
Article Figures & Data
Figures
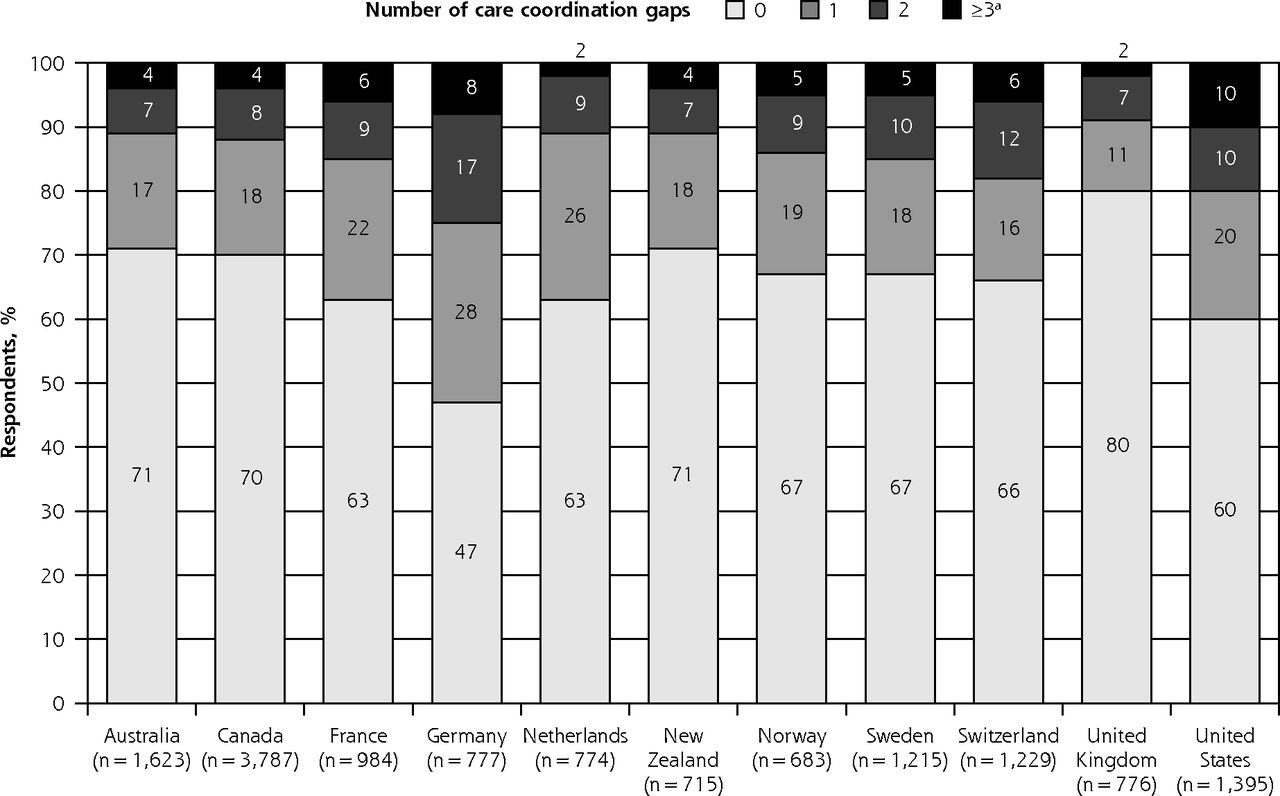
- Figure 1
Percentage of respondents with care coordination gaps by country.
aPoor primary care coordination was defined as having at least 3 gaps out of a possible 5.

Tables
- Table 1
Distribution of Respondents by Country, Socioeconomic Demographics, and Health-Related Characteristicsa
Characteristic All Respondents, No. (%) (N = 13,958) Respondents With Poor Primary Care Coordination, No. (%)b All Countries (n = 724) United States (n = 137) Country Australia 1,623 (11.6) 68 (9.4) NA Canada 3,787 (27.1) 174 (24.0) NA France 984 (7.0) 61 (8.4) NA Germany 777 (5.6) 60 (8.3) NA Netherlands 774 (5.5) 18 (2.5) NA New Zealand 715 (5.1) 27 (3.7) NA Norway 683 (4.9) 33 (4.6) NA Sweden 1,215 (8.7) 57 (7.9) NA Switzerland 1,229 (8.8) 71 (9.8) NA United Kingdom 776 (5.6) 18 (2.5) NA United States 1,395 (10.0) 137 (18.9) 137 (100.0) Age-group, y 18–24 1,123 (8.0) 48 (6.6) 7 (5.1) 25–34 1,735 (12.4) 84 (11.6) 19 (13.9) 35–49 3,339 (23.9) 202 (27.9) 33 (24.1) 50–64 4,107 (29.4) 231 (31.9) 45 (32.8) ≥65 3,654 (26.2) 159 (22.0) 33 (24.1) Regular doctor often/always: Knows your medical history 11,332 (81.2) 488 (67.4) 93 (67.9) Spends enough time with you 11,338 (81.2) 473 (65.3) 83 (60.6) Involves you as much as you want 11,355 (81.4) 494 (68.2) 91 (66.4) Explains things well 12,165 (87.2) 511 (70.6) 86 (62.8) Insurance – US respondents only (n = 1,395) (n = 137) No insurance 141 (10.1) 14 (10.2) 14 (10.2) Private 634 (45.4) 57 (41.6) 57 (41.6) Medicare 433 (31.0) 32 (23.4) 32 (23.4) Medicaid 180 (12.9) 34 (24.8) 34 (24.8) Missing 7 (0.5) 0 (0.0) 0 (0.0) NA = not applicable.
↵a Full results are available online (Supplemental Appendix 2, available at http://www.AnnFamMed.org/ content/15/2/113/suppl/DC1/).
↵b Poor primary care coordination was defined as having at least 3 gaps out of a possible 5.
- Table 2
Odds Ratios for Poor Primary Care Coordination and Individual Care Coordination Gapsa
Characteristic Poor Primary Care Coordination, Odds Ratio (95% CI)b Care Coordination Gap, Odds Ratio (95% CI)c Test/Records Not Available Conflicting Information Unnecessary Test Ordered Specialist Not Informed PCP Not Informed Country Australia 0.5 (0.4–0.7)d 0.5 (0.4–0.6)d 0.9 (0.7–1.1) 0.6 (0.5–0.7)d 0.6 (0.5–0.8)d 0.6 (0.5–0.8)d Canada 0.5 (0.4–0.6)d 0.6 (0.5–0.8)d 0.7 (0.6–0.9)d 0.4 (0.3–0.5)d 0.8 (0.6–1.0) 0.9 (0.7–1.1) France 0.6 (0.4–0.8)d 0.6 (0.4–0.7)d 0.7 (0.5–0.8)d 0.8 (0.6–1.0) 0.9 (0.7–1.2) 1.2 (1.0–1.5) Germany 0.5 (0.4–0.8)d 0.4 (0.3–0.5)d 0.9 (0.7–1.2) 1.0 (0.8–1.3) 1.0 (0.8–1.4) 2.6 (2.0–3.3)d Netherlands 0.3 (0.2–0.5)d 0.8 (0.6–1.1) 1.6 (1.2–2.0)d 1.3 (1.0–1.7) 0.4 (0.2–0.5)d 0.3 (0.2–0.4)d New Zealand 0.5 (0.3–0.8)d 0.5 (0.4–0.7)d 1.0 (0.8–1.3) 0.5 (0.3–0.6)d 0.6 (0.4–0.8)d 0.7 (0.5–1.0) Norway 0.5 (0.3–0.7)d 0.3 (0.3–0.5)d 0.9 (0.7–1.2) 0.5 (0.4–0.7)d 0.7 (0.5–1.0) 1.3 (1.0–1.6) Sweden 0.5 (0.3–0.6)d 0.6 (0.5–0.7)d 0.8 (0.6–1.0) 0.2 (0.2–0.3)d 0.8 (0.7–1.1) 1.3 (1.0–1.6) Switzerland 0.8 (0.6–1.1) 0.6 (0.5–0.8)d 0.8 (0.6–1.0) 1.7 (1.3–2.1)d 1.3 (1.0–1.7) 0.9 (0.7–1.1) United Kingdom 0.3 (0.2–0.5)d 0.5 (0.4–0.7)d 0.4 (0.3–0.5)d 0.5 (0.3–0.7)d 0.6 (0.4–1.0) 0.5 (0.3–0.7)d United States Reference Reference Reference Reference Reference Reference Age-group, y 18–24 1.9 (1.4–2.7)d 1.9 (1.5–2.4)d 3.1 (2.5–3.8)d 2.4 (1.8–3.0)d 1.1 (0.8–1.4) 1.3 (1.0–1.5) 25–34 2.3 (1.7–3.0)d 2.2 (1.8–2.8)d 3.0 (2.4–3.6)d 2.0 (1.6–2.5)d 1.3 (1.0–1.6) 1.2 (1.0–1.5) 35–49 2.2 (1.7–2.7)d 2.3 (1.9–2.8)d 2.6 (2.2–3.1)d 1.9 (1.6–2.3)d 1.2 (1.0–1.4) 1.2 (1.1–1.5)d 50–64 1.6 (1.2–2.0)d 1.9 (1.6–2.3)d 1.8 (1.6–2.1)d 1.5 (1.3–1.8)d 1.2 (1.0–1.4) 1.0 (0.9–1.2) ≥65 Reference Reference Reference Reference Reference Reference Regular doctor knows your medical history Often or always 0.6 (0.5–0.7)d 0.7 (0.6–0.8)d 0.7 (0.6–0.8)d 0.6 (0.5–0.7)d 0.8 (0.7–0.9)d 0.8 (0.7–0.9)d Never, rarely, or sometimes Reference Reference Reference Reference Reference Reference Regular doctor spends enough time with you Often or always 0.6 (0.5–0.8)d 0.7 (0.6–0.8)d 0.6 (0.5–0.6)d 0.7 (0.6–0.8)d 0.8 (0.7–0.9)d 0.8 (0.7–0.9)d Never, rarely, or sometimes Reference Reference Reference Reference Reference Reference Regular doctor involves you as much as you want Often or always 0.6 (0.5–0.8)d 0.8 (0.6–0.9)d 0.7 (0.6–0.8)d 0.8 (0.6–0.9)d 0.9 (0.7–1.1) 0.8 (0.7–0.9)d Never, rarely, or sometimes Reference Reference Reference Reference Reference Reference Regular doctor explains things well Often or always 0.6 (0.5–0.7)d 0.7 (0.6–0.9)d 0.8 (0.7–0.9)d 0.6 (0.5–0.7)d 0.8 (0.7–0.9)d 0.8 (0.6–0.9)d Never, rarely, or sometimes Reference Reference Reference Reference Reference Reference PCP = primary care physician.
↵a Parameters included in each model also included sex, household income, health status, number of doctors seen in the last year, and number of medications. Full regression analysis results are available online (Supplemental Appendix 3, available at http://www.AnnFamMed.org/content/15/2/113/suppl/DC1/).
↵b Had at least 3 gaps out of a possible 5.
↵c Gaps in detail: test/records not available at scheduled appointment; conflicting information received for medical care; unnecessary test ordered as it had already been done; specialist not informed by PCP; and PCP not informed by specialist.
↵d P <.05 after adjusting for multiple comparisons using the Bonferroni method.
Supplemental Appendixes 1-3
Supplemental Appendixes 1-3
Files in this Data Supplement:
- Supplemental data: Appendixes 1-3 - PDF file
The Article in Brief
Minding the Gap: Perceived Factors Associated With Primary Care Coordination of Adults in 11 Countries
Jonathan Penm , and colleagues
Background Care coordination (organizing patient care activities and sharing information among participants) is a key strategy for improving the effectiveness, safety and efficiency of health care systems. This study examines care coordination in 11 high-income countries.
What This Study Found One out of every three respondents experienced at least one coordination gap in primary care, but the overall percentage reporting poor primary care coordination was low. Among the 11 countries evaluated, the United States had the highest rate of poor primary care coordination. Among patients in Australia, Canada, France, Germany, the Netherlands, New Zealand, Norway, Sweden, Switzerland, United Kingdom and the United States, the rate of poor primary care coordination was 5 percent overall and highest in the US at 10 percent. Patients were less likely to experience poor care coordination if their primary care physician knew them well, spent sufficient time with them, involved them in care, and explained things well. Poor primary care coordination was more likely to occur among patients with chronic conditions and patients younger than 65 years. In the US, patients reported similar levels of poor primary care coordination regardless of insurance status, health status, income level and sex, suggesting a systemic issue that distinguishes the efficacy of primary care coordination from that of other countries.
Implications
- The authors note that care coordination gaps have been associated with a higher risk of patients experiencing a medical error, more follow-up appointments, and unnecessary health care spending. They conclude these findings warrant increased efforts to support relationships between primary care providers and patients, especially those who are younger and chronically ill.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- The impact of remote care approaches on continuity in primary care: a mixed-studies systematic review
- The impact of remote care approaches on continuity in primary care: a mixed-studies systematic review
- Barriers to implementation of enhanced recovery after surgery (ERAS) by a multidisciplinary team in China: a multicentre qualitative study
- Protocol for an implementation and realist evaluation of a new organisational model for primary care practices in the canton of Vaud, Switzerland
- Transforming concepts in patient safety: a progress report
- The influence of patient-clinician ethnocultural and language concordance on continuity and quality of care: a cross-sectional analysis
- In This Issue: On-the-Ground Advances & High-Level Influences