
Article Figures & Data
Figures
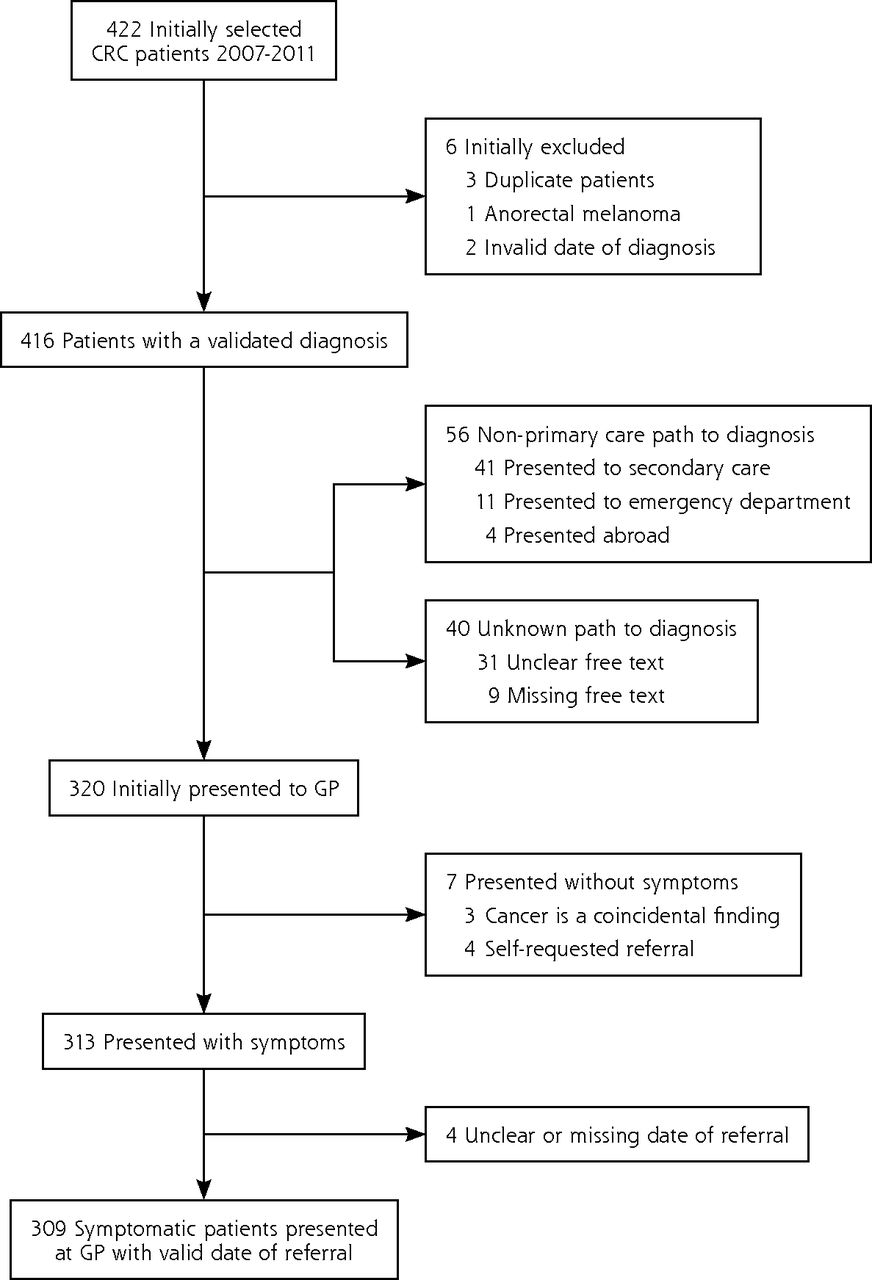
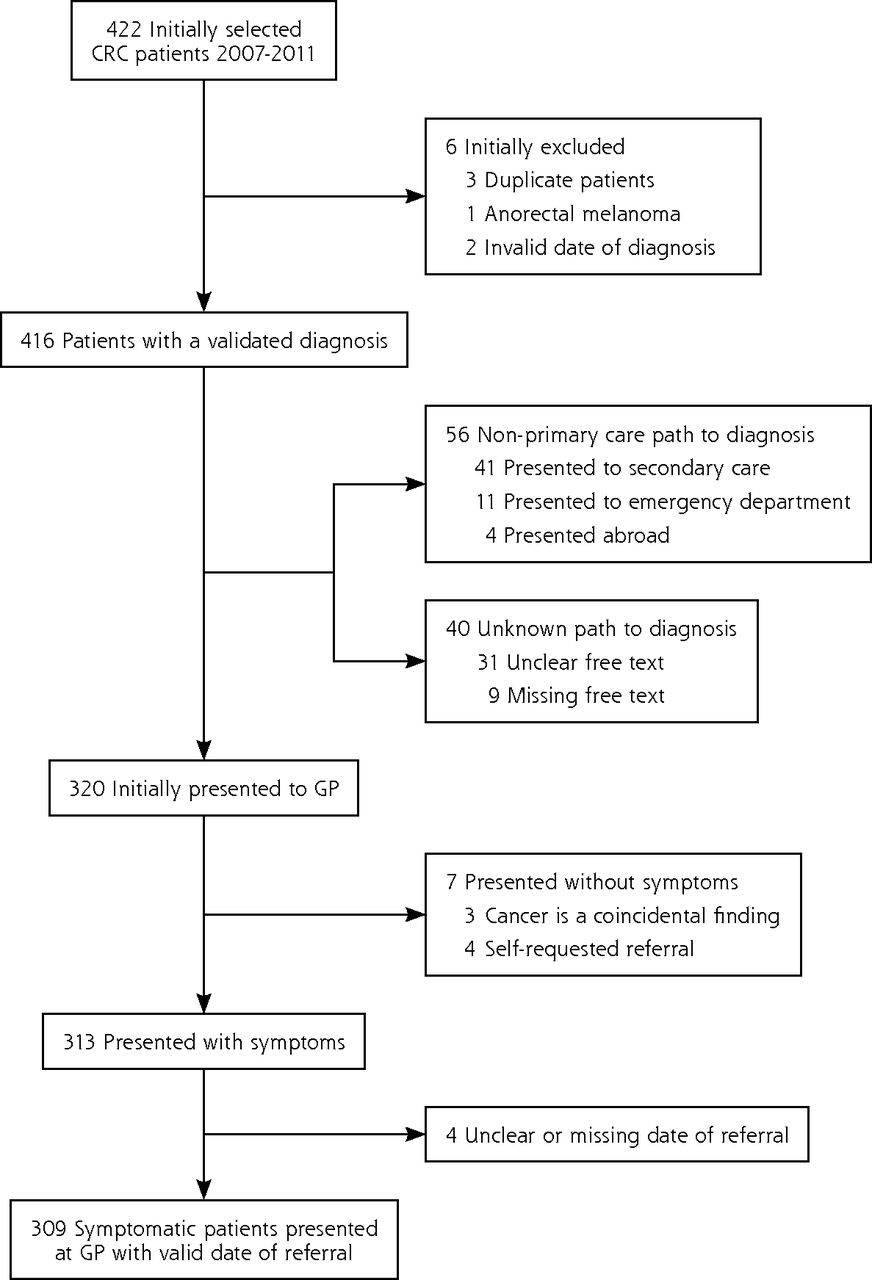
- Figure 1
Flowchart for CRC patient selection.
CRC = colorectal cancer; GP = general practitioner.
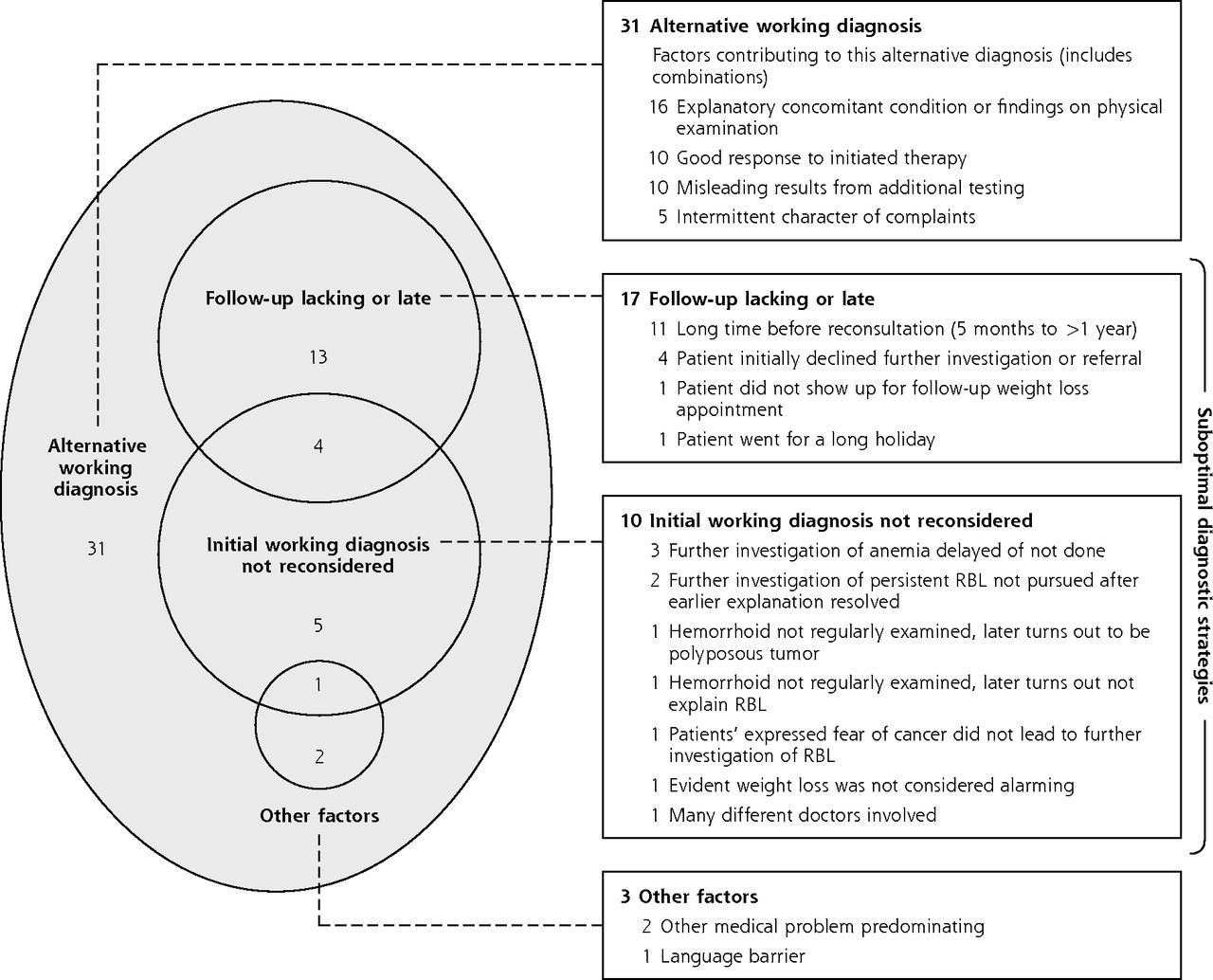
- Figure 2
Factors contributing to longest duration (≥219 days) for symptomatic CRC patients.a
CRC = colorectal cancer; RBL = rectal blood loss.
aThe Venn diagram circles do not illustrate the relative sizes of groups.

Tables
Characteristic No. (%) TNM stage at diagnosis 0 1 (0.3) I 41 (13.3) II 83 (26.9) III 114 (36.9) IV 65 (21.0) Unknown 5 (1.6) Tumor location Proximal colon 90 (29.1) Distal colon 20 (6.5) (Recto)sigmoid 99 (32.0) Rectal 97 (31.4) Colon unspecified 3 (1.0) CRC = colorectal cancer; GP = general practitioner; TNM = tumor, nodes, metastases.
- Table 2
Patient and Presentation Characteristics of Symptomatic CRC Patients, Duration of Primary Care Interval, and Log-Binomial Regression Analysis for 75th Percentile (N = 309)
Characteristic No. Duration, d, Median (IQR) P Valuea P90b Univariable RR (95% CI) Multivariable RR (95% CI) Age, y ≤50 35 34 (1-233) 491 1.5 (0.8-3.0) 51-60 47 3 (1-15) 408 0.6 (0.3-1.4) 61-70 100 14 (1-47) 94 0.8 (0.4-1.4) 71-80 91 6 (1-61) 204 0.9 (0.5-1.7) 81-90 36 8 (1-68) .154 150 1 (ref) Sex Male 155 4 (1-47) 101 1 (ref) 1 (ref) Female 154 13 (1-78) .004 321 1.6 (1.1-2.4) 1.4 (0.9-2.1) SES 2010c Low 81 12 (1-72) 240 1 (ref) Medium-low 79 9 (1-63) 239 0.9 (0.5-1.5) Medium-high 73 7 (1-51) 118 0.7 (0.4-1.3) High 76 6 (1-47) .551 223 0.7 (0.4-1.2) Registered comorbidityd Chronic somatic No 62 5 (1-48) 326 1 (ref) Yes 247 10 (1-61) .317 198 1.1 (0.7-1.9) ≥2 181 9 (1-58) 203 1.1 (0.6-1.8) ≥4 70 8 (1-43) 98 0.9 (0.5-1.7) Gastrointestinal No 256 8 (1-63) 219 1 (ref) Yes 53 15 (2-48) .622 119 0.7 (0.4-1.3) Psychiatric No 290 8 (1-58) 204 1 (ref) Yes 19 22 (2-84) .203 538 1.1 (0.5-2.3) Registered family history of CRCe Not registered 267 11 (1-65) 233 1 (ref) Negative 30 1 (1-13) 87 0.5 (0.2-1.3) Positive 12 2 (1-34) .003 87 0.3 (0.1-2.0) Consultation frequency for year prior to first CRC consultation ≤2 56 2 (1-29) 117 1 (ref) 3-11 188 11 (1-64) 235 1.4 (0.8-2.5) ≥12 65 12 (1-54) .093 120 1.2 (0.6-2.3) History of malignancy No 267 7 (1-50) 219 1 (ref) 1 (ref) Yes 42 18 (2-84) .101 178 1.7 (1.1-2.6) 1.5 (0.9-2.2) Main registered symptom at first CRC consultationf Alarm GI symptom(s) 168 2 (1-28) 123 1 (ref) 1 (ref) Nonalarm GI symptom(s) 113 26 (5-87) 257 1.9 (1.2-2.8) 1.7 (1.1-2.6) Other symptom(s) 28 13 (2-43) .000 273 0.9 (0.4-2.2) 0.9 (0.4-2.1) Hemorrhoids at physical examinationg No 298 8 (1-54) 219 1 (ref) Yes 11 69 (1-115) .192 213 2.3 (1.3-4.1) TNM stage at diagnosis 0 1 87 … … I 41 2 (1-42) 83 1 (ref) II 83 7 (1-48) 213 1.1 (0.5-2.3) III 114 7 (1-48) 159 1.1 (0.5-2.2) IV 65 23 (3-92) 502 1.9 (0.9-3.8) Unknown 5 5 (1-246) .013 … … CRC = colorectal cancer; GI = gastrointestinal; GP = general practitioner; IPC = primary care interval; IQR = interquartile range; P75 = 75th percentile value of the duration distribution; P90 = 90th percentile value of the duration distribution; RR = relative risk; SES = socioeconomic status score; TNM = tumor, nodes, metastases.
↵a P values based on Mann-Whitney U tests for variables with 2 categories and Kruskall-Wallis tests for variables with 3 or more categories.
↵b P90 value = 90th percentile value of the duration distribution; that is the IPC duration time in days where 90% of the population was below and 10% above.
↵c Socioeconomic status scores 2010 were retrieved from publicly available data from the Netherlands Institute for Social Research.16 Lowest SES score was defined as: SES score of <1 SD than the Dutch mean of 2010, Medium-low: 1 SD to mean SES score, Medium-high: mean SES score to +1 SD and Highest: > +1 SD higher than Dutch mean.
↵d Chronic somatic comorbidities were defined according to O’Halloran et al.17 Gastrointestinal comorbidities were all relevant GI-related registered comorbidities or conditions in either episode list or mentioned during GP consultations: irritable bowel syndrome, reflux disease, esophagitis, dyspepsia, abdominal pain, peptic ulcer, hiatus or abdominal hernia, benign GI neoplasms/polyps, constipation, chronic diarrhea, cholelithiasis, diverticulosis, anal fissures. Psychiatric comorbidities were all chronic psychiatric comorbidities according to O’Halloran et al.17
↵e Registered occurrence of colorectal cancer in a first degree family member.
↵F Alarm symptoms for colorectal cancer were defined as rectal blood loss, unintended weight loss, anemia, and a palpable tumor. GI symptoms include all GI-related, nonalarming symptoms. Other symptoms are all remaining, nonalarming, non-GI symptoms.
↵g Multivariable model excludes this factor due to low patient numbers.
Supplemental Appendix
Supplemental appendix
Files in this Data Supplement:
- Supplemental data: Appendix - PDF file
The Article in Brief
Potential for Reducing Time to Referral for Colorectal Cancer Patients in Primary Care
Charles W. Helsper , and colleagues
Background Delay in referral to specialty care for patients who have symptoms of colorectal cancer may lead to poor health outcomes. While the current median duration from first consultation with cancer related complaints to referrals is approximately one week for colorectal cancer patients in the UK and the Netherlands, time to referral varies strongly. Some cases document months and even years before referral, and explanations for suboptimal referral is often incomplete or oversimplified.
What This Study Found A retrospective cohort study in the Netherlands reviewed the time to specialty referral for a group of 309 patients with colorectal cancer who initially presented with symptoms to their primary care doctor. A multivariable analysis narrowed down the factors associated with delays in referrals to specialty care. Those who initially presented with red flag symptoms, such as rectal bleeding or unintended weight loss, experienced shorter wait time than those who presented with non-alarming gastrointestinal symptoms. Univariable analysis showed that female patients and patients without a registered family history of the disease were also more likely to have a longer wait period. Of the 10% of patients with the longest wait times for referral to specialty care all patients had received an alternative initial diagnosis from their primary care physicians. These patients usually presented with conditions that obscured concern for colorectal cancer, such as hemorrhoids, fissures and inflammatory bowel disease. Initial diagnoses were not always reconsidered when complaints persisted and follow-up consultations were sometimes omitted.
Implications
- This study points to a relationship between long time to referral of colorectal cancer in primary care and low cancer suspicion. There is potential for reducing longest times to referral of colorectal cancer patients in primary care by earlier reconsideration of the initial hypothesis and implementing strict follow-up consultations.
Visual Abstract
Files in this Data Supplement:
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Exploring why European primary care physicians sometimes do not think of, or act on, a possible cancer diagnosis. A qualitative study
- Measurement of clinical delay intervals among younger adults with colorectal cancer using health administrative data: a population-based analysis
- Role of primary care physician factors on diagnostic testing and referral decisions for symptoms of possible cancer: a systematic review
- Factors affecting the decision to investigate older adults with potential cancer symptoms: a systematic review
- Multilevel Approaches to Reducing Diagnostic and Treatment Delay in Colorectal Cancer