
Article Figures & Data
Figures
- Figures 1a–d
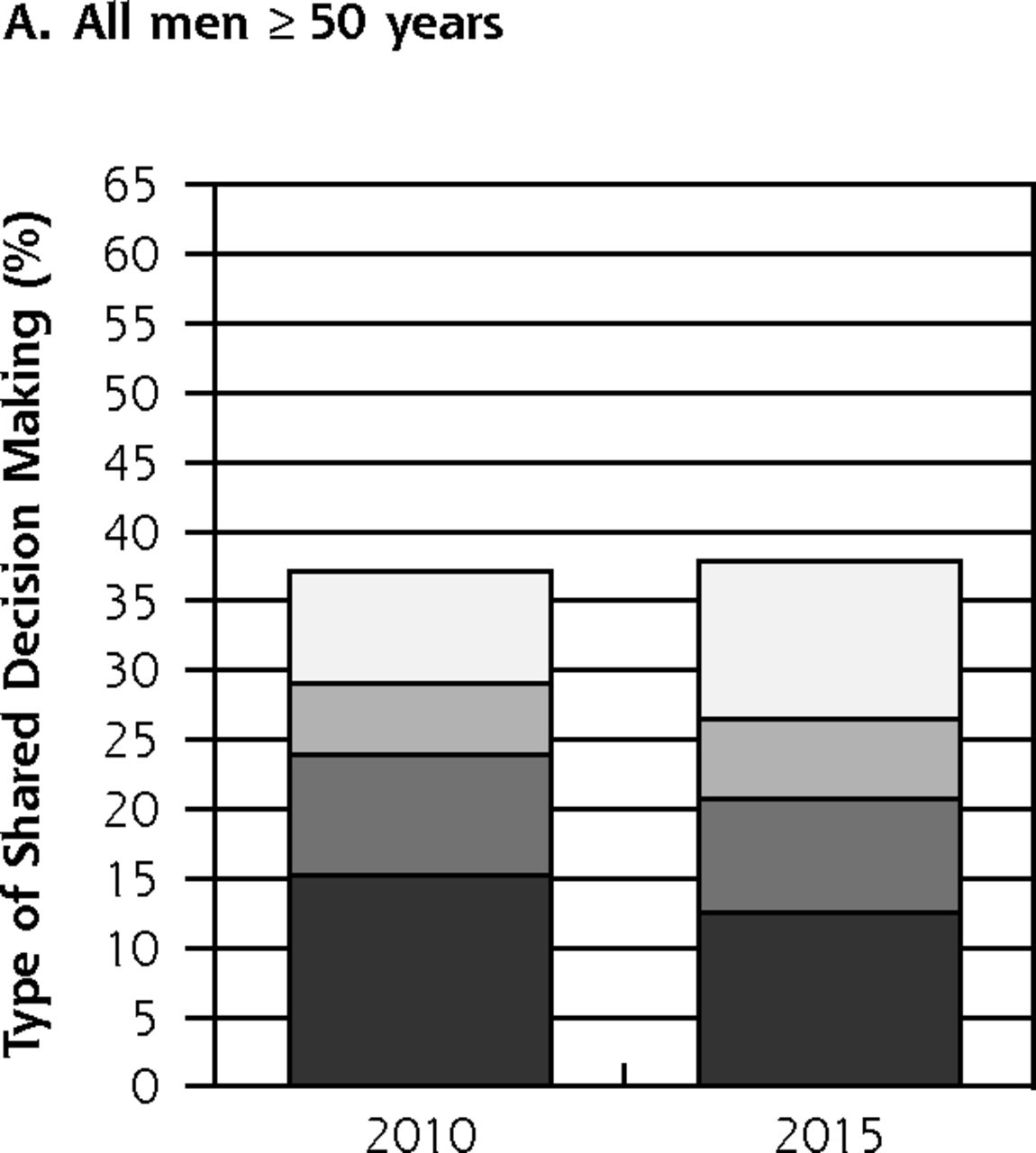
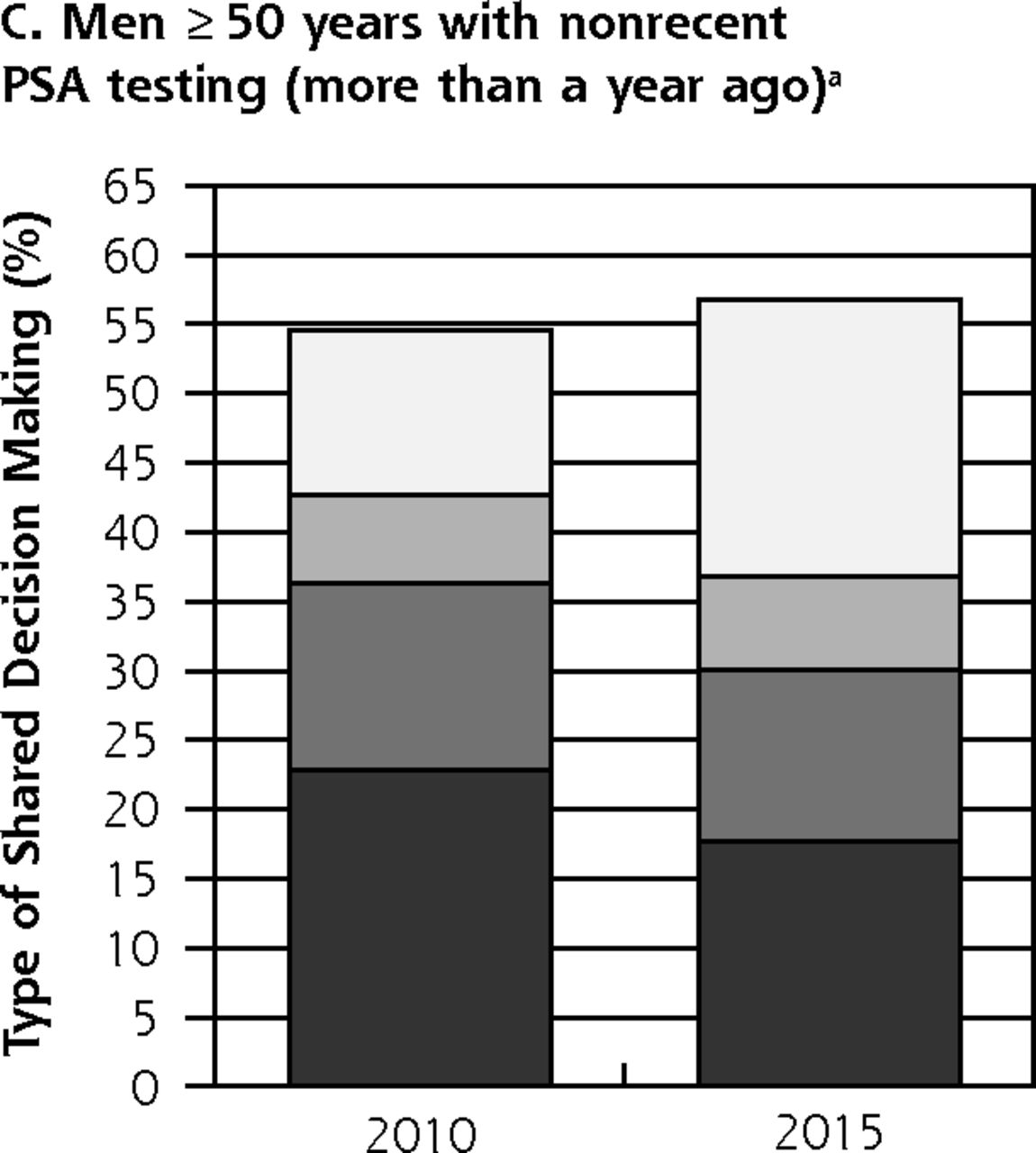
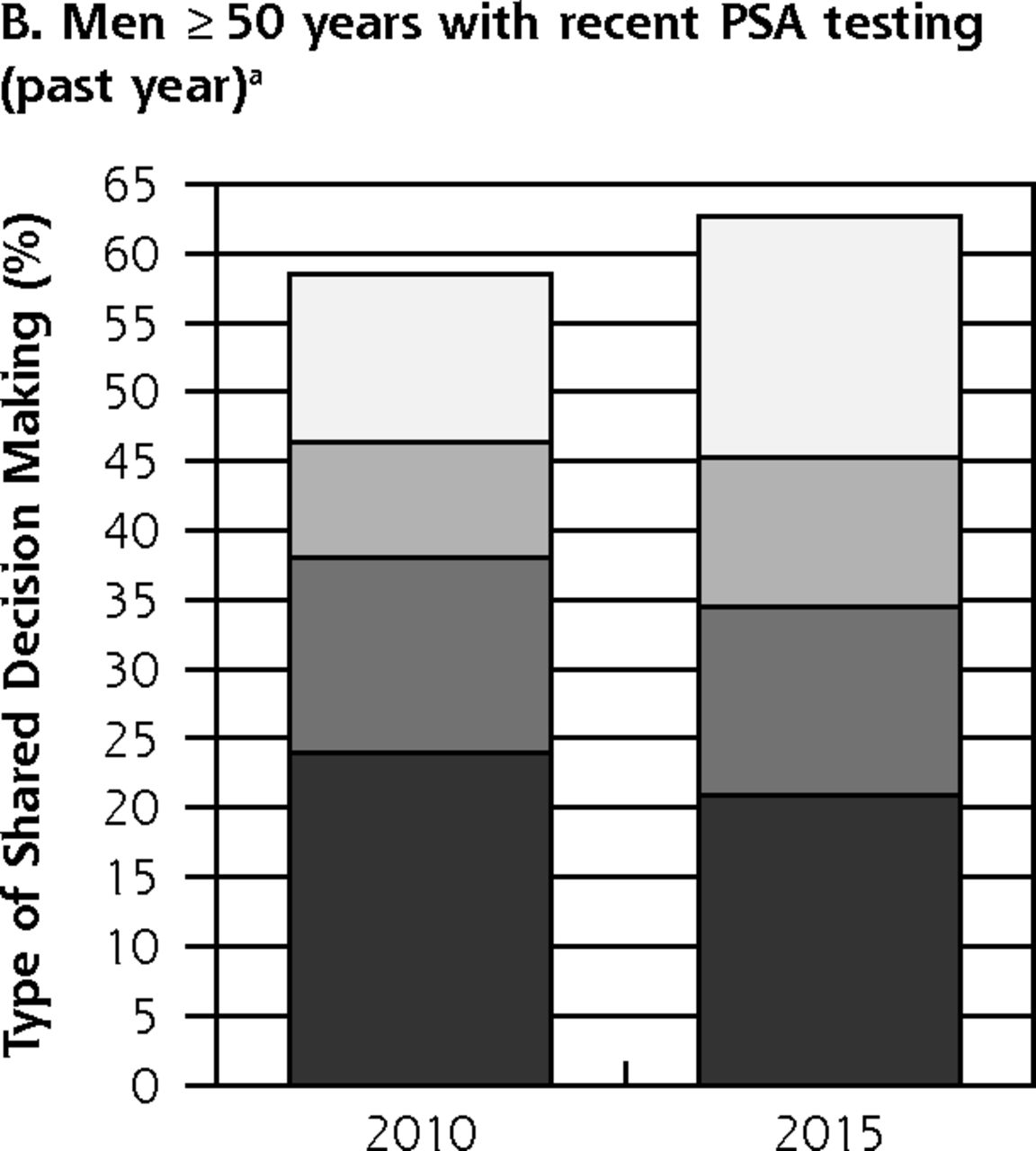
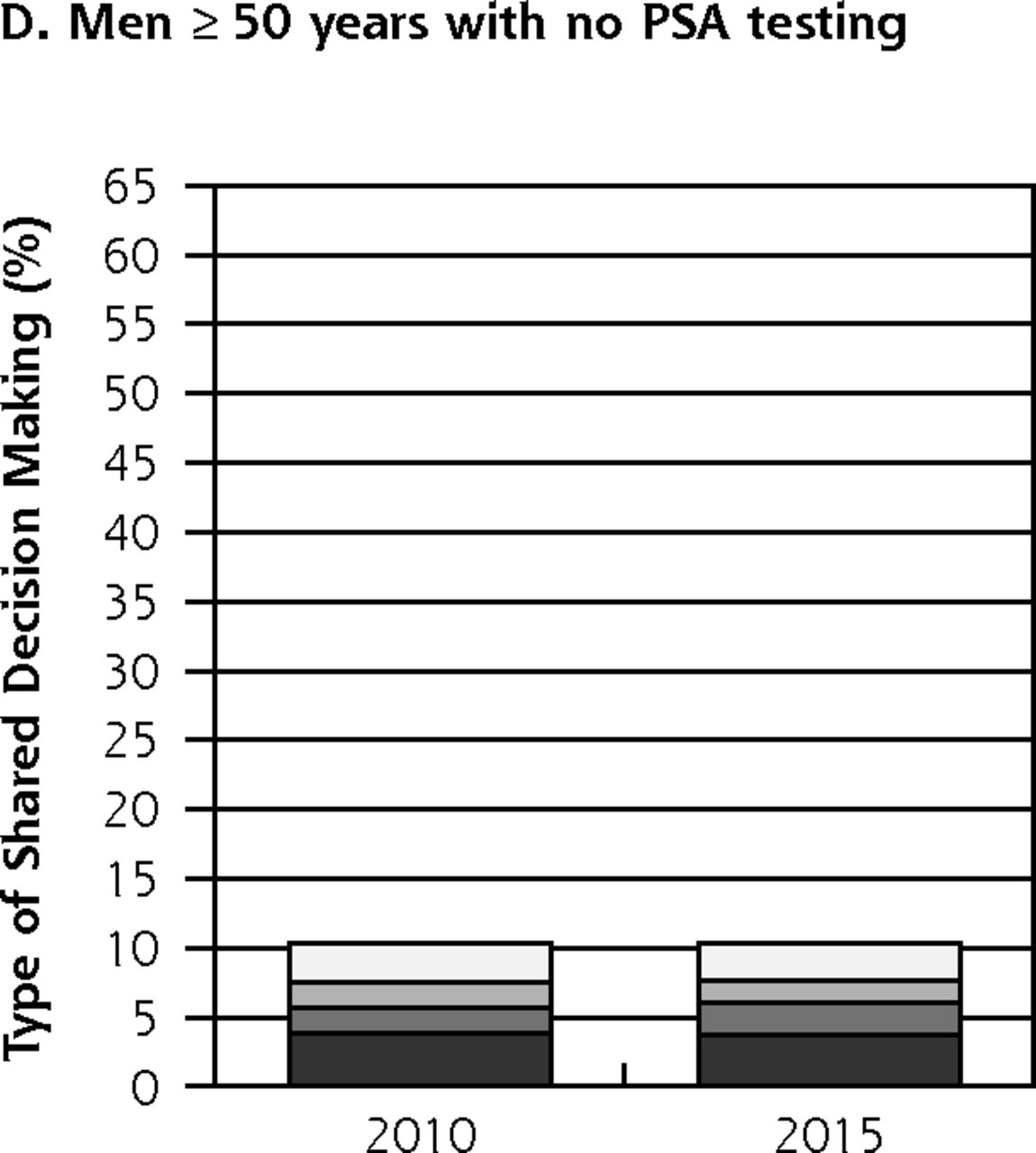
Receipt of shared decision making among men by PSA testing category, NHIS 2010 and 2015.
NHIS = National Health Interview Survey; PSA = prostate-specific antigen.
a Among men with PSA testing for routine reasons.


Tables
- Table 1
Receipt of Shared Decision Making Among Men by Testing History and Age, NHIS 2010 and 2015 (n = 9,598)
Testing History and Age ≥1 Element of SDM Advantages Advantages and Disadvantages Full 2010 2015 2010 2015 2010 2015 2010 2015 Among men with recent PSA testing (n = 3,079), % ≥50 y 58.5 62.6 23.9 20.9 14.1 13.6 12.2a 17.4a 50–64 y 58.3 63.4 23.7 21.3 14.6 15.0 11.6a 17.3a 65–74 y 57.4 63.5 23.3 19.8 14.1 12.1 13.6a 19.0a ≥75 y 61.7 58.0 26.6 22.0 11.7 11.4 11.8 13.9 Among men with nonrecent PSA testing (n = 2,104), % ≥50 y 54.6 56.8 22.9a 17.7a 13.4 12.4 11.9a 20.0a 50–64 y 56.5 55.1 23.2a 15.7a 13.3 12.2 14.3 19.7 65–74 y 48.9a 59.4a 20.9 21.3 14.8 13.3 7.0b 19.8 ≥75 y 55.4 58.7 24.7 18.5 11.5 11.7 9.6a 21.5a Among men with no PSA testing (n = 4,415), % ≥50 y 10.4 10.3 3.9 3.7 2.1 1.8 2.8 2.6 50–64 y 10.4 10.0 4.0 3.5 1.8 2.4 2.6 3.1 65–74 y 10.6 9.8 4.8b 5.3 1.5b 1.5b 3.0b 1.6 ≥75 y 10.0 9.7 2.1b 1.9b 2.2b 2.2b 4.6b 1.0b - Table 2
Adjusted Prevalence Ratios and 95% CI Predicting Shared Decision Making Among Men Who Received PSA Testing in the Past Year for Routine Reasons, NHIS 2010 and 2015
Characteristic ≥1 Element of SDM vs None aPR (95% CI) Advantages vs None aPR (95% CI) Advantages and Disadvantages vs None aPR (95% CI) Full vs None aPR (95% CI) Among men with recent PSA testinga Year 2010 1.00 [Reference] 1.00 [Reference] 1.00 [Reference] 1.00 [Reference] 2015 1.04 (0.98–1.11) 0.82 (0.71–0.96)b 0.94 (0.79–1.12) 1.51 (1.28–1.79)b Age 50–64 y 1.00 [Reference] 1.00 [Reference] 1.00 [Reference] 1.00 [Reference] 65–74 y 1.24 (0.88–1.76) 0.90 (0.69–1.18) 0.89 (0.61–1.30) 1.02 (0.77–1.35) ≥75 y 0.99 (0.63–1.54) 0.96 (0.07–1.32) 0.78 (0.52–1.18) 0.95 (0.69–1.30) Among men with nonrecent PSA testingc Year 2010 1.00 [Reference] 1.00 [Reference] 1.00 [Reference] 1.00 [Reference] 2015 1.04 (0.93–1.15) 0.78 (0.61–0.98)b 0.90 (0.69–1.18) 1.69 (1.29–2.20)b Age 50–64 y 1.00 [Reference] 1.00 [Reference] 1.00 [Reference] 1.00 [Reference] 65–74 y 1.08 (0.90–1.30) 1.41 (0.91–2.20) 0.95 (0.54–1.65) 0.75 (0.49–1.16) ≥75 y 1.13 (0.93–1.37) 1.39 (0.83–2.31) 0.80 (0.42–1.54) 0.85 (0.54–1.33) Among men with no PSA testingd Year 2010 1.00 [Reference] 1.00 [Reference] 1.00 [Reference] 1.00 [Reference] 2015 0.97 (0.76–1.24) 0.91 (0.60–1.37) 1.27 (0.74–2.18) 0.90 (0.56–1.43) Age 50–64 y 1.00 [Reference] 1.00 [Reference] 1.00 [Reference] 1.00 [Reference] 65–74 y 0.99 (0.60–1.62) 1.07 (0.40–2.86) 0.62 (0.24–1.55) 1.04 (0.53–2.01) ≥75 y 0.85 (0.45–1.58) 0.45 (0.13–1.60) 1.05 (0.37–2.93) 1.47 (0.70–3.10) aPR = adjusted prevalence ratio; NHIS = National Health Interview Survey; PSA = prostate-specific antigen; SDM = shared decision making.
Note: Each model is adjusted for: age, survey year, race/ethnicity, educational attainment, insurance type, immigration status, and geographic region.
↵a Model includes 2,592 men; 487 men excluded from each model based on missing educational attainment and immigration data.
↵b Statistically significant at P <.05.
↵c Model includes 1,752 men; 352 men excluded from each model based on missing educational attainment and immigration data.
↵d Model includes 4,246; 169 men excluded from each model based on missing educational attainment and immigration data.
The Article in Brief
Recent Patterns in Shared Decision Making for Prostate-Specific Antigen Testing in the United States
Stacey A. Fedewa , and colleagues
Background There is consensus that the decision to undergo prostate-specific antigen testing for prostate cancer screening should be shared by patients and clinicians, but rates of shared decision making are low. This study examines whether there have been recent changes in shared decision-making for PSA testing.
What This Study Found Although there has been no increase in shared decision making for PSA testing, the content of discussions has become more comprehensive. The study compared responses to the National Health Interview Survey in 2010 and 2015 among men age 50 and older (n=9598). In this nationally representative sample, a similar proportion (approximately 60 percent) of men with recent PSA testing reported one or more elements of shared decision-making in both 2010 and 2015. They also reported a modest shift away from discussions limited to the advantages of PSA testing toward full shared decision-making in which advantages, disadvantages, and uncertainties were discussed (12 percent of recently-tested men in 2010 compared to 17 percent in 2015). One in 10 men who did not receive PSA testing reported receiving one or more elements of shared decision making, a number which did not change during the study period.
Implications
- The results suggest that, contrary to guideline recommendations, many men receiving PSA testing still do not receive shared decision making and a limited number of men without PSA testing receive one or more shared decision-making elements.
- The authors call for new and innovative strategies to achieve more widespread application of shared decision-making for men considering PSA testing.
Supplemental Figure and Tables
Supplemental Figure and Tables
Files in this Data Supplement:
- Supplemental data: Figure and Tables - PDF file




{kind=link}
{kind=link}
{kind=link}
{kind=link}