
Abstract
PURPOSE No consensus has been reached regarding which anticholinergic scoring system works most effectively in clinical settings. The aim of this population-based cohort study was to examine the association between anticholinergic medication burden, as defined by different scales, and adverse clinical outcomes among older adults.
METHODS From Taiwan’s Longitudinal Health Insurance Database, we retrieved data on monthly anticholinergic drug use measured by the Anticholinergic Risk Scale (ARS), the Anticholinergic Cognitive Burden Scale (ACB), and the Drug Burden Index - Anticholinergic component (DBI-Ach) for 116,043 people aged 65 years and older during a 10-year follow-up. For all 3 scales, a higher score indicates greater anticholinergic burden. We used generalized estimating equations to examine the association between anticholinergic burden (ARS and ACB: grouped from 0 to ≥4; DBI-Ach: grouped as 0, 0–0.5, and 0.5–1) and adverse outcomes, and stratified individuals by age-group (aged 65–74, 75–84, and ≥85 years).
RESULTS Compared with the ARS and DBI-Ach, the ACB showed the strongest, most consistent dose-response relationships with risks of all 4 adverse outcomes, particularly in people aged 65 to 84 years. For example, among those 65 to 74 years old, going from an ACB score of 1 to a score of 4 or greater, individuals’ adjusted odds ratio increased from 1.41 to 2.25 for emergency department visits; from 1.32 to 1.92 for all-cause hospitalizations; from 1.10 to 1.71 for fracture-specific hospitalizations; and from 3.13 to 10.01 for incident dementia.
CONCLUSIONS Compared with the 2 other scales studied, the ACB shows good dose-response relationships between anticholinergic burden and a variety of adverse outcomes in older adults. For primary care and geriatrics clinicians, the ACB may be a helpful tool for identifying high-risk populations for interventions.
- anticholinergic burden
- Anticholinergic Risk Scale (ARS)
- Anticholinergic Cognitive Burden scale (ACB)
- Drug Burden Index - Anticholinergic component (DBI-Ach)
- emergency department visits
- hospitalizations
- fractures
- dementia
- adverse effects
- older adults
- aged
- primary care
INTRODUCTION
Medications with anticholinergic properties are used for a variety of diseases and constitute 30% to 50% of all medications commonly prescribed to older adults.1 The aging-related decline of acetylcholine production may increase the vulnerability of older adults to anticholinergic adverse effects,2,3 such as blurred vision, urinary retention, tachycardia, drowsiness, and cognitive impairments.4 The blurred vision and dizziness caused by exposure to anticholinergic agents may further result in falls and associated adverse events.5–7 The cognitive impairment associated with exposure to these medications may lead to chronic cognitive deficits such as dementia.4,8 The cumulative effect of multiple anticholinergic agents, the so-called anticholinergic burden, has been used as an indicator for suboptimal prescribing in older adults.9 In recent years, several scoring systems have been developed to quantify anticholinergic burden, such as the Anticholinergic Risk Scale (ARS),10 the Anticholinergic Cognitive Burden Scale (ACB),8 and the Drug Burden Index - Anticholinergic component (DBI-Ach).11
These scales differ considerably in how they were developed, in their method of measuring anticholinergic burden, and in the results they yield. Notably, their approaches to identifying medications with anticholinergic properties to be included in their scales differ greatly. The ARS ranks the 500 most commonly prescribed drugs in a Veterans Affairs Health Care System by their dissociation constant for the cholinergic receptor,10 while the ACB ranking was developed through a systematic literature review and expert opinions.8 Medications were included in the DBI-Ach if they had demonstrated clinically important anticholinergic effects that were documented in country-specific drug monographs or registered product information.11 To date, no consensus has been reached regarding which scoring system is most useful in clinical settings. Moreover, existing studies of the various scoring systems have a variety of limitations: evaluation of only a single system,12–14 application of different cutoff values for anticholinergic burden between scoring systems, small sample sizes,15,16 cross-sectional designs,15,16 and short follow-up periods17 (≤1 year). All of these limitations preclude a clear answer to this clinical question.
To address these limitations, the main aim of this study was to compare the associations between longitudinal anticholinergic burden, as defined by the different scales, and adverse clinical outcomes among older adults.
METHODS
Study Design and Data Set
We conducted a retrospective population-based cohort study using Taiwan’s National Health Insurance Research Database (NHIRD).18 Implemented in 1995, the National Health Insurance program covers more than 99% of the total population (23 million people) in Taiwan.19 The NHIRD contains comprehensive data about demographic information, health service use, prescriptions, and diagnoses based on the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). We used a subset of the NHIRD—the Longitudinal Health Insurance Database (LHID),18 which contains the claims data of 2 million randomly selected beneficiaries from the NHIRD—to develop a 12-year (2000–2011) panel of claims for analysis. These individuals were sampled from the registry for beneficiaries of the NHIRD in the years 2000 (1 million) and 2005 (1 million). The age and sex distributions of the LHID do not differ significantly from those of the parent NHIRD cohort.18
This study was approved by the institutional review board of the National Taiwan University Hospital (National Taiwan University Hospital Research Ethics Committee No. 201401004W). Because the identification numbers of all individuals in the NHIRD were encrypted to protect their privacy, the study was exempted from full board review, and informed consents were waived.
Study Population
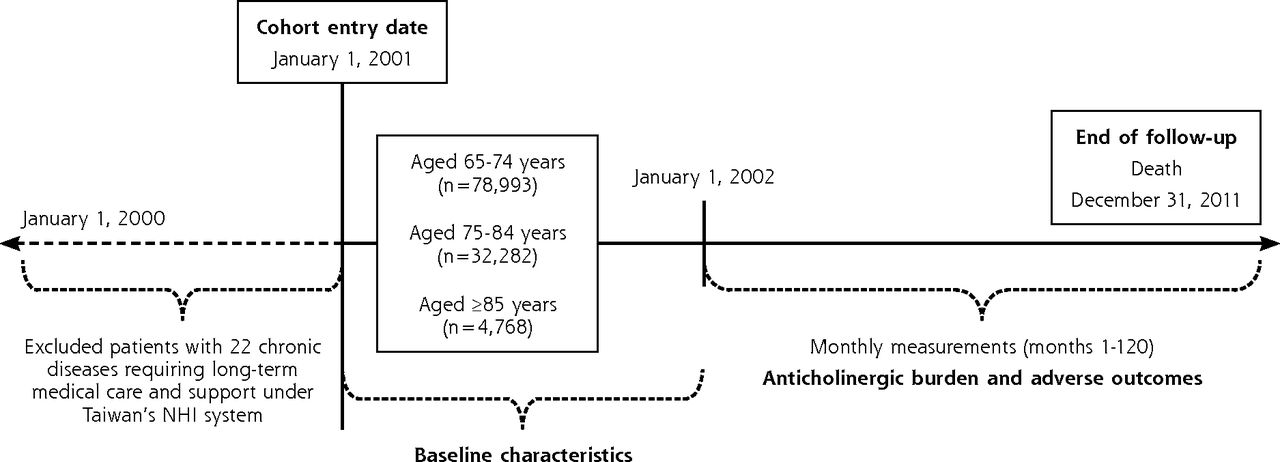
The study cohort consisted of individuals who were aged 65 years and older at study entry (January 1, 2001) (Figure 1). We excluded people who in the year preceding the recruitment date received a diagnosis of any of the 22 chronic diseases requiring long-term medical care and support under Taiwan’s National Health Insurance system, including cancer, rheumatoid arthritis, and systemic lupus erythematosus (Supplemental Appendix 1, available at http://www.AnnFamMed.org/content/15/6/561/suppl/DC1/).18 All eligible individuals were categorized into 3 age-groups based on their age at enrollment: aged 65 to 74 years (the so-called young-old), 75 to 84 years (middle-old), and 85 years and older (oldest-old). We examined potentially different impacts of anticholinergic burden on adverse outcomes across the 3 age-groups because we expected that drug use pattern would change with advancing age. Baseline characteristics were collected in the first year after enrollment (2001).
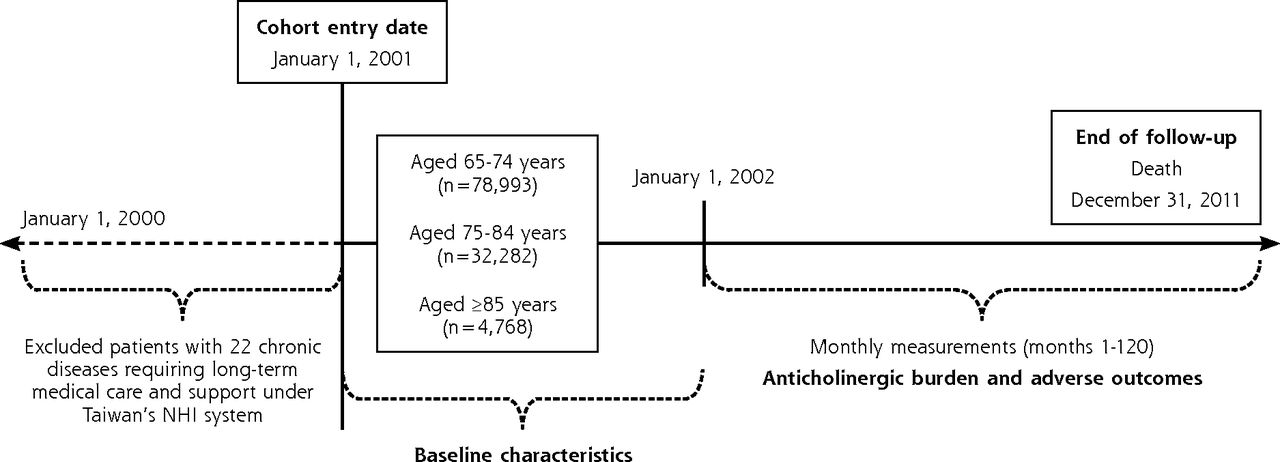
Study design.
NHI=National Health Insurance.
Anticholinergic Burden Scales
During the 10-year follow-up period, we retrieved data on longitudinal anticholinergic burden assessed monthly for 120 months as measured by the ARS (Supplemental Appendix 2, available at http://www.AnnFamMed.org/content/15/6/561/suppl/DC1/), by the ACB (Supplemental Appendix 3, available at http://www.AnnFamMed.org/content/15/6/561/suppl/DC1/), and by the DBI-Ach (Figure 1). We selected these scales to represent 3 distinct methods of identifying drug lists in clinical settings and measuring anticholinergic burden, as described in the Introduction section.
Both the ARS and ACB have 4-point scales (0, limited or none; 1, moderate; 2, strong; 3, very strong) to rank the anticholinergic activity of each medication, so a patient’s score on each of these scales was calculated as the sum of the rankings for all prescribed drugs.8,10,20 For both, a higher score indicates higher anticholinergic burden. If a patient receives a medication ranked 1 and another medication ranked 2 in the list of ARS, then the patient’s ARS score is 3. There is no published consensus, however, regarding the optimal cutoff levels for ARS and ACB. We therefore grouped together individuals having scores of 4 or higher because we had relatively few with scores that high.
To calculate the DBI-Ach score, we first needed to identify country-specific medications with anticholinergic effects.11 On the basis of our previous study,21 we used medications listed in the ARS to calculate this score. Specifically, DBI-Ach was calculated as

where D is the daily dose and δ is the minimum recommended daily dose as approved by the regulator; this calculation was established based on a series of assumptions made to derive a pharmacologic equation that incorporated the concept of dose-response.11 For the DBI-Ach score, we replaced the minimum recommended daily dose used in the calculation of this score as suggested previously by Faure et al22 with the defined daily dose. The definition of defined daily dose is the average maintenance dose per day for a drug used for its main indication in adults as defined by the World Health Organization.23 The DBI-Ach score ranges from 0 to 1, with 0.5 indicating that an individual is exposed to an anticholinergic medication at the minimum recommended daily dose, and higher scores indicating greater burden.
We selected only those drugs that were prescribed for more than 7 days in each month to calculate anticholinergic burden for each of the 3 scoring systems. Although drugs for short-term symptom relief such as antihistamines are often sold over the counter in other countries, they are reimbursed under Taiwan’s National Health Insurance system. Including exposure to these drugs (ie, usually a 3-day supply) in our study could have resulted in overestimation of anticholinergic burden.
Adverse Outcomes
During the same 10-year period, we retrieved data on 4 adverse outcomes of interest: emergency department visits, all-cause hospitalizations, fracture-specific hospitalizations, and incident dementia. We defined a fracture-specific hospitalization as a hospital admission with a discharge diagnosis of fracture (ICD-9-CM codes 800–829).24 Patients with incident dementia were defined as those who had at least 3 outpatient or inpatient claim records of a diagnosis of dementia (290.xx, 294.1x, 331.0, 331.2).25 The first date of any of these diagnosis codes was considered the date of onset. We excluded patients with dementia at baseline (1 year after cohort enrollment) when analyzing the association between anticholinergic burden and incident dementia.
Statistical Analysis
We used generalized estimating equation (GEE)26 models (SAS PROC GENMOD; SAS Institute Inc) with a logit link and first-order autoregressive correlation structure to examine the association between anticholinergic burden (measured by scores) and adverse outcomes, taking into account the repeated measurements for the same individual. The GEE models were adjusted for sex and time-varying comorbidities, annually measured by Charlson Comorbidity Index27 (higher index indicates more comorbidities). For the ARS and ACB scales, we further adjusted the defined daily dose 23 of drugs with anticholinergic properties in the GEE models to compare the 3 scales. Separate models were fitted to each age-group and each scale. The results of all GEE models are presented as adjusted odds ratios (aORs) with 95% CIs for each of the 3 age-groups (65–74 years, 75–84 years, and ≥85 years). All statistical analyses were performed with SAS version 9.3, and a P value <.05 was considered statistically significant.
RESULTS
We analyzed data from a total of 116,043 older adults: 78,993 (68.07%) aged 65 to 74 years, 32,282 (27.82%) aged 75 to 84 years, and 4,768 (4.11%) aged 85 years and older (Table 1). In the first year after cohort enrollment (baseline period), the proportion of patients who received anticholinergic agents as ascertained by the ARS, ACB, and DBI-Ach was 37.31%, 59.99%, and 37.31%, respectively. The average monthly anticholinergic burden measured by the 3 scoring systems in all older adults studied was 0.26, 0.60, and 0.04, respectively.
Baseline Characteristics and Health Care Use of Study Cohort, Overall and Stratified by Age
The mean duration of follow-up was 8.31 years. Number of events for each adverse outcome in each age-group during follow-up are provided in Tables 2 through 5.
Anticholinergic Burden and Emergency Department Visits in Older Adults
Anticholinergic Burden and All-Cause Hospitalizations in Older Adults
Anticholinergic Burden and Fracture-Specific Hospitalizations in Older Adults
Anticholinergic Burden and Incident Dementia in Older Adults
Of the 3 scales for assessing anticholinergic burden, only the ACB and DBI-Ach showed clear dose-response relationships with increased odds of emergency department visits (Table 2) and all-cause hospitalizations (Table 3) in all age-groups.
Only the DBI-Ach showed a dose-response relationship with fracture-specific hospitalizations in all age-groups (Table 4). The ARS and ACB showed dose-response relationships with fracture-specific hospitalizations in individuals aged 65 to 74 years and 75 to 84 years, but not in those aged 85 years and older. The ACB showed a dose-response relationship with incident dementia in patients aged 65 to 74 years and 75 to 84 years, but not in patients aged 85 years and older (Table 5); the other scales did not show such relationships in any of the age-groups.
DISCUSSION
To the best of our knowledge, this is the first study to compare long-term associations between anticholinergic burden measured by different scales and adverse clinical outcomes, with an average follow-up period exceeding 8 years. We found that among the 3 scales, only anticholinergic burden assessed with the ACB showed a dose-response relationship with all outcomes studied—emergency department visits, all-cause hospitalizations, fracture-specific hospitalizations, and incident dementia.
Our study expands on the current knowledge of anticholinergic burden in the older population in many ways. First, by using a nationwide cohort of older adults with fairly long follow-up, our study allows head-to-head comparisons of longitudinal anticholinergic burden derived from the ARS, ACB, and DBI-Ach scales and associated clinical outcomes, which have not been previously reported in the literature. Some other studies have tried to compare the ARS and ACB, but were limited by their small sample sizes15,28 and a 1-time cross-sectional study design.17 Second, our study provides important insights by linking anticholinergic burden to 4 key clinical outcomes, whereas most existing studies have examined only the discrepancies between scales.29,30 Ours is also the first to demonstrate an association between anticholinergic burden and emergency department visits, which has important clinical implications. Another aspect that distinguishes this study from previous ones is the definition of adverse outcomes considered. Although previous studies found that use of anticholinergics was associated with falls5,6,12 and admissions due to falls7,17 resulting from adverse effects such as blurred vision and dizziness,31 our study used fracture-specific hospitalizations as an end point to further capture the adverse effects of anticholinergic burden. Additionally, we examined the link of anticholinergic burden with incident dementia, instead of with cognitive function as done in most of the existing studies.32–34
Our findings are consistent with those of previous studies15,17 in that the proportion of patients who received anticholinergic agents measured by the ACB (59.99%) was higher than that measured by the ARS (37.31%) at the baseline assessment. This discrepancy between scoring systems may result from the different collections of drugs included in the scales. In our study, the commonly used anticholinergics contained in the ACB were mainly cardiovascular drugs such as dipyridamole, isosorbide mononitrate, nifedipine, atenolol, digoxin, and furosemide, whereas the commonly used anticholinergics contained in the ARS were mainly antihistamines or drugs affecting the nervous system, such as quetiapine and trazodone (data not shown). These findings are also in line with those of several previous studies.13,15,32,35 Primary care and geriatrics clinicians should pay special attention to these medications.
Unlike the ACB score, the ARS score showed a dose-response relationship only with regard to fracture-specific hospitalizations, exhibiting a U-shaped relationship with the other adverse outcomes studied. In particular, we found that the ARS score had a U-shaped relationship with risk of incident dementia, as Pasina et al15 have likewise reported. Our analyses showed that an ARS score of 1 was associated with a 10-fold increase in the odds of incident dementia. A potential explanation for this association is that anticholinergic drugs (particularly those contained in the ARS) may be prescribed to treat symptoms of dementia, such as insomnia or depression. The DBI-Ach score also showed a dose-response association with adverse outcomes. Calculating this score requires more effort, however, and it may not be very efficient to use it in routine daily practice.
There are some limitations to this study, mainly due to the use of claims data. First, we were not able to include drugs not reimbursed by Taiwan’s National Health Insurance, nor could we consider variables not routinely recorded in the NHIRD such as body mass index, education level, and patient adherence. Second, with regard to the consistency of the study design, we did not control for a few risk factors that may affect the association between anticholinergic burden and adverse outcomes, such as osteoporosis (a risk factor for fracture) and depression and Parkinson disease (risk factors for dementia). Consistent results were still obtained, however, after adjusting for these risk factors. Third, our findings may not be generalizable to other, non-Asian populations because of different prescribing patterns. In addition, the exclusion of older adults having 22 chronic diseases requiring long-term medical care and support under Taiwan’s National Health Insurance system and relatively small number of participants in the oldest-old age-group (aged ≥85 years) may limit the generalizability of our study to these patients. A large proportion of people in this age-group may be lost to follow-up over 10 years. Fourth, only drugs prescribed for 7 or more days within a 1-month period were considered in measurement of anticholinergic burden. Short-term use of anticholinergic agents, however, may also affect clinical outcomes. In addition, use of medications may represent underlying disease; for example, many of the medications listed in the ACB are cardiovascular drugs, which may affect clinical outcomes as well. Fifth, we did not include total number of medications as a covariate in the analyses because of concerns about colinearity between this number and anticholinergic burden. A previous study has reported that patients who were prescribed 6 to 10 medications or 11 or more medications were significantly more likely to receive anticholinergic prescriptions (OR = 3.41; 95% CI, 2.23–5.22 and OR = 4.69; 95% CI, 2.99–7.34, respectively).36 Lastly, although these scoring systems show an association between high anticholinergic burden and adverse outcomes, we could not establish causation from this observational study.
In conclusion, compared with the ARS and the DBI-Ach, the ACB consistently showed dose-response relationships with a variety of adverse outcomes. For primary care and geriatrics clinicians, the ACB may be a good tool for identifying high-risk populations for interventions.
Footnotes
Conflicts of interest: authors report none.
Funding support: This study was supported by a research grant (MOST 104-2410-H-002-225-MY3) sponsored by the Ministry of Science and Technology, Taiwan.
Disclaimer: The funding source had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and the decision to submit the manuscript for publication.
Author contributions: Dr Hsiao had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Hsu, Chen, Hsiao. Acquisition, analysis, or interpretation of data: all authors. Drafting of the manuscript: Hsu, Hsiao. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: Hsu, Wen, Hsiao. Obtained funding: Hsiao. Administrative, technical, or material support: Hsiao. Study supervision: Chen, Hsiao.
Supplementary materials: Available at http://www.AnnFamMed.org/content/15/6/561/suppl/DC1/.
- Received for publication October 17, 2016.
- Revision received May 16, 2017.
- Accepted for publication June 22, 2017.
- © 2017 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Anticholinergic drugs and clinical outcomes in older people with and without dementia- A systematic Review
- Association between anticholinergic burden and dementia in UK Biobank
- Anticholinergic burden and fractures: a protocol for a methodological systematic review and meta-analysis
- Influence of opioid prescribing standards on drug use among patients with long-term opioid use: a longitudinal cohort study
- In This Issue: Tech, Touch, & Templates for Understanding and Improving Care