
Article Figures & Data
Figures
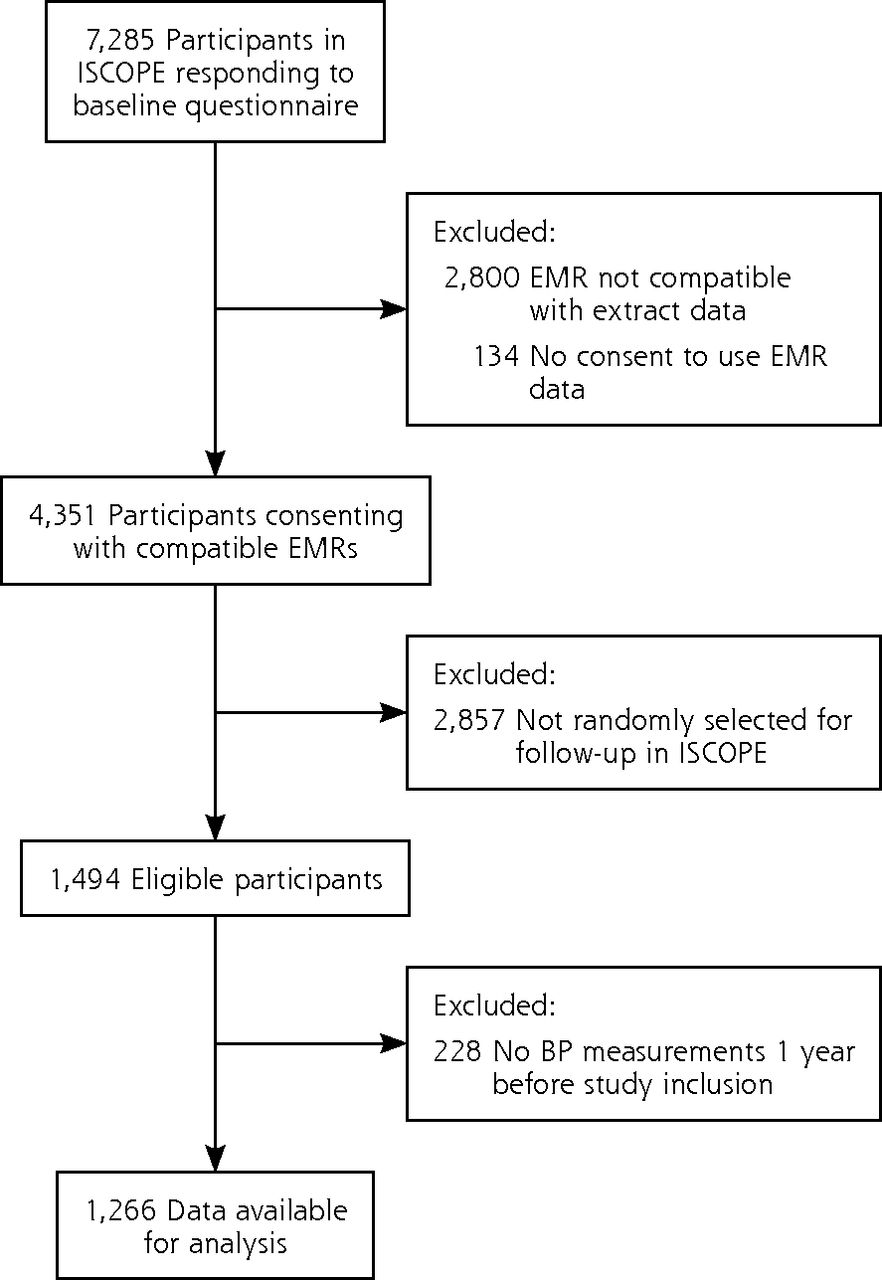
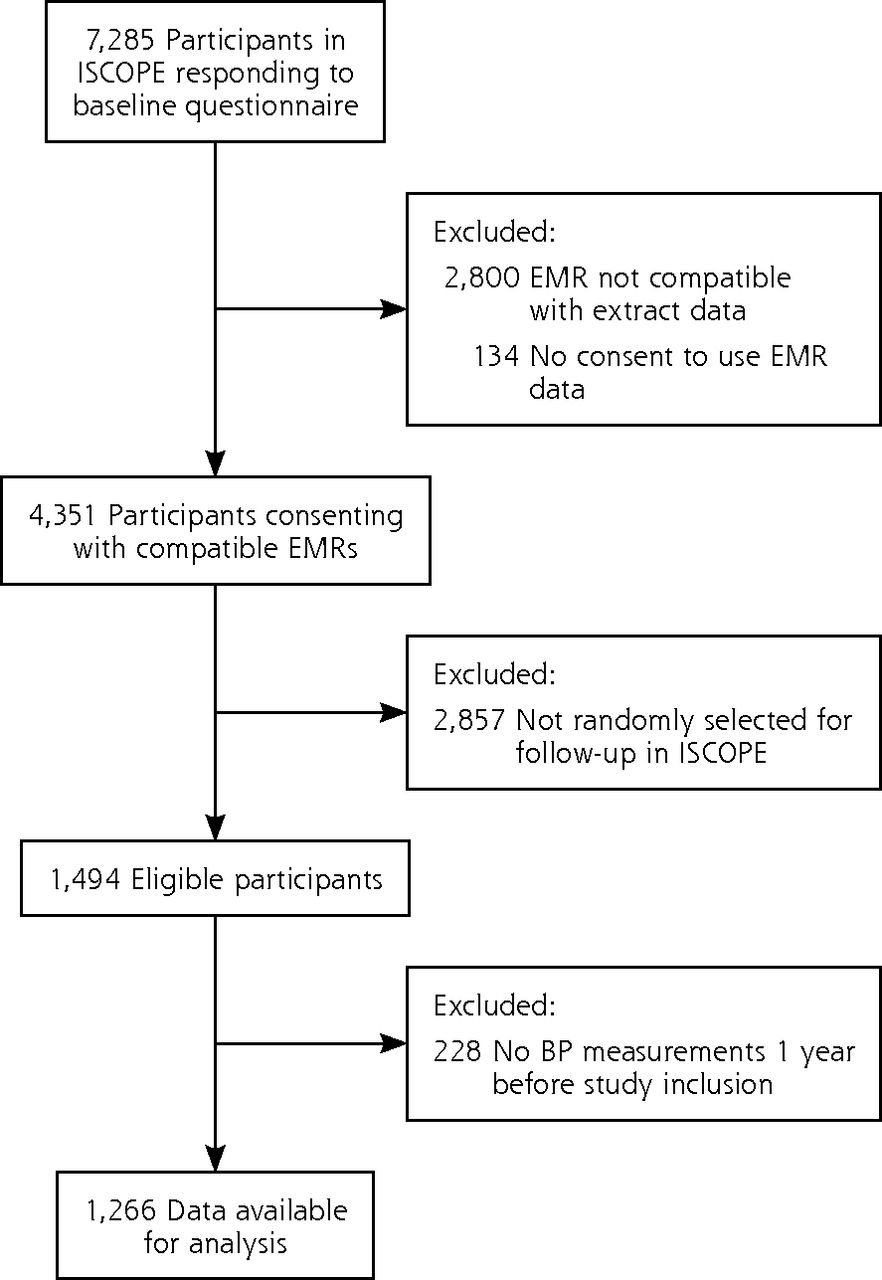
- Figure 1
Study flowchart
BP = blood pressure; EMR = electronic medical record; ISCOPE = Integrated Systematic Care for Older Persons study.
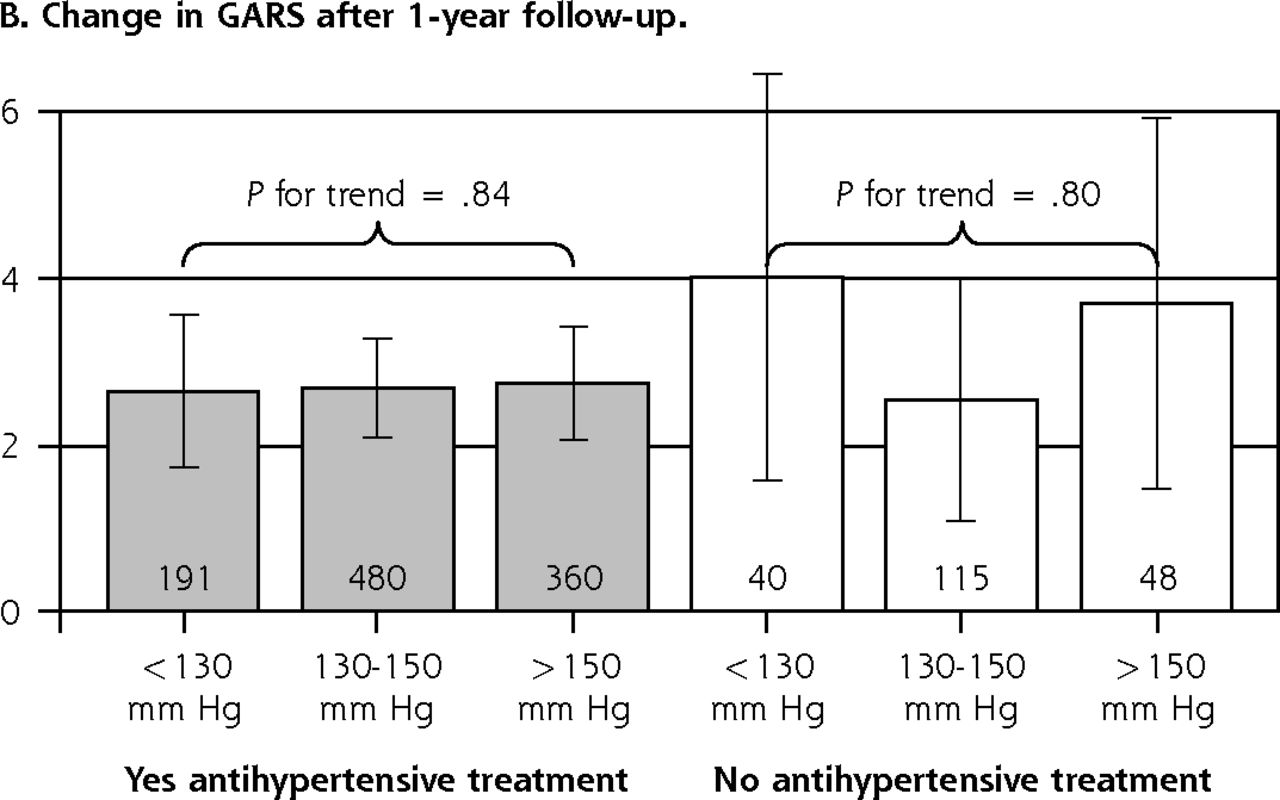
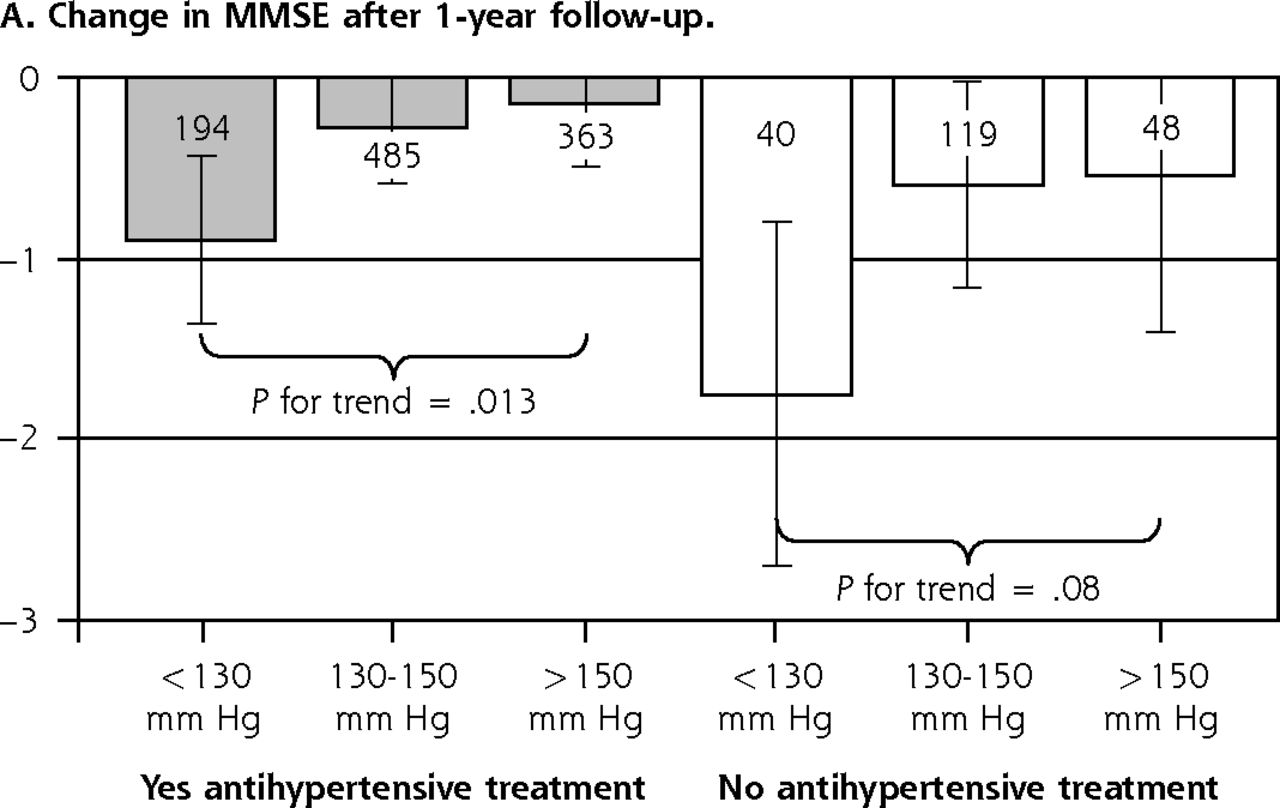
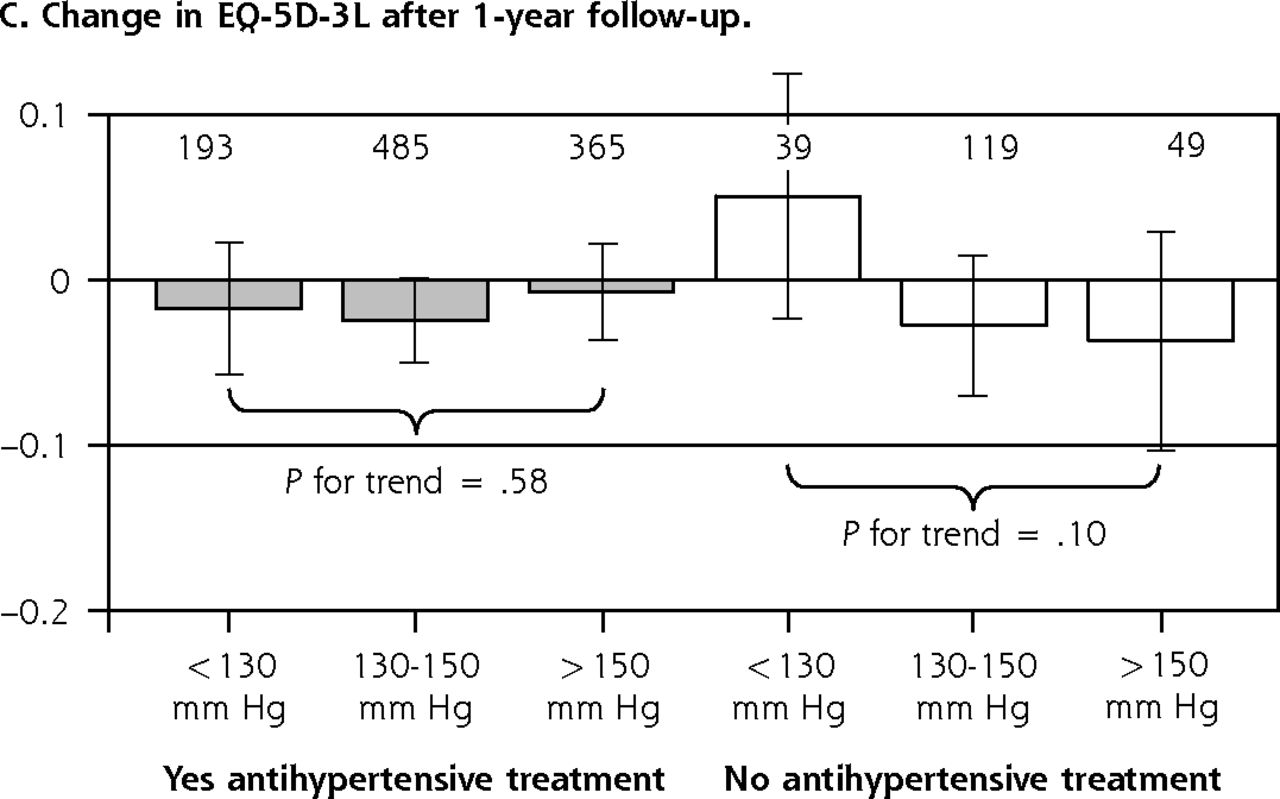
- Figure 2
Associations between systolic blood pressure, antihypertensive treatment, and change in function after a 1-year follow-up.
GARS = Groningen Activity Restriction Scale; MMSE = Mini-Mental State Examination.
Note: Numbers in or above bars equal number of participants.
Estimates, 95% CI, and P for trend from crude mixed-effects linear regression accounting for clustering within family physicians. A. Cognitive function measured by MMSE (fewer points = cognitive decline). B. Daily functioning measured by GARS (more points = more disability). C. Quality of life measured by EQ-5D-3L (fewer points = lower quality of life).


Tables
- Table 1
Baseline Characteristics of Participants Overall and Grouped by Antihypertensive Treatment (n = 1,266)
Characteristic Overall
(n = 1,266)Antihypertensive Treatment P
ValueaYes
(n = 1,057)No
(n = 209)Sociodemographic data Female, n (%) 874 (69) 728 (69) 146 (70) .72 Age, years (SD) 82.4 (5) 82.5 (5) 82.3 (5) .59 Primary school only, n (%) 656 (52) 541 (51) 115 (55) .33 Low incomeb, n (%) 197 (16) 166 (16) 31 (15) .72 Residential home, n (%) 101 (8) 83 (8) 18 (9) .72 Systolic blood pressure, n (%) <130 mm Hg 237 (19) 197 (19) 40 (19) 130-150 mm Hg 613 (48) 493 (47) 120 (57) .004 >150 mm Hg 416 (33) 367 (35) 49 (23) Comorbidity, n (%) CVDc 511 (40) 503 (48) 8 (4) <.001 Diabetes mellitus 274 (22) 242 (23) 32 (15) .013 Depression 182 (14) 148 (14) 34 (16) .42 Cancer 159 (13) 134 (13) 25 (12) .75 Complex health problemsd 674 (53) 571 (54) 103 (49) .23 Baseline function, mean (SD) MMSEe score 27.2 (3.1) 27.2 (3.0) 27.0 (3.5) .31 GARSf score 33.0 (11.5) 33.3 (11.4) 31.2 (11.7) .019 EQ-5D-3Lg index values 0.70 (0.27) 0.66 (0.27) 0.71 (0.26) .031 CVD = cardiovascular disease; EUR = euro; GARS = Groningen Activities Restriction Scale; MMSE = Mini-Mental State Examination.
↵a P value from χ2 test for categorical data and t test for normally distributed continuous data.
↵b Defined as state pension only (~EUR 750 monthly).
↵c CVD included myocardial infarction, angina pectoris, intermittent claudication, other ischemic heart disease, stroke, transient ischemic attack, and heart failure.
↵d Defined as patients having problems in 3 or more of 4 domains (functional, somatic, mental, social).
↵e MMSE on a scale of 0 to 30 points (higher scores indicate better cognitive function).
↵f GARS; score ranges from 18 to 72 (higher scores indicate greater disability).
↵g Quality of life (EQ-5D-3L index values; full health has a value of 1, dead a value of 0).
- Table 2
Associations Between Baseline Systolic Blood Pressure and Antihypertensive Treatment With Change in Cognitive/Daily Function and Quality of Life After 1-year Follow-Up (n = 1,266)
Characteristic Antihypertensive Treatment Yes (n = 1,057) No (n = 209) No. Change (95% CI) P Value P Trend No. Change (95% CI) P Value P Trend Cognitive function <130 mm Hg 194 Reference … <.001 40 Reference … .07 130-150 mm Hg 485 0.71 (0.20-1.22) .007 … 118 1.04 (−0.04 to 2.12) .06 … >150 mm Hg 362 1.01 (0.47-1.55) <.001 … 48 1.22 (−0.03 to 2.47) .06 … Daily function <130 mm Hg 191 Reference … .47 40 Reference … .70 130-150 mm Hg 480 −0.08 (−1.11 to 0.96) .88 … 114 −1.73 (−4.54 to 1.10) .42 … >150 mm Hg 359 −0.37 (−1.47 to 0.74) .51 … 48 −0.75 (−4.02 to 2.52) .65 … Quality of life <130 mm Hg 193 Reference … .17 39 Reference … .14 130-150 mm Hg 484 0 (−0.04 to 0.04) .98 … 118 −0.06 (−0.14 to 0.02) .13 … >150 mm Hg 364 0.03 (−0.02 to 0.07) .24 … 49 −0.07 (−0.16 to 0.02) .12 … GARS = Groningen Activities Restriction Scale; MMSE = Mini-Mental State Examination; Reference = <130 mm Hg; SBP = systolic blood pressure.
Note: Multivariable mixed-effects regression model adjusted for age, sex, baseline MMSE/GARS/EQ-5D-3L and accounting for clustering within family physicians.
Reading example: Patients undergoing antihypertensive treatment and with a baseline SBP >150 mm Hg had 1.01 points MMSE (95% CI, 0.47-1.55 points) less cognitive decline compared to patients undergoing antihypertensive therapy and with a baseline SBP <130 mm Hg (Reference).
Characteristic Antihypertensive Treatment Yes (n = 571) No (n = 103) No. Change (95% CI) P Value P Trend No. Change (95% CI) P Value P Trend Cognitive function <130 mm Hg 117 Reference … < .001 20 Reference … .13 130-150 mm Hg 258 0.99 (0.32-1.66) .004 … 60 1.90 (0.05-3.75) .044 … >150 mm Hg 189 1.39 (0.68-2.11) <.001 … 22 1.78 (−0.42 to 3.98) .11 … Daily function <130 mm Hg 115 Reference … .59 20 Reference … .65 130-150 mm Hg 254 −0.18 (−1.57 to 1.20) .79 … 57 −2.02 (−6.14 to 2.10) .34 … >150 mm Hg 188 −0.40 (−1.88 to 1.09) .60 … 22 −1.20 (−6.11 to 3.72) .63 … Quality of life <130 mm Hg 117 Reference … .61 19 Reference … .19 130-150 mm Hg 257 −0.03 (−0.08 to 0.03) .21 … 60 −0.11 (−0.23 to 0.01) .08 … >150 mm Hg 190 0.01 (−0.05 to 0.07) .99 … 22 −0.10 (−0.24 to 0.04) .16 … GARS = Groningen Activities Restriction Scale; MMSE = Mini-Mental State Examination; Reference = <130 mm Hg; SBP = systolic blood pressure.
Note: Associations of baseline systolic blood pressure and antihypertensive treatment with change in cognitive/daily function and quality of life after 1-year follow-up (n = 1,266). Multivariable mixed-effects regression model adjusted for sex, age, baseline MMSE/GARS/EQ-5D-3L, and accounting for clustering within family physicians.
Reading example: Patients undergoing antihypertensive treatment and with a baseline SBP >150 mm Hg had 1.39 points MMSE (95% CI, 0.68-2.11 points) less cognitive decline compared to patients undergoing antihypertensive therapy and with a baseline SBP <130 mm Hg (Reference).
Supplemental Appendixes
Supplemental Appendixes
Files in this Data Supplement:
- Supplemental data: Appendixes - PDF file
The Article in Brief
Systolic Blood Pressure and Cognitive Decline in Older Adults With Hypertension
Jacobijn Gussekloo , and colleagues
Background Studies of hypertension tend to exclude patients with complex health problems and lack generalizability. This study set out to determine if, for older patients being treated for hypertension, both with and without complex health problems, systolic blood pressure is linked to one-year changes in cognitive/daily functioning or quality of life.
What This Study Found In people aged 75 years and older who are being treated for hypertension, systolic blood pressure less than 130 mm Hg is associated with additional cognitive decline, particularly in individuals with complex health problems. Researchers in the Netherlands analyzed data for 1,266 participants in the Integrated Systematic Care for Older Persons study. Patients were stratified by systolic blood pressure in the year before baseline, and change was evaluated from baseline to one-year follow-up in outcome measures evaluating cognitive function (the Mini-Mental State Examination), activities of daily living, and quality of life. For participants being treated for hypertension, there was a clear trend across categories of systolic blood pressure: with lower systolic blood pressure, cognitive declined worsened at one-year follow-up. For participants being treated for hypertension and with systolic blood pressure less than 130 mm Hg, cognitive decline in one year averaged 0.90 points on the Mini-Mental State Examination compared to 0.14 points for those with systolic blood pressure greater than 150 mm Hg, a 0.76-point less decline. The results were similar for participants with complex health problems (n=674). Compared to the reference group (systolic blood pressure less than 130 mm Hg), participants showed less cognitive decline after one year by 0.99 points on the Mini-Mental State Examination when systolic blood pressure was 130-150 mm Hg and by 1.39 points when systolic blood pressure was greater than 150 mm Hg. Daily functioning and quality of life were the same across the strata of systolic blood pressure and antihypertensive treatment.
Implications
- The authors call for more studies to determine if there is a causal relationship between systolic blood pressure and cognitive decline and to understand the mechanism of the association observed. Until the results of new trials are available, they state, clinicians must decide on the appropriate treatment for hypertension in older patients.
Annals Journal Club
Mar/Apr 2019: Antihypertensive Treatment, Low Systolic Blood Pressure, and Cognitive Decline
Kathryn Rooney, BA, Rush Medical College, and Michael E. Johansen, MD, MS, Associate Editor
The Annals of Family Medicine encourages readers to develop a learning community to improve health care and health through enhanced primary care. Participate by conducting a RADICAL journal club. RADICAL stands for Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. We encourage diverse participants to think critically about important issues affecting primary care and act on those discussions.1
HOW IT WORKS
In each issue, the Annals selects an article and provides discussion tips and questions. Take a RADICAL approach to these materials and post a summary of your conversation in our online discussion. (Open the article and click on "TRACK Discussion/ Submit a comment.") Discussion questions and information are online at: http://www.AnnFamMed.org/site/AJC/.
CURRENT SELECTION
Article for Discussion
Streit S, Poortvliet RKE, den Elzen WPJ, Blom JW, Gussekloo J. Systolic blood pressure and cognitive decline in older adults with hypertension. Ann Fam Med. 2019;17(2):100-107.
Discussion Tips
Prominent guidelines for hypertension management recommend a goal systolic blood pressure of <130 mm Hg for noninstitutionalized, ambulatory adults aged ≥65 years. The current study uses a cohort design to examine whether stricter blood pressure control is associated with changes in memory. We recommend that participants read both this article and the recently published analysis of the randomized controlled SPRINT trial2 to compare and contrast the studies and findings.
Discussion Questions
- What question is asked by the study and why does it matter?
- What is the difference between an observational study and a randomized study? Why is this important? Are observational studies able to show causation?3
- What is the difference between categorical, dichotomous, ordinal, and continuous variables? Why does this matter?4
- How is change from baseline measured in this study? Is this an appropriate way to measure change from baseline measures?5
- How appropriate is the observational, prospective cohort study design for answering this question?
- To what degree can the findings be accounted for by:
- How patients were selected, excluded, or lost to follow-up?
- How patients were stratified?
- How confounding variables were accounted for?
- The amount of time allotted for follow-up?
- How the main outcome variables were measured?
- What are the main findings of this study?
- How relevant are the outcome measures (Mini-Mental State Examination, Groningen Activities Restriction Scale, and EQ-5D-3L) for capturing the outcomes of interest (ie, memory loss)?
- How does this study compare to the analysis of the SPRINT trial and cognitive impairment?3 Could both of these trials be correct?
- How might this study change your practice?
- What future research would be most valuable to pursue?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals Journal Club: It's time to get RADICAL. Ann Fam Med. 2006;4(3):196-197.
- Williamson JD, Pajewski NM, Auchus AP, et al; SPRINT MIND Investigators for the SPRINT Research Group. Effect of intensive vs standard blood pressure control on probable dementia: a randomized clinical trial. JAMA. 2019;321(6):553-561.
- Pearl J, MacKenzie D. The Book of Why: The New Science of Cause and Effect. New York, NY: Basic Books, Inc; 2018.
- Altman DG, Royston P. The cost of dichotomising continuous variables. BMJ. 2006;332(7549):1080.
- How should change be measured? http://biostat.mc.vanderbilt.edu/wiki/Main/MeasureChange. Published Jan 4, 2017. Accessed Feb 22, 2019.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Hypertension control and its relationship with cognitive impairment among adults aged 45 to 80 in China
- White matter hyperintensities may be an early marker for age-related cognitive decline
- Home Blood Pressure Monitoring in Cases of Clinical Uncertainty to Differentiate Appropriate Inaction From Therapeutic Inertia
- In This Issue: Minding the Gaps