
Article Figures & Data
Figures
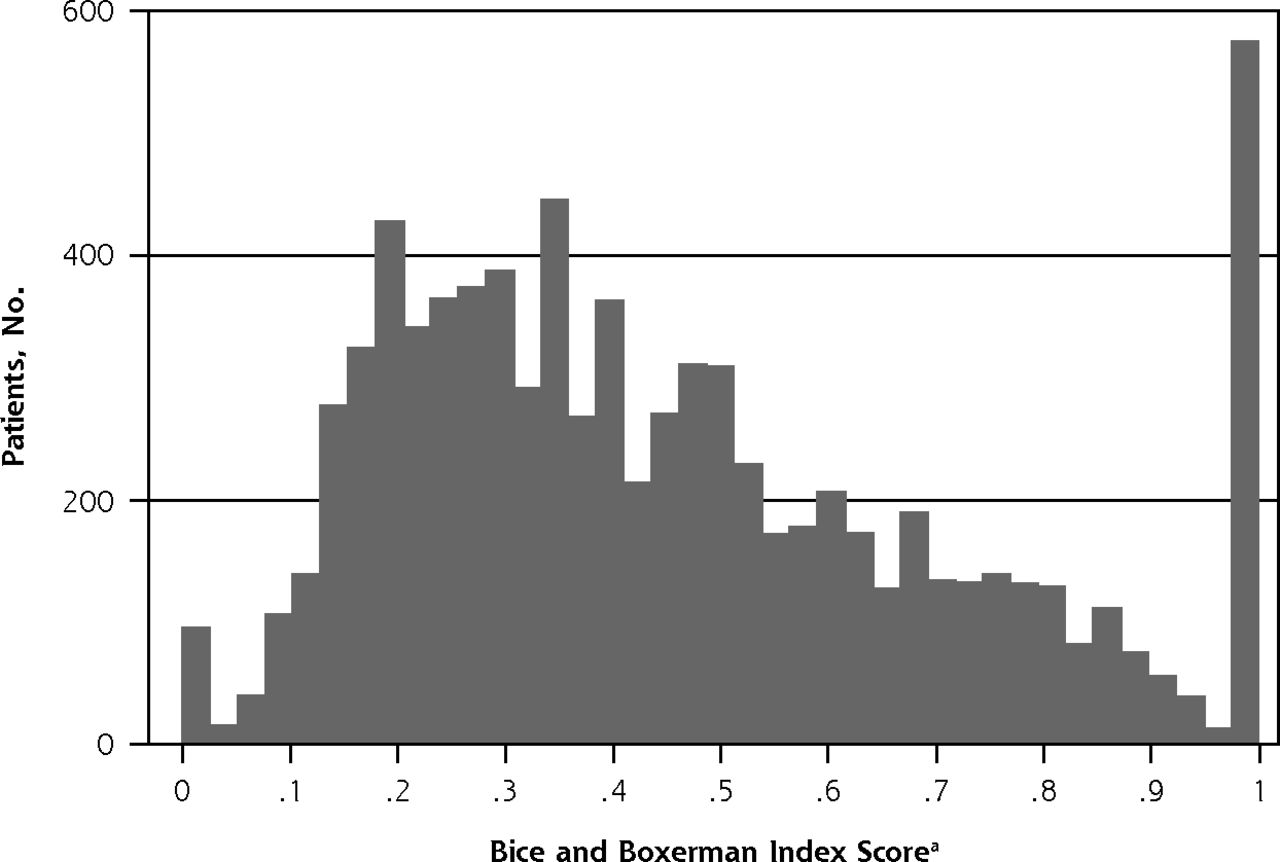
- Figure 1
Distribution of Bice and Boxerman index scores among the 8,248 patients in the prospective cohort analysis.
Higher score indicates greater continuity of care.
- Figure 2
Distribution of appointed general practitioner index scores among the 2,892 patients in the nested case-control analysis.
a Proportion of visits to general practitioner most recently visited. Higher score indicates greater continuity of care.


Tables
- Table 1
Association Between BB Index Score and Risk of Emergency Hospital Admission in the Prospective Cohort Analysis (N = 8,248)
BB Index Score Patients, No. Unadjusted Adjusteda Hazard Ratio (95% CI) P Value Hazard Ratio (95% CI) P Value Of the patient 0 95 1.589 (0.970–2.604) .07 2.272 (1.371–3.764) .001 Q1 (>0 to <0.247) 1,892 1.188 (0.953–1.482) .13 1.123 (0.882–1.431) .35 Q2 (0.247 to <0.383) 1,891 1.091 (0.875–1.358) .44 1.050 (0.830–1.329) .69 Q3 (0.383 to <0.567) 1,901 1.101 (0.885–1.369) .39 1.053 (0.837–1.323) .66 Q4 (0.567 to <1) 1,894 1.031 (0.829–1.281) .78 0.963 (0.768–1.206) .74 1 (ref) 575 1.000 – 1.000 – Of the practice, average Q1 (<0.336) 2,085 1.083 (0.915–1.282) .35 0.968 (0.809–1.158) .70 Q2 (0.366 to <0.436) 2,017 0.916 (0.771–1.089) .32 0.853 (0.718–1.014) .07 Q3 (0.436 to <0.535) 2,068 0.871 (0.735–1.031) .11 0.878 (0.744–1.037) .12 Q4 (0.535) (ref) 2,078 1.000 – 1.000 – BB=Bice and Boxerman; Q=quartile ref=reference category.
Note: Estimated hazard ratios are from mixed-effects Weibull regression analysis.
↵a Adjusted for age, sex, number of general practitioner consultations, having had a previous emergency hospital admission in 2010–2012, deprivation level, general practitioner practice location (urban/rural), number of general practitioners in a practice, and the following morbidities: diabetes, chronic obstructive pulmonary disease, asthma, epilepsy, cancer, stroke, coronary heart disease, chronic renal disease, depression and schizophrenia. For the complete table, see Supplemental Table 2 (http://www.annfammed.org/content/15/6/515/suppl/DC1).
- Table 2
Association Between BB Index Score and Odds of Emergency Hospital Admission in the Nested Case-Control Analysis (N=2,892)
BB Index Score Case Patients, No. Control Patients, No. Unadjusted Adjusteda Odds Ratio 95% CI P Value Odds Ratio 95% CI P Value 0 14 60 1.525 0.752–3.094 .24 2.148 1.009–4.572 .047 Q1 (>0 to <0.257) 188 446 2.674 1.762–4.059 <.001 1.832 1.157–2.901 .01 Q2 (0.257 to <0.395) 171 437 2.137 1.422–3.212 <.001 1.569 1.002–2.427 .049 Q3 (0.395 to <0.576) 176 486 1.989 1.331–2.973 .001 1.370 0.881–2.130 .16 Q4 (0.576 to <1) 171 459 1.935 1.307–2.866 .001 1.170 0.758–1.807 .48 1 (ref) 49 235 1.000 – 1.000 – BB=Bice and Boxerman; Q=quartile; ref=reference category.
Note: Estimated odds ratios from a conditional (fixed-effects) logistic regression analysis.
↵a Adjusted for sex, number of general practitioner consultations, previous hospital admission, and morbidities. For complete table, see Supplemental Table 5, http://www.annfammed.org/content/15/6/515/suppl/DC1.
- Table 3
Cross-Tabulation of a Patient’s Appointed General Practitioner Index Score and Number of General Practitioner Consultations in the Nested Case-Control Analysis (N = 2,892)
General Practitioner Index Score General Practitioner Consultations, No. (%) Total 2–7 8–12 13–19 ≥20 Q1 (0.01 to <0.18) 77 (12.1) 157 (24.7) 167 (26.3) 234 (36.9) 635 (100.0) Q2 (0.18 to <0.40) 188 (28.1) 174 (26.0) 150 (22.4) 157 (24.5) 669 (100.0) Q3 (0.40 to <0.71) 175 (27.1) 153 (23.7) 159 (24.7) 158 (24.5) 645 (100.0) Q4 (>0.71 to <1) 96 (14.6) 170 (25.8) 168 (25.5) 225 (34.1) 659 (100.0) 1 151 (53.7) 61 (21.5) 51 (18.0) 21 (7.4) 284 (100.0) Total 687 (23.8) 715 (24.7) 695 (24.0) 795 (27.5) 2,892 (100.0) Q=quartile.
- Table 4
Association Between Appointed General Practitioner Index Score and Odds of Emergency Hospital Admission in the Nested Case-Control Analysis (N = 2,892)
General Practitioner Index Score Case Patients, No. Control Patients, No. Unadjusted Adjusteda Odds Ratio 95% CI P Value Odds Ratio 95% CI P Value Q1 (0.01 to <0.18) 232 403 3.591 2.393–5.387 <.001 2.318 1.481–3.627 <.001 Q2 (0.18 to <0.40) 177 492 2.096 1.391–3.157 <.001 1.614 1.033–2.522 .04 Q3 (0.40 to <0.71) 160 485 1.932 1.288–2.898 .001 1.496 0.963–2.325 .07 Q4 (0.71 to <1) 151 508 1.585 1.066–2.359 .02 1.031 0.666–1.596 .89 1 (ref) 49 235 1.000 – – 1.000 – – Q=quartile; ref=reference category.
Note: Estimated odds ratios from a conditional (fixed-effects) logistic regression analysis.
↵a Adjusted for sex, number of general practitioner consultations, previous hospital admission, and morbidities. For complete table, see Supplemental Table 7, http://www.annfammed.org/content/15/6/515/suppl/DC1.
Supplemental Appendixes
Supplemental Tables 1-7, Supplemental Figures 1-4, and Supplemental Textbook
Files in this Data Supplement:
- Supplemental data: Tables & Figures - PDF file
The Article in Brief
Continuity of Primary Care and Emergency Hospital Admissions Among Older Patients in England
Peter Tammes , and colleagues
Background This study from the UK explores whether better continuity of care (seeing the same clinician over time) in older patients is associated with a lower risk of emergency hospital admission.
What This Study Found Older patients who experience more discontinuity of care in general practice are at higher risk of emergency hospital admissions. In a study of 10,000 randomly selected patients over age 65, medical records were linked with hospital episode statistics. The study used two research approaches: a prospective cohort approach, to assess the general impact of continuity of care on emergency admission, and a nested case-control approach, to test if seeing a different GP from usual increases the risk of emergency admission during the following 30 days. The prospective approach found a graded non-significant inverse relationship between continuity of care and risk of emergency hospitalization, though patients experiencing least continuity had a risk more than twice as high than those who had complete continuity. The retrospective approach found a graded inverse relationship between continuity of care and emergency hospitalization.
Implications
- Initiatives to enhance continuity of care, the authors suggest, could potentially reduce hospital admissions.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Quantifying, Understanding and Enhancing Relational Continuity of Care (QUERCC): a mixed-methods protocol
- Continuity and locum use for acute consultations: observational study of subsequent workload
- Continuity and breaches in GP care and their associations with mortality for patients with chronic disease: an observational study using Norwegian registry data
- Continuity of care and consultation mode in general practice: a cross-sectional and longitudinal study using patient-level and practice-level data from before and during the COVID-19 pandemic in England
- Personal Continuity and Appropriate Prescribing in Primary Care
- Relational Continuity, Physician Payment, and Team-Based Primary Care in the Canadian Health Care System
- General practice and patient characteristics associated with personal continuity: a mixed-methods study
- Measuring the Value Functions of Primary Care: Physician-Level Continuity of Care Quality Measure
- Association between continuity of primary care and both prescribing and adherence of common cardiovascular medications: a cohort study among patients in England
- Primary care contacts, continuity, identification of palliative care needs, and hospital use: a population-based cohort study in people dying with dementia
- Primary Care Variation in Rates of Unplanned Hospitalizations, Functional Ability, and Quality of Life of Older People
- Is continuity of primary care declining in England? Practice-level longitudinal study from 2012 to 2017
- Continuity of Cancer Care and Collaboration Between Family Physicians and Oncologists: Results of a Randomized Clinical Trial
- How does general practitioner discontinuity affect healthcare utilisation? An observational cohort study of 2.4 million Norwegians 2007-2017
- Retrospective cohort study to investigate the 10-year trajectories of disease patterns in patients with hypertension and/or diabetes mellitus on subsequent cardiovascular outcomes and health service utilisation: a study protocol
- Changes in patient experience associated with growth and collaboration in general practice: observational study using data from the UK GP Patient Survey
- Association between continuity and access in primary care: a retrospective cohort study
- Quality improvements of safety-netting guidelines for cancer in UK primary care: insights from a qualitative interview study of GPs
- The impact of a named GP scheme on continuity of care and emergency hospital admission: a cohort study among older patients in England, 2012-2016
- Tackling multimorbidity in primary care: is relational continuity the missing ingredient?
- Higher Primary Care Physician Continuity is Associated With Lower Costs and Hospitalizations
- In This Issue: Tech, Touch, & Templates for Understanding and Improving Care