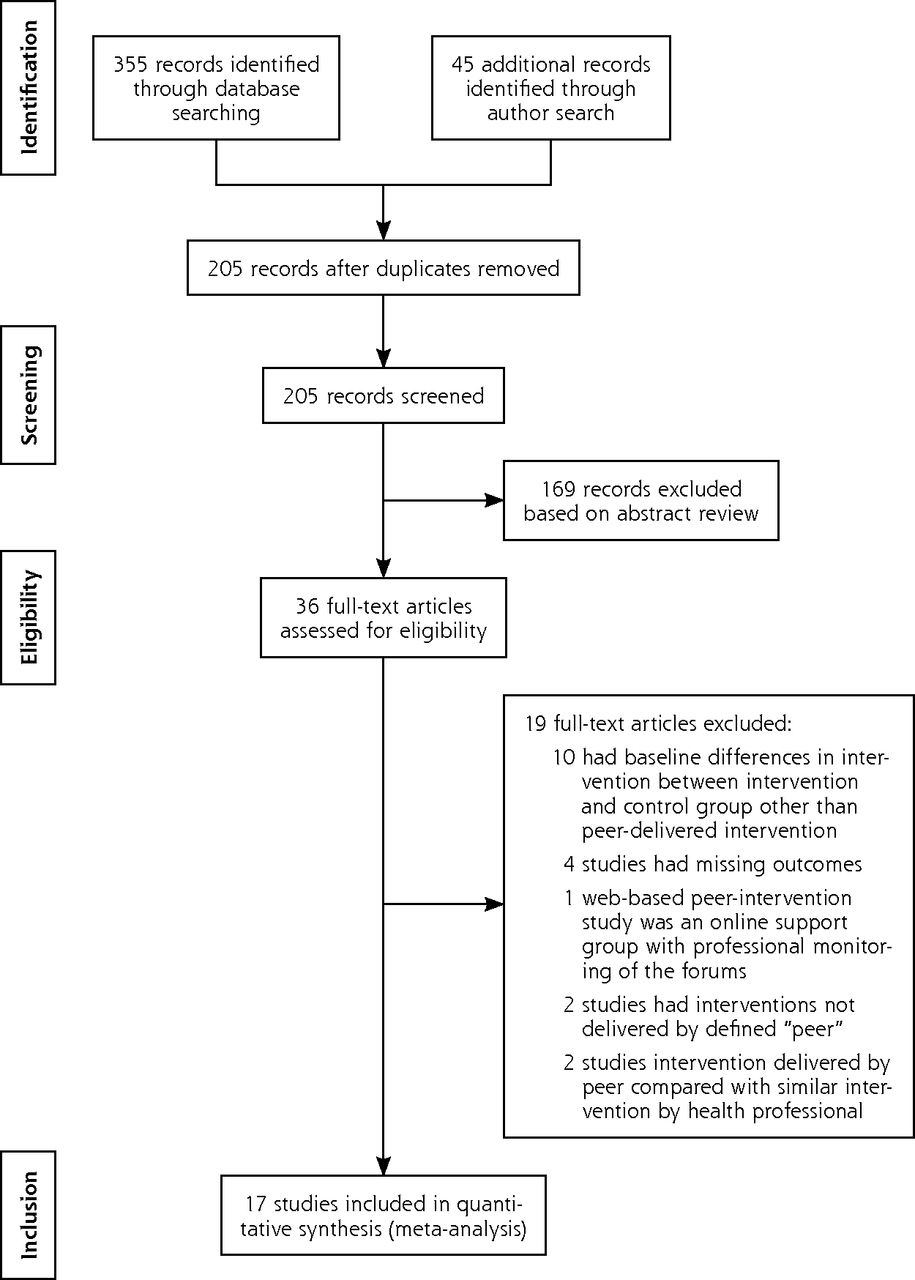
- Figure 1
Results of the literature search.
Note: Performed according to methods outlined by Moher et al.20
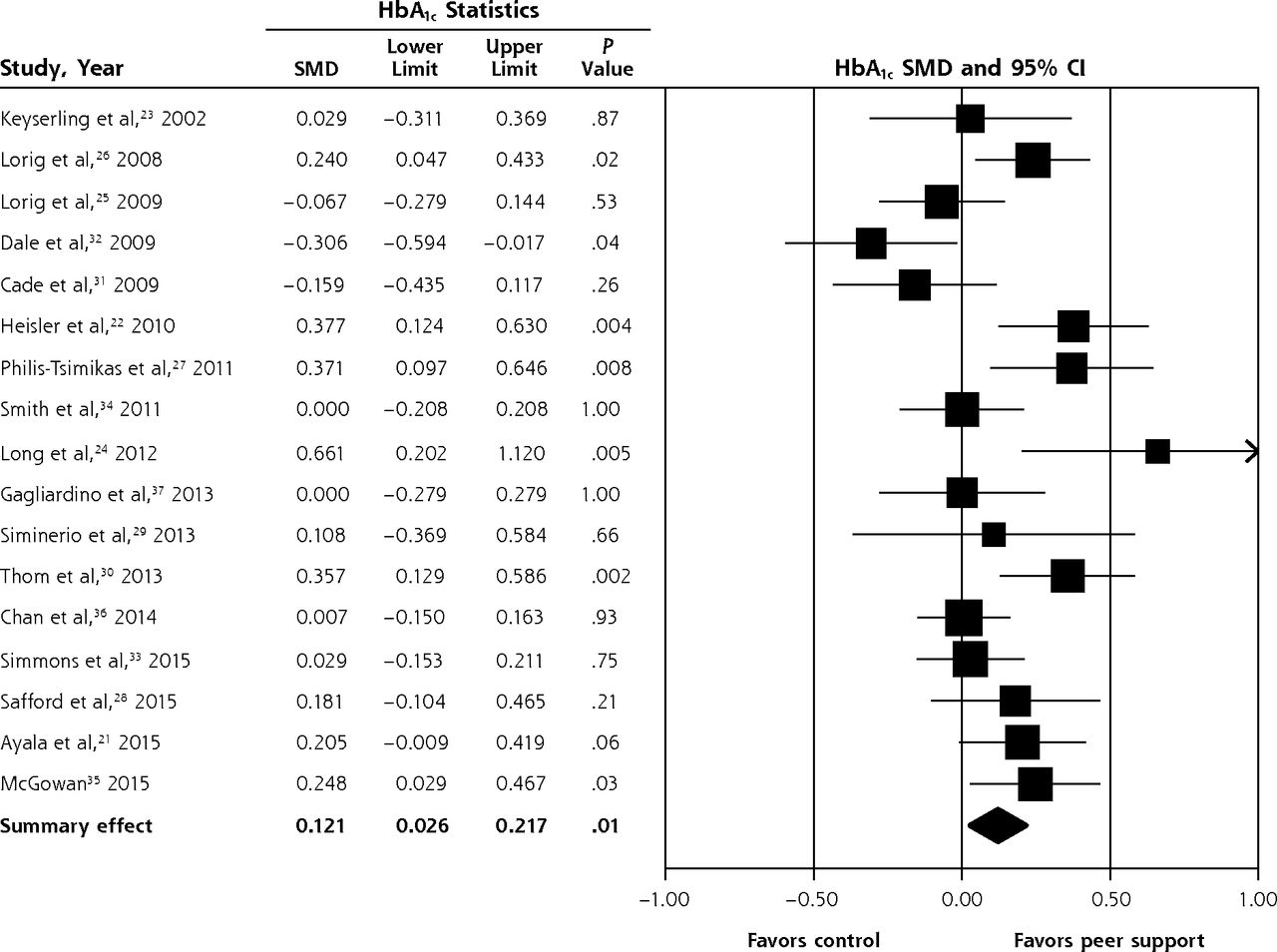
- Figure 2
Effect of peer support interventions on hemoglobin A1c levels.
HbA1c = hemoglobin A1c; SMD = standardized mean difference.
Notes: Random effects model. I2 = 60.66%; P for heterogeneity = .001.
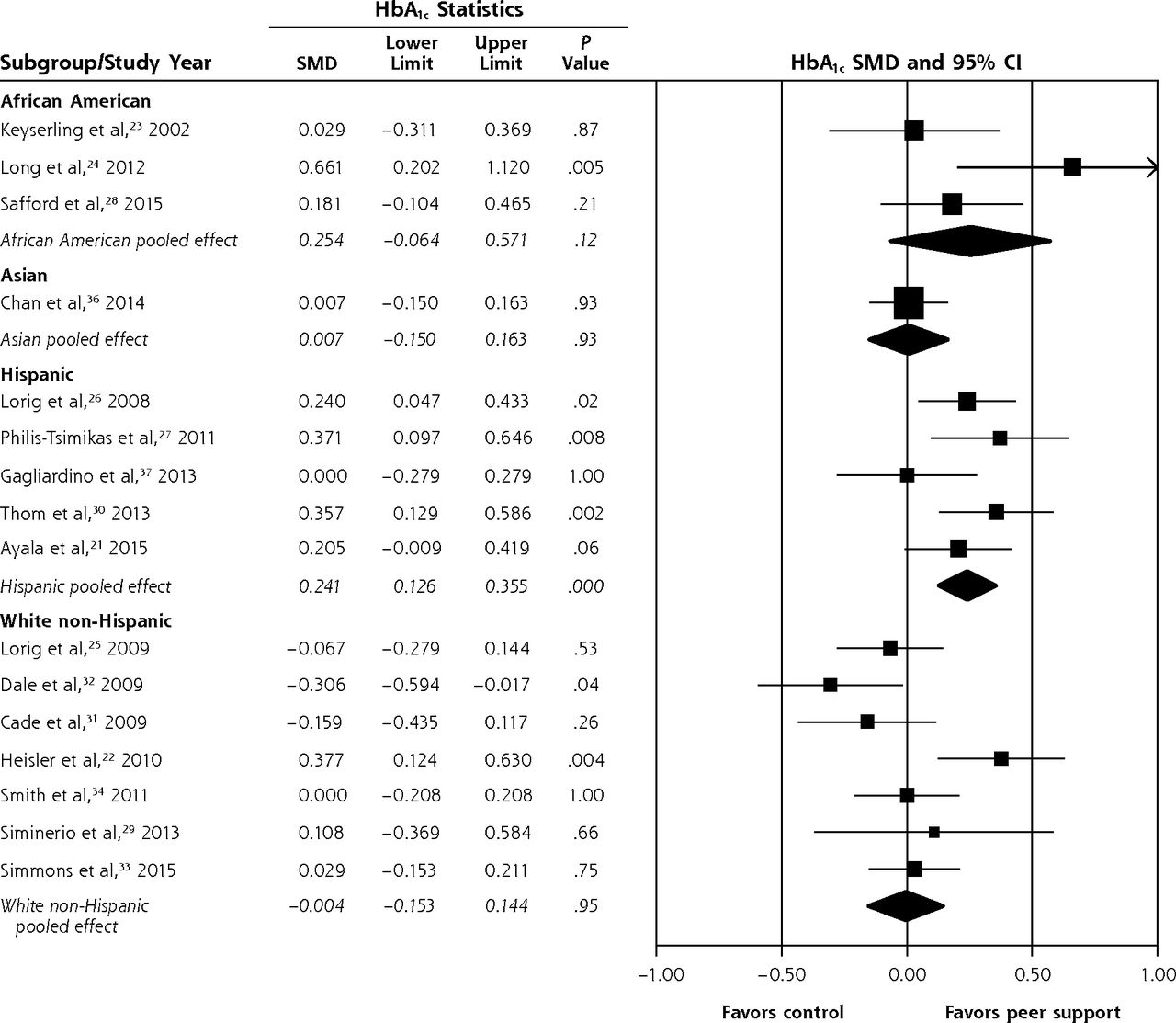
- Figure 3
Subgroup analysis of the effect of peer support interventions on hemoglobin A1c levels in studies by predominant race/ethnicity of the participants.
HbA1c = hemoglobin A1c; SMD = standardized mean difference.
Notes: African American subgroup: I2 = 58.60%, P for heterogeneity = .08. Asian subgroup: I2 = 0.00%. Hispanic subgroup: I2 = 17.12%, P for heterogeneity = .30. White non-Hispanic subgroup: I2 = 59.41%, P for heterogeneity = .02.
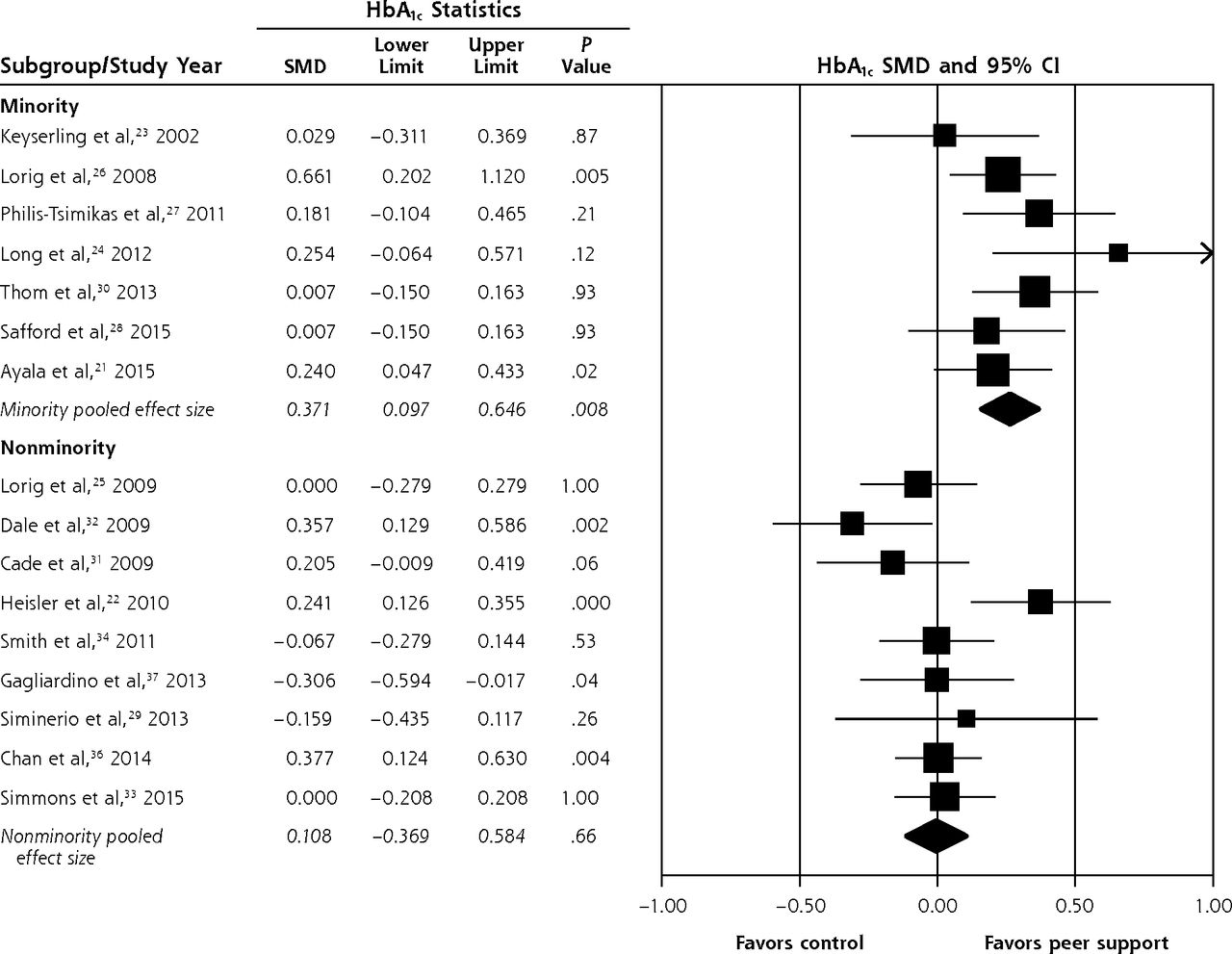
- Figure 4
Subgroup analysis of the effect of peer support interventions on hemoglobin A1c levels in studies by predominant minority status of the participants.
HbA1c = hemoglobin A1c; SMD = standardized mean difference.
Notes: Minority subgroup: I2 = 9.24%, P for heterogeneity = .35. Nonminority subgroup: I2 = 45.90%, P for heterogeneity = .06.


Tables
Study, Year Patients, No. Setting, Population Intervention Control Duration of Peer Training Peer Supervision Attendance Rates, Intensity Keyserling et al,23 2002 133 United States: African American women
Mean HbA1c 11.1%Same as control; also 3 group sessions and monthly telephone calls from a peer counselor for 12 mo
7 peer counselors for 67 patientsIndividual counseling visits with nutritionist at mo 1, 2, 3, and 4 16 h None reported 81% of participants attended at least 1 peer counselor session, 30% attended 2 sessions, and 19% attended 3 sessions
Average phone calls per participant: 9.7Lorig et al,26 2008 417 United States: Spanish-speaking patients
Mean HbA1c 7.41%6-wk program:
2.5 h weekly led by 2 peer leaders
2 peers per 10–15 patientsUsual care 24 h Random observations Not reported Lorig et al,25 2009 345 United States: white, non-Hispanic patients 67%
Mean HbA1C 6.72%6-wk program:
2.5 h weekly led by 2 peer leaders
2 peers per 10–15 patientsUsual care 24 h Random observations Mean attendance of 4.9 of 6 sessions Dale et al,32 2009 187 United Kingdom: white, non-Hispanic patients 96.65%
Mean HbA1c 8.55%Peer supporter called participants after change in their diabetes care at days 7–10, 14–18, 28–35, 56–70, 120–150
1 peer called median of 10 patientsUsual care 2-d training program developed for the study None reported Mean number of calls each patient received: 4.5 (range = 1–6 calls; SD, 2.2) Cade et al,31 2009 207 United Kingdom: white, European-origin patients 95%
Mean HbA1C 7.4%Peer educators delivered 2-h education sessions per week for 7 wk
5 peer educators for 86 participantsUsual care Residential training course provided by the Expert Patients Programme of the National Health Service None reported Of 110 participants in intervention group, 18 attended only 1 session and 22 attended all 7 sessions
63 participants attended final diabetes-specific sessionHeisler et al,22 2010 244 United States: Male veterans, white non-Hispanic 82%
Mean HbA1c 7.97%Peer partners encouraged to call weekly
Three optional 1.5-h face-to-face sessions at 1, 3, and 6 moUsual care Initial 1.5-h training in peer communication skills Interactive voice response–facilitated telephone platform recorded call initiation, frequency, and duration 90% of peer pairs had at least 1 conversation; average number of calls per pair per month was 2.4, 1.7, 1.4, 1.0, 0.9, 0.8 for 6 consecutive mo Philis-Tsimikas et al,27 t2011 207 United States: Mexican Americans
Mean HbA1c 10.4%Weekly 2.5-h education sessions by peer educators for 8 wk Usual care 40 h of training, plus trainees cotaught 2 series of classes with their trainer and taught 2 series on their own, under observation by the trainer Classes were audio-recorded and reviewed using checklists Not reported Smith et al,34 2011 388 Republic of Ireland: Cluster randomized
50% population low income
Ireland general demographics 94.3% white non-Hispanic
Mean HbA1c 7.2%9 peer supporter–facilitated sessions over 2 y; at mo 1, at mo 2, and every 3 mo thereafter Usual care Two 3-h evening training sessions conducted by research teams Meetings were recorded Participants attended mean of 5 peer support meetings; 18% never attended a meeting Long et al,24 2012 77 United States: African American veterans
Mean HbA1c 9.85%Weekly telephone calls by peer mentors; 34 mentors and 39 participants Usual care Single 1-h one-on-one training session No supervision First month, average of 4 calls/mo; by 6 mo, average of 2 calls/mo Gagliardino et al,37 2013 198 Argentina: Hispanic, nonminority in country of residence
Mean HbA1c 7.2%4 weekly peer educator sessions of 90–120 min initially; 1 at 6 mo followed by weekly calls for 6 mo then biweekly calls for 3 mo
Additional face-to-face visits among peers and their supportees were scheduled every second month if specific issues warranted4 weekly sessions of 90–120 min initially; 1 at 6 mo by educators 3-d intensive, structured, small group interactive course Diabetes knowledge of participants tested with multiple-choice questionnaire Not reported Siminerio et al,29 2013 68 United States: white non-Hispanic ethnicity >80%
Mean HbA1c 8.65%Same as control followed by monthly peer calls for 6 mo for diabetes self-management support 6 wk of CDE diabetes self-management education intervention 1-d peer training workshop for CDE with companion workbook-CDE then trained peers in 2-3–h small sessions Contact logs for communications; goal selections were tracked Average of 5.03 calls per participant by peer supporter lasting approximately 25–30 min Thom et al,30 2013 299 United States: Hispanic 46.65%, African American 31.25%; coded as predominantly Hispanic
Mean HbA1c 9.95%Telephone contacts with peers at least twice a month and 2 or more in-person contacts in 6 mo
Coaches worked with median of 7 patientsUsual care 36 h of training over 8 wk in either English or Spanish Not reported Median of 5 (range = 0–29) interactions with the peer health coach
123 patients (83%) had at least 1 interaction; most interactions (76.6%) were by telephone, and the remainder were in personChan et al,36 2014 628 China: Chinese speaking 100%
Mean HbA1c 8.2%Same as control and peer supporter telephone calls: biweekly for 3 mo, then monthly for 3 mo, and then 1 call every other month for 6 mo; anticipated 15 min per call Comprehensive assessment, personalized report, 2-h nurse-led empowerment class, follow-up primary care visit with repeated laboratory assessment and mailing of follow-up reports Four 8-h training sessions Peer supporter completed and mailed checklists to document discussion items, duration of each call, and relevant remarks every 3 mo Median of 20 calls per patient Simmons et al,33 2015 644 England: Cluster randomized factorial design; white, non-Hispanic >90%
Mean HbA1c 7.3%Peer-led group education sessions once a month for at least 5 mo and telephone/e-mail for 1:1 counseling Usual care Main training 14 h plus 3.5 h diabetes education session Not reported 61.5% participants attended at least 1 education session; most participants had telephone or e-mail contacts with peers
Mean number of group attendances: 3.7Safford et al,28 2015 424 United States: cluster randomized trial; African American >90%
Mean HbA1c 7.9%Same as control and initial 45–60–min in-person or telephone get-to-know session with peer supporter followed by weekly calls for 2 mo followed by monthly calls for 8 mo 1 h of group diabetes education class, 5-min counseling session, and diabetes report card 12 h over 2 d Contacts documented on forms and random contacts with intervention participants Mean number of contacts: 13.3 (SD, 8.1) 8.3% of participants had no contacts Ayala et al,21 2015 336 United States: predominantly Hispanic
Mean HbA1c 8.7%8 telephone or in-person contacts with peer supporter in first 6 mo, then as needed contacts in the last 6 mo; 92% of participants had telephone contacts
5–8 patients per peer leaderUsual care 40–50 h Contact logs maintained and tracked by peer leader coordinator Median number of contacts per participant: 4 (range = 1–24) 7% received no intervention McGowan,35 2015 361 Canada: race/ethnicity not given
Mean HbA1c 7.19%Two participant groups received 2 varied types of peer-led self-management programs with varying components: weekly meetings for 6 wk Usual care 24 h Session attendance was logged Mean attendance for intervention group: 5 sessions CDE = certified diabetes educator; HbA1c = hemoglobin A1c.
Study, Year Adequate Sequence Generation Allocation Concealment Blinding of Investigators and/or Outcome Assessors Complete Outcome Data Keyserling et al,23 2002 Yes Yes No Yes Lorig et al,26 2008 Yes Yesa No Yes Lorig et al,25 2009 Yes Yesa No Yes Dale et al,32 2009 Yes Yes No Yes Cade et al,31 2009 Yesb Noc Noc Yes Heisler et al,22 2010 Yes Yes Yes Yes Philis-Tsimikas et al,27 2011 Yes Yesa Noa Yes Smith et al,34 2011 Yes Yes No Yes Long et al,24 2012 Yes Yes Yes Yes Gagliardino et al,37 2013 Yesa Noc Noc Noc Siminerio et al,29 2013 Yes Noa No Yes Thom et al,30 2013 Yes Yes Noa Yes Chan et al,36 2014 Yes Yes Noc Yes Simmons et al,33 2015 Yes Yes Yes Yes Safford et al,28 2015 Yes Yes No Yes Ayala et al,21 2015 Yes Noc Noc Yes McGowan,35 2015 Yes Yes No Yes Notes: Yes indicates low risk of bias; No indicates high risk of bias. Selective outcome reporting risk was considered minimal as we selected only studies that reported hemoglobin A1c level as the outcome. No other major biases were noted in the included studies. None of the trials blinded participants.
↵a Author response to information requests.
↵b Likely low risk of bias but no details on sequence generation available from article and author.
↵c Not reported or no response from author.
The Article in Brief
Peer Support Interventions for Adults With Diabetes: A Meta-Analysis of Hemoglobin A1C Outcomes
Sonal J. Patil , and colleagues
Background Peer support is a promising approach to improving and sustaining diabetes self-management. This study analyzes existing research to assess the effectiveness of peer-support interventions on improving glycemic control in adult patients with diabetes as measured by HbA1C, compared to patients who received similar care except for peer delivered interventions.
What This Study Found Peer support interventions delivered by people affected by diabetes are associated with a small but statistically significant reduction in glycosylated hemoglobin, with larger effects among minority (particularly Hispanic) participants. There was an overall 0.24 percent improvement in HbA1c. Studies with predominantly Hispanic participants showed an HbA1c improvement of 0.48 percent in the peer support intervention group compared with the control group. In contrast, the pooled effect size from studies with predominantly white, non-Hispanic participants showed no improvement in HbA1c level with peer support interventions.
Implications
- Peer health coaches might be providing more culturally appropriate health education in ethnic minority populations, particularly in the Latino population. The authors call for future research to assess the effect of peer interventions on long-term patient-centered outcomes.
Annals Journal Club
Nov/Dec 2016: A Meta-Analysis of Peer-Support Interventions for Adults With Diabetes
The Annals of Family Medicine encourages readers to develop a learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club. RADICAL is an acronym for Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. It also indicates the need to engage diverse participants in thinking critically about, and then acting on, important issues affecting primary care.1
HOW IT WORKS
In each issue, the Annals selects an article and provides discussion tips and questions. We encourage you to post a summary of your journal club's conversation. (Open the article and click on "TRACK Discussion: Submit a comment.") Details are available at http://www.AnnFamMed.org/site/AJC/.
CURRENT SELECTION
Article for Discussion
Patil S, Ruppar T, Koopman RJ, et al. Peer support interventions for adults with diabetes: a meta-analysis of hemoglobin A1C outcomes. Ann Fam Med 2016;14(6):540-551.
Discussion Tips
Systematic reviews and meta-analyses are observational studies that provide an overview of a literature. However, analysis of these types of studies requires additional skills over those needed to analyze randomized controlled trials. This article offers an opportunity to investigate positive and negative aspects of this type of study in assessing the effect of peer support interventions on the narrow but summative outcome of glycosylated hemoglobin.
Discussion Questions
- What is a systematic review? What is a meta-analysis? How are they related? What are their primary weaknesses?
- What was the research question for this review?
- Was the scope of the question appropriate (too broad or narrow)? How adequate was the search?
- What kind of important studies might have been missed due to scope or search criteria?
- What is PRISMA?2 What are the benefits and downsides of following this reporting structure?
- What is heterogeneity and why is it an important concept in systematic reviews and
meta-analysis?
- How is heterogeneity measured in this study?
- What is publication bias? Why is this an important concept in systematic reviews and
meta-analyses?
- How is this investigated in the study?
- What is a standard mean difference? Why was this the primarily reported outcome?
- What are the main findings? Was an important level of heterogeneity identified, and how does that affect your interpretation of the findings?
- How did the results change when investigated by different subgroups?
- What is an ecological fallacy? How might individual patient data (instead of trial level) have strengthened the study findings?
- What are the strengths and weaknesses of hemoglobin A1C as an outcome measure?3 Why do you think the authors investigated hemoglobin A1C?
- Were the decreases in hemoglobin A1C "clinically meaningful"? Were they durable? How long was the follow-up of the included studies?
- Are the patients in the primary studies comparable to patients in your practice?
- Will this article change your practice? If so, how?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals Journal Club: It's time to get RADICAL. Ann Fam Med. 2006;4(3):196-197 http://annfammed.org/content/4/3/196.full.
- Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700.
- Yudkin John S, Lipska Kasia J, Montori Victor M. The idolatry of the surrogate. BMJ. 2011;343:d7995.
Supplemental Appendixes
Files in this Data Supplement:
- Supplemental data: Appendixes - PDF file
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Investigating the sustainability of self-help programmes in the context of leprosy and the work of leprosy missions in Nigeria, Nepal and India: a qualitative study protocol
- Here for You: A Review of Social Support Research in Young Adults With Diabetes
- Peer Coaching to Improve Diabetes Self-Management Among Low-Income Black Veteran Men: A Mixed Methods Assessment of Enrollment and Engagement
- Lifestyle interventions for type 2 diabetes management among migrants and ethnic minorities living in industrialized countries: a systematic review and meta-analyses
- Task Sharing Chronic Disease Self-Management Training With Lay Health Coaches to Reduce Health Disparities
- Ontario Brain Injury Association Peer Support Program: a mixed methods protocol for a pilot randomised controlled trial
- Supported self-management for people with type 2 diabetes: a meta-review of quantitative systematic reviews
- Aspects of Multicomponent Integrated Care Promote Sustained Improvement in Surrogate Clinical Outcomes: A Systematic Review and Meta-analysis
- In This Issue: Social Context; Disease Causes
- A Meta-Analysis of Peer-Support Interventions for Adults With Diabetes