
Abstract
PURPOSE Whereas communication among health care professionals plays an important role in providing the best quality of care for primary care patients, little evidence exists regarding how professional communication contributes to job satisfaction among health care providers, including physicians and clinical staff, in primary care clinics. This study evaluates the extent to which professional communication networks contribute to job satisfaction among health care professionals in primary care clinics.
METHODS A total of 143 health care professionals, including physicians and clinical staff, at 5 US primary care clinics participated in a cross-sectional survey on their communication connections regarding patient care with other care team members and their job satisfaction. Social network analysis calculated core-periphery measures to identify individuals located in a dense cohesive core and in a sparse, loosely connected periphery in the communication network. Generalized linear mixed modeling related core-periphery position of clinic employees in the communication network to job satisfaction, after adjusting for job title, sex, number of years working at the clinic, and percent full-time employment.
RESULTS Average job satisfaction was 5.8 on a scale of 1 to 7. Generalized linear mixed modeling showed that individuals who were in the core of the communication network had significantly greater job satisfaction than those who were on the periphery. Female physicians had lesser overall job satisfaction than other clinic employees.
CONCLUSIONS Interventions targeting professional communication networks might improve health care employee job satisfaction at primary care clinics.
INTRODUCTION
Job satisfaction among primary care professionals, including physicians and clinical staff, can have a significant effect on patient satisfaction with care and patient care quality.1,2 Close to 68% of family physicians and 73% of general internists report job dissatisfaction.3 Less than 40% of family and internal medicine physicians indicated satisfaction with work-life balance in 2014.4 Increasing regulations, electronic health records (EHRs), hectic pace, long hours, and increasing workload contribute to lower job satisfaction among health care professionals.5 In addition, worse job satisfaction in primary care is closely related to professional burnout characterized by loss of emotional, mental, and physical energy in the context of job-related stress and could lead to reduced patient outcomes.1,6–8 Whereas clinicians’ job satisfaction is recognized as an important goal to aim for, there is a gap in understanding the ways in which team care delivery could enhance clinicians’ job satisfaction in primary care.
Notably, little is known about how professional communication in primary care teams contributes to job satisfaction among health care professionals including physicians and clinical staff. Primary care team members rely on team communication as a sensemaking process to assign meaning to experience and to collaborate during health care delivery.9 Team communication helps teams form shared understanding of clinical situations under the conditions of interdependency and time constraints that are inherent to primary care practices. Effective team communication allows health care practitioners to develop coordination, which is the capacity to predict, anticipate, and respond to one another in high-stress and restricted-time environments such as primary care and, in turn, may increase job satisfaction.10 Flexible professional communication between team members that is not constricted by authority gradients could enhance professional job satisfaction because it leverages the strengths of all health care practitioners.11–14 Ineffective professional communication might hinder job satisfaction and severely limit sensemaking, coordination, and collaboration if there are clinic hierarchies for communication and/or if there are bottlenecks in clinic communication flow.15,16 Poor team communication among primary care professionals might lead to worse job satisfaction if there is a dual organization, for example, in which some team members are isolated from interacting with the rest of the clinic staff.16 To improve job satisfaction among primary care professionals, including physicians and clinical staff, there is a need to place analytic focus on how team professional communication flow relates to job satisfaction among primary care practitioners.
To fill this gap in the link between team professional communication flow and job satisfaction among primary care practitioners, we aimed to investigate the following research question: How does professional communication flow in primary care clinics relate to job satisfaction among health care professionals?
METHODS
Data Source and Study Procedures
We obtained study data from a sample of 5 primary care clinics within a large health care delivery system associated with an academic institution in southern Wisconsin. A total of 8 primary care clinics were invited, and 5 agreed to participate. Study sites were selected on the basis of consultation with leadership from the health care system. Invited sites were non-residency–based primary care clinics that were not currently involved in research or quality improvement initiatives. Reasons for refusal to participate in the study included recent staff turnover and lack of time. The 5 participating clinics were urban (2), suburban (2), and rural (1). The clinics had from 3 to 11 primary care practitioners (PCPs). The Institutional Review Board of the University of Wisconsin approved the study.
The first author introduced the study procedures and provided study consent forms at an all-staff clinic meeting at each participating clinic. All physicians (doctors of medicine [MDs], doctors of osteopathic medicine [DOs]), physician assistants (PAs), nurse practitioners (NPs), registered nurses (RNs), medical assistants (MAs), licensed practical nurses (LPNs), laboratory technicians, radiology technicians, clinic managers, medical receptionists, and other patient care professionals were then invited to schedule a 30-minute face-to-face structured survey interview. Eligibility criteria included age 18 years or older, ability to read and understand English, and employment at the study site in a patient care or patient interaction capacity. Participants received $10 for completing the study survey and were entered into a lottery drawing for $100. In addition, the research team donated $200 to a local outreach effort of the clinic’s choice to clinics with 90% participation. A total of 97% (143 of 147 invited) of eligible subjects took part in the study. Using a clinic staff roster as an aid for memory recall, study participants were asked to identify with whom at their clinic and how frequently they interacted face to face and via EHRs.
Face-to-Face and Electronic Communication Measures
To measure face-to-face communication flow, we asked participants, “Consider the PAST 6 MONTHS. On a typical day in clinic, how often do you communicate face-to-face about patient care with other clinicians and clinic staff?” To measure electronic communication flow, we asked, “Consider the PAST 6 MONTHS. On a typical day in clinic, how often do you communicate about patient care with other clinicians and clinic staff via electronic medical records?” Responses to both questions were ordered from 0 (less than 1-2 times per month) to 5 (multiple times per day). For each clinic and for both face-to-face and electronic communication, a dichotomous (0/1) participant-by-participant communication matrix was created on the basis of the responses to the clinic communication survey. A communication connection between 2 health care practitioners was coded as present (1) if frequency of communication was reported as daily or multiple times per day, or absent (0) otherwise.
Core-Periphery Communication Network Measure
We used social network analysis and the Borgatti-Everett (B-E) algorithm17 to detect the core-periphery structure of the face-to-face and electronic communication networks for each clinic. The core-periphery model is based on the concept of dividing the network into 2 distinct sets of nodes. The first set is a cohesive core of individuals who are highly interconnected (ideally, every member of the core is connected to every other member of the core). The second set comprises peripheral individuals who are loosely connected to the core network members and have few connections to each other (ideally, no connection exists between any 2 peripheral members). Peripheral members can only connect to each other by first connecting to a core member. The B-E algorithm iteratively partitions the network members into core and periphery groups and calculates the correlation between the observed connections within the core and the periphery and an idealized core and periphery (one with a complete set of connections within the core and an absent set of connections within the periphery). By maximizing the correlation of the observed network with the idealized core-periphery structure, the B-E algorithm defines each member of the communication network to be either a core member or a periphery member. A correlation of ≥0.8 is generally accepted as an indication of strong core-periphery structure. As described by Borgatti and Everett,17 there is no statistical test for significance of the core-periphery delineation. See the Supplemental Appendix (http://www.AnnFamMed.org/content/17/5/428/suppl/DC1/) for the mathematical derivation of the B-E algorithm.
The individuals in the network core have densely intertwined connections that can be used interchangeably and that can substitute for each other to send information. In other words, information can flow quickly by following multiple possible pathways in the core but not in the periphery. Individuals in the periphery have fewer and longer connections to pass information, given that they need to rely on their links to core connections to exchange information with other peripheral individuals. Individuals in the network core are more efficient at passing information than those in the periphery.
Job Satisfaction Measures
We measured job satisfaction with the Warr-Cook-Wall (WCW) job satisfaction survey, which measures overall job satisfaction and satisfaction with regard to 9 aspects of work (amount of responsibility, freedom of working method, amount of variety in work, colleagues and fellow workers, physical working conditions, opportunity to use abilities, income, recognition for work, and hours of work).18 Each item is rated on a 7-point Likert scale (1 = extremely dissatisfied, 7 = extremely satisfied).
Individual and Demographic Characteristics
Study participants completed survey questions regarding job title, number of years working at the clinic, percent full-time employment (FTE), and sex.
Statistical Analysis
Multivariate analyses using generalized linear mixed modeling (GLMM)19 tested the association between an individual’s core-periphery network position in the clinic face-to-face and electronic communication networks (core or periphery) and the individual’s job satisfaction after adjusting for clinic-level fixed effects, job title, sex, number of years working at the clinic, and percent FTE. The GLMM model used a 2-level structure with clinic employees nested by clinic. Separate GLMM models were constructed for each of the 9 aspects of the WCW job satisfaction survey.
We calculated correlations between physician/NP job satisfaction and the job satisfaction of clinic members to whom they were directly connected via face-to-face or electronic communication. For each study participant, we calculated the mean job satisfaction of the clinic members who had either a face-to-face or electronic communication tie to that clinician. The resulting mean values were then correlated with the clinician’s job satisfaction using the Pearson correlation coefficient. We used UCINET 6 to construct networks and obtain social network analysis measurements20 and HLM 7 (STATCON GmbH) to construct GLMM models.
RESULTS
This study surveyed 143 health care professionals, including physicians and clinical staff, from 5 primary care clinics (Table 1). The study sample consisted of 24 physicians, 7 NPs, 27 RNs, 7 LPNs, 21 MAs, 32 medical receptionists, 12 laboratory technicians, 8 radiology technicians, and 5 clinic managers. Respondents were 91.6% female, in line with US Census Bureau data indicating that 91% of all nurses, NPs, and LPNs, and 97% of all medical receptionists, are female.21 A total of 18.2% of the participants had worked at their practice for ≤1 year, and just less than one-third worked <80% FTE time.
Health Care Professional Job Satisfaction by Participant Attributes (n = 143)
Overall, 82 (57%) respondents were located in the face-to-face communication core of their respective clinics, and 83 (58%) were located in the electronic communication core of their clinics. The face-to-face communication core comprised primarily RNs, MAs, and receptionists. Interestingly, only 6 (19%) of the physicians and NPs were in the face-to-face communication core. However, 20 (65%) of the physicians and NPs were in the electronic communication core. Less than half (48%) of the MAs were in the electronic communication core.
As shown in Table 1, overall job satisfaction (presented as mean [SD]) varied by job title and percent FTE. The lowest job satisfaction was among female physicians (5.1 [1.5]) in contrast to male physicians (6.1 [0.7]), clinic managers (6.2 [0.4]), LPNs (6.3 [0.8]), and radiology technicians (6.4 [0.9]), who had the greatest job satisfaction by job title. With regard to part-time employment, employees who worked 70% to <80% time had the lowest job satisfaction (5.0 [1.7]), whereas those who worked 90% to <100% time had the greatest job satisfaction (6.3 [0.8]).
Table 2 shows unadjusted mean responses to the 9 different aspects of job satisfaction on the WCW job satisfaction survey by job title. Physicians, NPs, and clinic managers had significantly lower satisfaction with hours of work. Female physicians also had significantly lower satisfaction with the amount of responsibility given to them.
Components of Warr-Cook-Wall Job Satisfaction Scale by Job Title (n = 143)
Table 3 presents the results of the GLMM models for overall WCW survey score as well as different aspects of job satisfaction after adjusting for membership in the face-to-face communication core or electronic communication core. Health care professionals who were in the face-to-face communication network core had greater overall job satisfaction (β = 0.33; P <.05), greater satisfaction with regard to the amount of responsibility they were given (β = 0.73; P <.01), and greater satisfaction with the opportunity to use their abilities (β = 0.79; P <.01). Health care professionals who were in the electronic communication network core did not have significantly greater overall job satisfaction (β = 0.29; P = .145).
Multilevel Models of Job Satisfaction Aspects
After adjusting for confounders, female physicians differed from the overall trends across job categories with regard to face-to-face communication core membership and job satisfaction. For female physicians, face-to-face communication core membership was associated with lower, albeit not statistically significant, overall job satisfaction (mean 4.3 for core member vs mean 5.3 for core nonmember; P = .351). By comparison, clinic professionals other than female physicians had greater overall job satisfaction when in the face-to-face communication core (mean 6.0 for core member vs mean 5.7 for core nonmember; P = .031). However, for female physicians, electronic communication core membership trended toward greater overall job satisfaction (mean 5.5 for core member vs mean 4.5 for core nonmember; P = .105). Female physicians were satisfied with their variety of work, the opportunity to use their abilities, and income but dissatisfied with work hours and the job overall. In addition, there was a significant correlation between female physicians’ satisfaction with work hours and their directly connected staff’s job satisfaction with the greater amount of responsibility given to them (r = 0.446; P = .012).
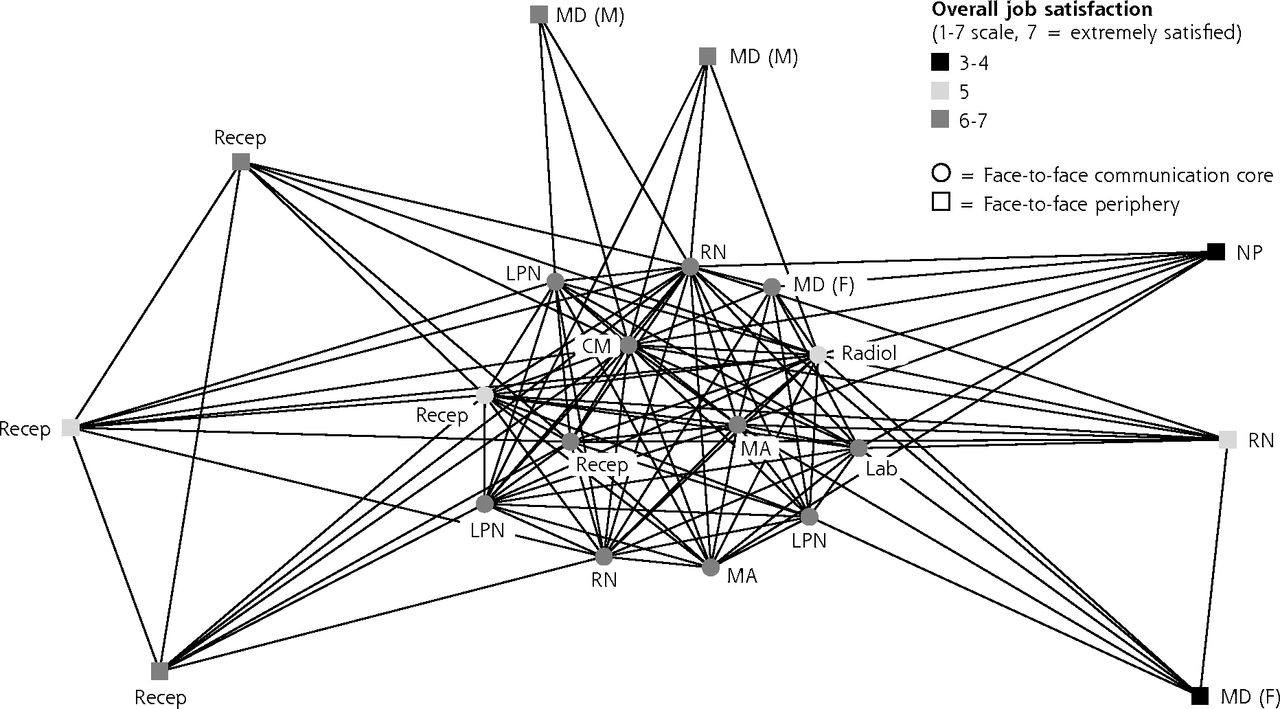
Figure 1 represents the overall job satisfaction and face-to-face communication network of the health care professionals at 1 of the 5 study clinics. Job satisfaction was lower among clinic members who were on the periphery of the clinic communication network. In particular, 1 female physician and 1 NP with the lowest job satisfaction were connected to very few members of the face-to-face communication core of the network.
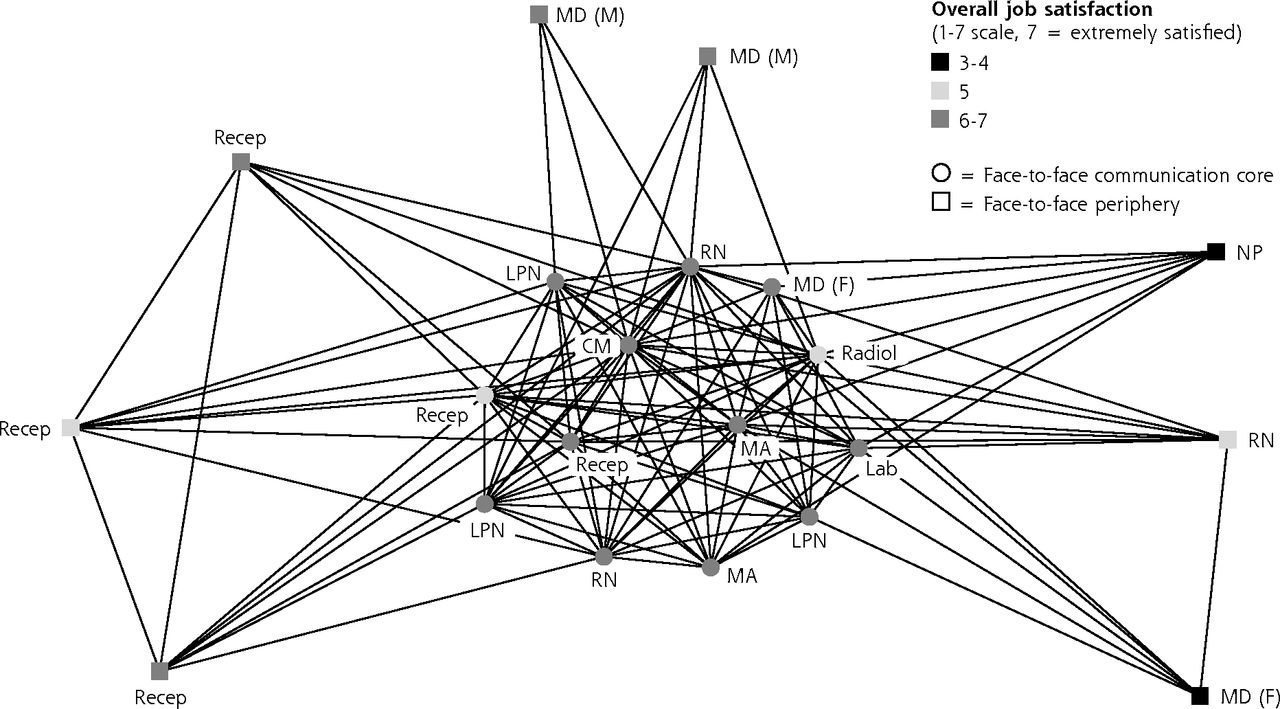
Core-periphery communication position and job satisfaction in primary care.
CM = clinic manager; LPN = licensed practical nurse; MA = medical assistant; NP = nurse practitioner; Phys(F) = physician, female; Phys(M) = physician, male; Radiol = radiology technician; Recep = medical receptionist; RN = registered nurse.
DISCUSSION
We evaluated the associations between professional team communication flow and job satisfaction among primary care professionals. Overall, our findings showed that variations in team communication flow are associated with statistically significant variations in job satisfaction among team members. Contrary to electronic communication core membership, being included in the highly interconnected core of face-to-face communication increased overall job satisfaction with regard to the amount of responsibility given and greater satisfaction with the opportunity to use one’s abilities for all clinical professionals, with the exception of female physicians.
Team members who are part of a highly interconnected face-to-face communication core might develop team cognition, which is cognitive information processing on the part of the team (eg, team-level problem solving, sensemaking). Team cognition (ie, team-shared understanding of the capabilities of each team member, who is good at what, who should be assigned what at what time) allows a team to be more than the sum of its parts. It affords teams flexibility and adaptability and enables teammates to relate to each other and to newly emerging information in the process of task performance. The link between team cognition and team performance outcomes is well established in the literature. In view of better team performance, team members might experience better job satisfaction if they experience constructive working relationships and engage in shared team care delivery. Future studies might wish to further explore what characteristics of the face-to-face communication core contribute to patient outcomes.
Interestingly, in contrast to male physicians, female physicians were satisfied with their variety of work, the opportunity to use their abilities, and income, but they were dissatisfied with work hours and with their job overall, indicating a less than desirable work-life balance. Notably, female physicians who were more satisfied with their work hours had team members who were more satisfied with the amount of responsibility given to them. Furthermore, female physicians in the face-to-face communication core were less satisfied with their job overall. It is possible that their presence in the face-to-face core might introduce an authority gradient and might create bottlenecks in team communication flow when information has to go through female physicians. This might create more workload and less job satisfaction for female physicians when responsibilities are not equally shared among all team members. Sharing of care responsibilities with other team members might allow female physicians to increase job satisfaction and work-life balance. Future research might wish to further explore sex differences in job satisfaction in relation to the distribution of care responsibilities among team members.
Our present results have important implications for primary care stakeholders. To increase job satisfaction among primary care professionals, it might be necessary to look beyond individual practitioners to consider how to support frequent daily communication among all team members and how to allow all team members to be interconnected in their face-to-face communication and to share in team-based care. Adoption of daily team huddles or structured team communication in primary care teams might improve job satisfaction. The American Medical Association has developed a STEPS Forward, Implementing Team Huddle intervention to boost health team outcomes and team climate by enhancing team communication skills.22,23 Future studies might further explore how to foster team communication that would reduce core-periphery structures in team face-to-face communication rather than solely focusing on the individual-level aspects contributing to job satisfaction.
The present study showed that job satisfaction is associated with team-level communication, which reflects work environment and management practices in primary care clinics. Interventions targeting cohesion, shared trust, shared values, and emphasis on team communication engaging all teammates might be a pathway to increase job satisfaction in the primary care workforce. Our results come to light in view of recent research showing that less-chaotic clinics are associated with better communication and greater satisfaction with work-life balance among health care professionals.1 From this vantage point, organizational culture, management style, and team climate might be critical areas for quality improvement in primary care if we wish to promote clinicians’ job satisfaction to decrease burnout and staff turnover and to increase the quality of patient care.
The periphery position of 81% of PCPs being away from the clinical staff in the core (78% nurses, 76% MAs, 62% receptionists) of the team face-to-face communication network might create 2 distinct subgroups in care teams, in which PCPs might be functionally operating in parallel while engaging in a power dynamic with clinical staff. Notably, these parallel organizational structures in team communication were reversed in the electronic communication core, with less than 50% of MAs and 48% of receptionists being in the electronic communication core, whereas more than 65% of PCPs were in the electronic communication core network. Deliberate efforts to clarify team members’ roles and to gain understanding of what each team member brings to the table might help break these team communication silos. Furthermore, the core-periphery communication structures in primary care teams could be exacerbated by the fact that education for physicians and clinical staff is historically conducted separately; doctors learn little in medical school about how they can work with clinical staff, and clinical staff learn little in their medical training programs about working with physicians. Doctors and clinical staff learn to work together for the first time when they start working in the very high-stress, high-stakes environment of primary care clinics, which might contribute to team communication problems. New approaches to medical education, targeting team communication skills, are needed to overcome silo mentality and enhance care team members’ job satisfaction. More than 30 years of research on business and sports teams’ performance reveal that team cohesion—“a dynamic property reflecting members’ perceptions of the unity and personal attractions to task and social objectives of the group”24—is instrumental for teams to achieve high performance outcomes. Given the importance of team cohesion, team-building endeavors should be greatly encouraged in primary care teams to break core-periphery team communication silos and to enhance job satisfaction in primary care.
Finally, it is important to caution readers that this study cannot prove a causal mechanism between team professional communication and job satisfaction, owing to the cross-sectional nature of the study data. Future research might wish to use longitudinal and experimental study designs to identify causal mechanisms between team communication and job satisfaction among team members.
Strengths and Limitations
Strengths of the present study lie in the very high response rates and complete communication networks and job satisfaction data for all of the primary care practitioners. Our findings should be viewed in light of the limitations. First, the study data came from 5 practices in the Midwestern area of the continental United States; therefore, the results might not be generalizable to a broad national or international context. Second, the study looked only at the frequency of face-to-face and electronic interactions and did not attempt to measure communication content. Third, the study did not explore why different team members choose a particular mode of communication (ie, face-to-face vs electronic) to coordinate patient care. Future studies might wish to explore this further. Finally, the multiple comparisons conducted in the analyses increase the likelihood of type I error. Future studies are needed to confirm the results.
CONCLUSIONS
To increase clinician job satisfaction, primary care leadership and stakeholders might be well advised to support efforts to develop highly interconnected face-to-face communication among all team members to leverage the strengths of all health care practitioners and to avoid silo effects among the primary care workforce.
Footnotes
Conflicts of interest: authors report none.
To read or post commentaries in response to this article, see it online at http://www.AnnFamMed.org/content/17/5/428.
Author contributions: M.P.M. had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: M.P.M., L.I.Z.; acquisition, analysis, or interpretation of data: M.P.M., L.I.Z.; drafting of the manuscript: M.P.M., L.I.Z.; critical revision of the manuscript for important intellectual content: M.P.M., L.I.Z.; study supervision: M.P.M.
Funding support: M.P.M. received support from NIAAA grant K01AA018410-04 for the design and conduct of the study. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Role of the sponsor: NIAAA had no role in the design or conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Prior presentation: An earlier version of this work was presented at the North American Primary Care Research Group (NAPCRG) conference; November 17-21, 2017; Montreal, Canada.
Supplemental materials: Available at http://www.AnnFamMed.org/content/17/5/428/suppl/DC1/.
- Received for publication August 31, 2018.
- Revision received February 18, 2019.
- Accepted for publication April 3, 2019.
- © 2019 Annals of Family Medicine, Inc.




{kind=link}