
Abstract
PURPOSE Care coordination has been identified as a key strategy in improving the effectiveness, safety, and efficiency of the US health care system. Our objective was to determine whether population or health care system issues are associated with primary care coordination gaps in the United States and other high-income countries.
METHODS We analyzed data from the 2013 Commonwealth Fund International Health Policy (IHP) survey with multivariate logistic regression analysis. Respondents were adult primary care patients from 11 countries: Australia, Canada, France, Germany, the Netherlands, New Zealand, Norway, Sweden, Switzerland, United Kingdom, and the United States. Poor primary care coordination was defined as participants reporting at least 3 gaps in the coordination of care out of a maximum of 5.
RESULTS Analyses were based on 13,958 respondents. The rate of poor primary care coordination was 5.2% (724/13,958 respondents) overall and highest in the United States, at 9.8% (137/1,395 respondents). Multivariate regression analysis among all respondents found that they were less likely to experience poor primary care coordination if their primary care physician often or always knew their medical history, spent sufficient time, involved them, and explained things well (odds ratio = 0.6 for each). Poor primary care coordination was more likely to occur among patients with chronic conditions (odds ratios = 1.4–2.1 depending on number) and patients younger than 65 years (odds ratios = 1.6–2.3 depending on age-group). Among US respondents, insurance status, health status, household income, and sex were not associated with poor primary care coordination.
CONCLUSIONS The United States had the highest rate of poor primary care coordination among the 11 high-income countries evaluated. An established relationship with a primary care physician was significantly associated with better care coordination, whereas being chronically ill or younger was associated with poorer care coordination.
- primary health care
- coordination of care
- patient experience
- surveys and questionnaires
- international
- continuity of patient care
INTRODUCTION
Coordination of care has been identified by the Institute of Medicine as a key strategy in improving the effectiveness, safety, and efficiency of the US health care system.1 Care coordination in primary care involves deliberately organizing patient care activities and sharing information among all of the participants concerned to achieve safer and more effective care.2 Effective primary care coordination programs have been shown to reduce hospitalizations,3 but require patients to have frequent contact with health care professionals and to anticipate needs and communicate information to the right people at the right time.2 Implementing such programs has become increasingly difficult in many countries because of multiple factors that include a shortage of primary care physicians (PCPs), health professional workloads, underfunding of primary care by governments, fragmentation between sectors of health care, and the burden of disease and risk profile of the population.4–6
A continuous relationship between a patient and his or her physician has often been encouraged to enhance care coordination.7,8 Optimizing this relationship has been shown to increase patient satisfaction and medication adherence, and reduce hospitalizations.7,8 Despite these benefits, data measuring the effect of patients’ relationship with their PCP on care coordination are sparse. International comparisons are also useful to identify if challenges experienced in the United States are due to its unique patient population or health care system.
The Commonwealth Fund is a private foundation dedicated to promoting a health care system that achieves better access, improved quality, and greater efficiency.9 As part of its mission, the Fund has been conducting an International Health Policy (IHP) survey in multiple countries for more than a decade. In 2013, this survey focused on adults from 11 countries: Australia, Canada, France, Germany, the Netherlands, New Zealand, Norway, Sweden, Switzerland, United Kingdom, and the United States.10 We aimed to use the 2013 Commonwealth Fund IHP survey data to determine how adult patients perceive care coordination and to identify risk factors associated with primary care coordination gaps, comparing the United States and other high-income countries.
METHODS
This study was considered exempt by the University of Cincinnati Institutional Review Board (2015–5769). A detailed methodology of the IHP survey has been published previously.11,12
Outcome Measure and Factors
Primary care coordination was assessed with 5 questions in the IHP survey. Three questions focused on respondents’ experience in the last 2 years and asked whether there was ever a time when (1) test results or medical records were not available, (2) they received conflicting information, and (3) their doctors ordered a medical test that they felt was unnecessary.11 The remaining 2 questions focused on respondents’ experience with their specialist in the last 2 years. These questions asked whether there was ever a time when (1) their specialist did not have basic medical information or test results from their regular doctor and (2) after they saw their specialist, their regular doctor did not seem informed and up to date about the care received from the specialist.11 Responses were coded “no” to these last 2 questions if respondents had not visited a specialist in the last 2 years. Respondents answering “yes” to any of these 5 components were considered to have a gap in care coordination. Respondents were considered to have poor primary care coordination if they had at least 3 gaps out of the 5 possible gaps. Similar questions have also been used in previously validated surveys on care coordination.13–15
Data Analysis
To validate the clinical relevance of the poor primary care coordination composite score used in this study, we used logistic regression analysis to correlate the score’s association with hospitalizations and emergency department visits in the last 2 years. Emergency department visits were self-reported as either urgent or nonurgent, where nonurgent issues could have been treated where they usually get their medical care.
Each care coordination gap and poor primary care coordination were assessed for their associations with the risk factors using a multivariate logistic regression model. All of these models were further adjusted by sampling weights to account for distributions of the populations and reach unbiased estimates of the parameters. The sampling weights were decided based on each country’s age, sex, region, and education. Weights were also factored by race and ethnicity in the United States (these data were not available for other countries). Finally, all statistical analyses were computed using SAS 9.4 software (SAS Institute) and P values <.05 were considered statistically significant.
RESULTS
A total of 16,383 adults provided responses in the 2013 IHP survey, translating to a 23% response rate. In total, 13,958 (85%) of these respondents completed the primary care coordination questions and were included in our analyses. Respondents’ socioeconomic demographics and health-related characteristics are summarized in Table 1.
Distribution of Respondents by Country, Socioeconomic Demographics, and Health-Related Characteristicsa
Care Coordination Gaps
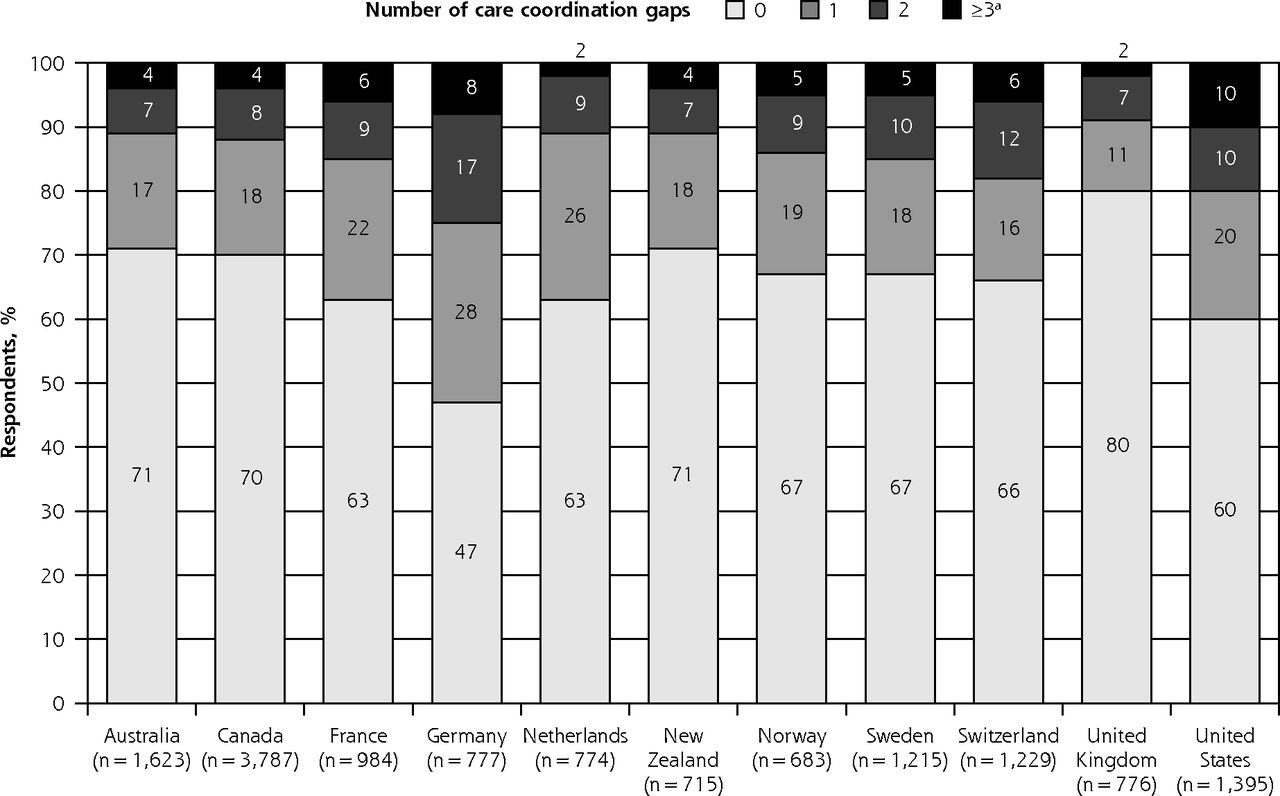
Overall, 33% of respondents experienced at least 1 care coordination gap, and 5% experienced poor primary care coordination (3 or more gaps). The United States had the largest percentage of respondents with poor primary care coordination (9.8%) among the 11 high-income countries studied (Figure 1).

Percentage of respondents with care coordination gaps by country.
aPoor primary care coordination was defined as having at least 3 gaps out of a possible 5.
Regression models showed the clinical relevance of poor primary care coordination as those affected had a greater likelihood of being hospitalized (odds ratio [OR] = 3.4; 95% CI, 3.0–4.0) and having to visit the emergency department for nonurgent care (OR = 2.7; 95% CI, 2.3–3.2) and urgent care (OR = 2.0; 95% CI, 1.7–2.3) compared with those who did not experience poor primary care coordination (Supplemental Appendix, available at http://www.AnnFamMed.org/content/15/2/113/suppl/DC1/). This result supported the construct validity of the definition of poor primary care coordination that we used.
Factors Associated With Gaps
The multivariate logistic regression models for each care coordination component comparing each country with the United States are presented in Table 2. Respondents from the United States were significantly more likely to report a gap in each of the components than those from the other high-income countries. Respondents who reported positive, established interactions with their PCP were less likely to report poor primary care coordination. This association is shown where respondents with a primary care physician who often or always knew their medical history, spent sufficient time, involved them, and explained things well were less likely to report poor primary care coordination (OR = 0.6 for each, 95% CIs ranged from 0.5 to 0.8 for all items). Additionally, respondents younger than 65 years had higher odds of having poor care coordination compared with those aged 65 years and older even when accounting for the number of physicians they saw and medical conditions they had. Respondents aged 25 to 34 years had the highest odds ratio of having poor care coordination (OR = 2.3; 95% CI, 1.7–3.0) Additional multivariate logistic regression analysis for US respondents also showed that insurance status, health status, household income, and sex were not associated with having poor primary care coordination.
Odds Ratios for Poor Primary Care Coordination and Individual Care Coordination Gapsa
The multivariate logistic regression models for each care coordination component showed that respondents who reported positive, established interactions with their PCP were less likely to report poor primary care coordination (Table 2). As such, those reporting that their PCP often or always knew their medical history, spent sufficient time with them, involved them in decision about their care, and explained things well had significantly lower odds of having a gap in each of the 5 care coordination components (OR ranged from 0.6 to 0.8 for each, 95% CI ranged from 0.5 to 0.9 for all items). Additionally, respondents with chronic medical conditions and respondents aged 25 to 34 years, compared with those aged 65 years and older, were more likely to have a gap in each of the 5 care coordination questions.
DISCUSSION
Key Findings
In the 11 countries collectively, one-third of respondents experienced at least 1 gap in the coordination of care, and 5% experienced sufficient gaps to constitute poor primary care coordination. US respondents had the highest rate of poor primary care coordination at 9.8%. Care coordination gaps have been associated with a higher risk of patients experiencing a medical error, more follow-up appointments, and unnecessary health care spending.16–21 The high rate of poor primary care coordination in the United States may also imply that US patients are receiving lower-quality care compared with peers in other high-income countries. This finding further fuels the debate that the United States does not rate highly on a global basis, with its health care system ranked 37th22 and its adult mortality ranked 43rd.23
In the United States, care coordination appeared to be independent of patient characteristics such as insurance status, health status, household income, and sex. This finding highlights that US patients of various insurance statuses and income levels reported similar levels of poor primary care coordination, implying that a systemic issue in the US health care system is responsible for poor primary care coordination. It has been reported that 3 out of 4 adults in the United States believe the health system needs fundamental change or complete rebuilding.10,24 The systemic issue may be associated with the fact that a referral to a specialist is not needed.25 A similar scenario also exists in France, Germany, and Switzerland.25 As such, more than 5% of patients from all these countries reported having poor primary care coordination. Conversely, in the remaining countries, where it is not possible to visit a specialist without a referral from a PCP,25 less than 5% of respondents report having poor primary care coordination. This gatekeeping role by PCPs thus appears to improve care coordination as health care systems become increasingly fragmented.
Our study also shows that older patients generally experienced better care coordination than their younger counterparts in the United States and other high-income countries, even after adjusting for their insurance status. A similar trend has been observed in Spain,26 which was not included in this study, and may be due to older patients being more familiar with the health care system.27 It has also been suggested, however, that the current health care system is generally not designed to accommodate the needs of young adults with chronic conditions, particularly as more children with disabilities are surviving into adulthood.28,29 As these trends continue to grow, care coordination programs should ensure they are designed for a younger, chronically ill population.
This study is the first to quantify the association of the patient-physician relationship on care coordination throughout numerous high-income countries. The patient-centered medical home (PCMH) model was recently financially incentivized in the United States to enhance the physician care experiences that focus on whole-person orientation and foster a personalized relationship with their patients.30 Although the number of primary care practices that have achieved PCMH recognition has steadily increased to include more than 34,000 physicians and more than 6,700 sites in 2013,31 these numbers represents only about 15% of all PCPs in the United States.32 Preliminary reports, however, have shown PCMHs to positively influence patient outcomes by decreasing hospitalizations and emergency department visits.33 Furthermore, having a PCMH has also been shown to improve patients’ experiences with their PCP in multiple countries outside the United States.34–36 This positive impact of PCMHs and results from our study further highlight the importance of the patient-physician relationship in optimal care coordination programs.
Limitations
The generalizability of this study is limited by its 23% response rate. This response rate, however, is similar to that of other large international surveys.10 The response rates for each country were as follows: Australia, 30%; Canada, 24%; France, 32%; Germany, 11%; the Netherlands, 23%; New Zealand, 30%; Norway, 11%; Sweden, 29%; Switzerland, 33%; the United Kingdom, 20%; and the United States, 22%. As response rates were particularly low in Germany and Norway, potential bias could have been introduced. Additional effort was conducted to weigh each response to enhance the generalizability of the data. This post hoc adjustment, however, cannot completely eliminate nonresponse bias from our study.
Last, additional country-specific data were not available for the analysis to identify why some countries had better care coordination than others. This missing information included the supply of PCPs in each country and where the care was received (eg, in large comprehensive clinics, in clinician offices).
Conclusions
One-third of all respondents experienced at least 1 coordination gap in primary care, but the percentage with poor primary care coordination was low. Respondents from the United States had the highest rate of poor primary care coordination. Having an established relationship with a PCP was significantly associated with better care coordination. Furthermore, patients in the United States with poor primary care coordination appeared to be chronically ill, younger individuals. These differences transcended insurance status and household income, suggesting a systemic issue in the US health care system that distinguishes its efficacy of primary care coordination from that of other countries. Additionally, these results suggest that increased efforts to support relationships between patients and their PCPs are required and that new programs should be designed for a younger, chronically ill population to enhance care coordination.
Acknowledgments
The authors thank The Commonwealth Fund for granting access to the data.
Footnotes
Conflicts of interest: authors report none.
Supplementary materials: Available at http://www.AnnFamMed.org/content/15/2/113/suppl/DC1/
- Received for publication March 10, 2016.
- Revision received September 27, 2016.
- Accepted for publication October 16, 2016.
- © 2017 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- The impact of remote care approaches on continuity in primary care: a mixed-studies systematic review
- The impact of remote care approaches on continuity in primary care: a mixed-studies systematic review
- Barriers to implementation of enhanced recovery after surgery (ERAS) by a multidisciplinary team in China: a multicentre qualitative study
- Protocol for an implementation and realist evaluation of a new organisational model for primary care practices in the canton of Vaud, Switzerland
- Transforming concepts in patient safety: a progress report
- The influence of patient-clinician ethnocultural and language concordance on continuity and quality of care: a cross-sectional analysis
- In This Issue: On-the-Ground Advances & High-Level Influences