
Article Figures & Data
Figures
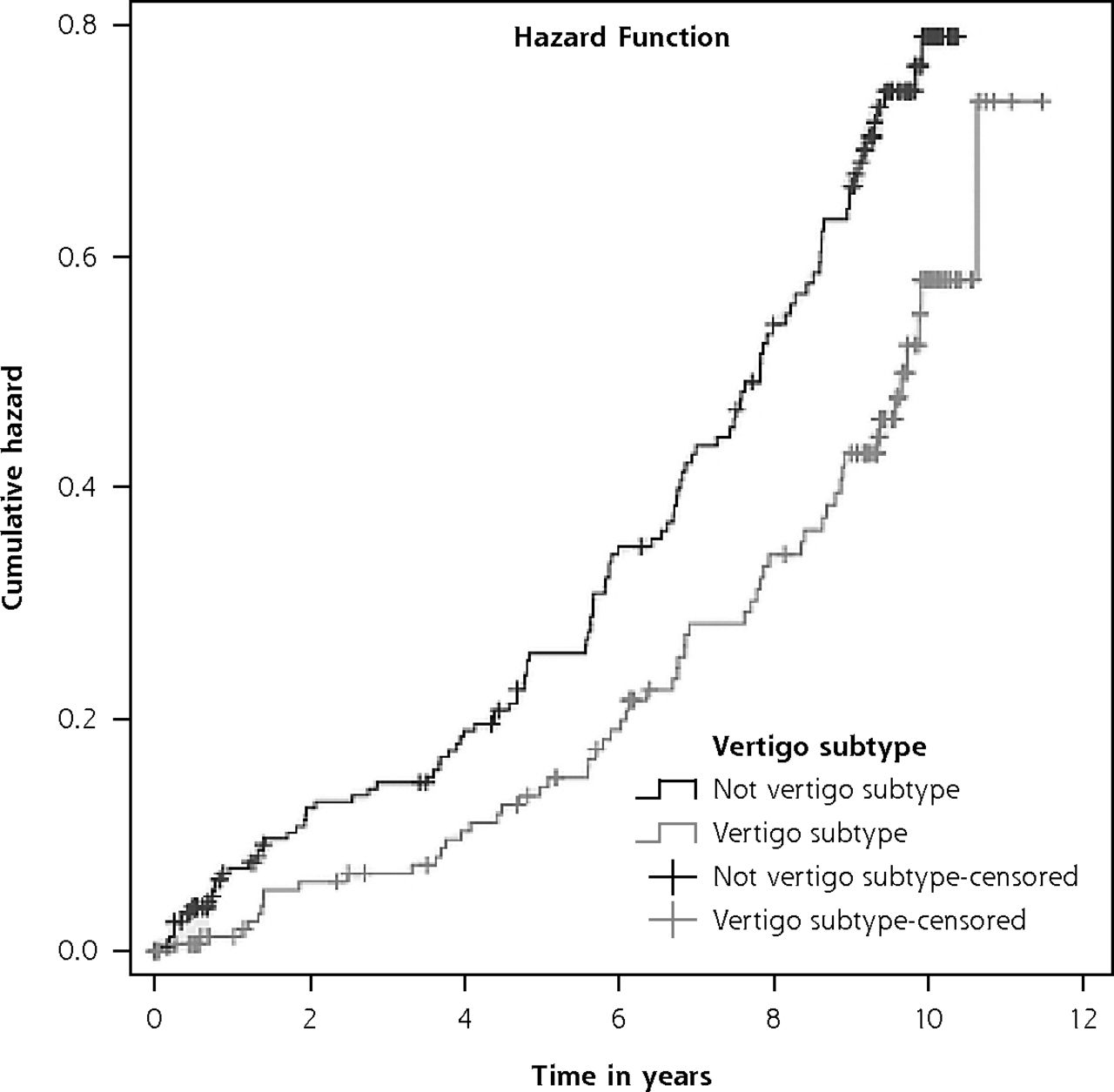
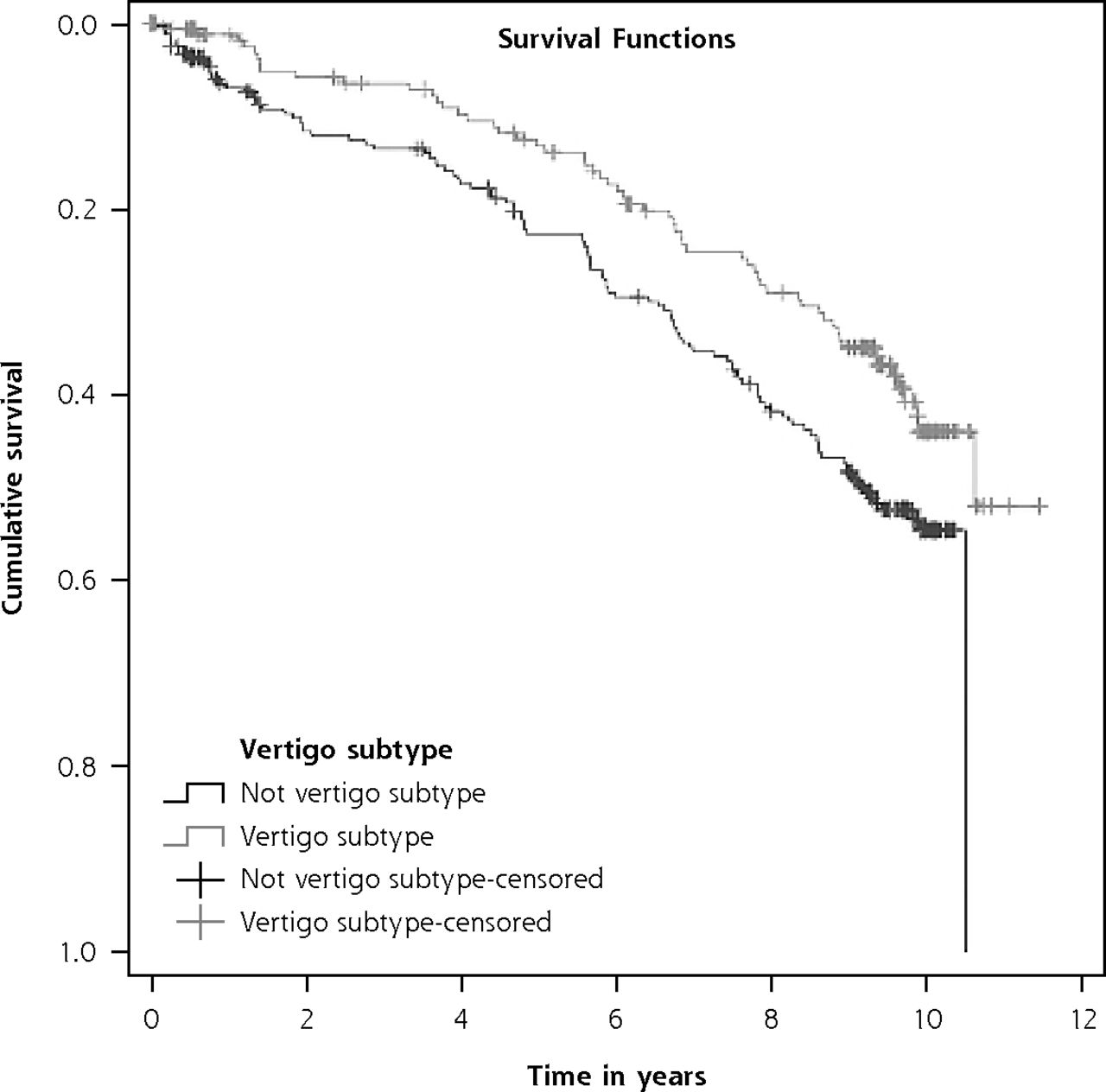
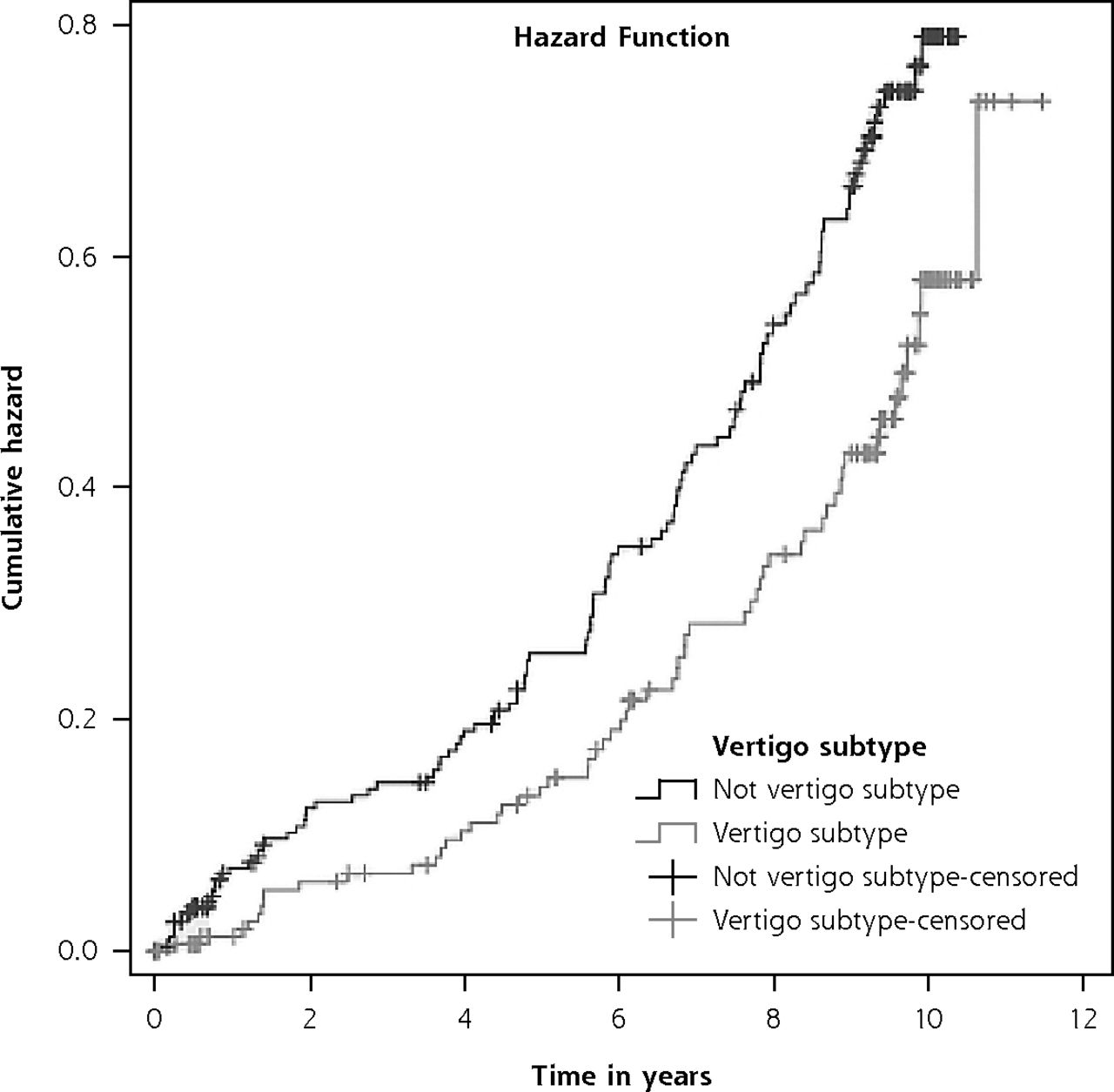
- Figure 1
Kaplan-Meier survival curves for patients assigned to dizziness subtype vertigo.a
aPanel assigned subtype by at least 2 out of 3 panel members. Patients with vertigo compared with patients who were not assigned to this subtype.
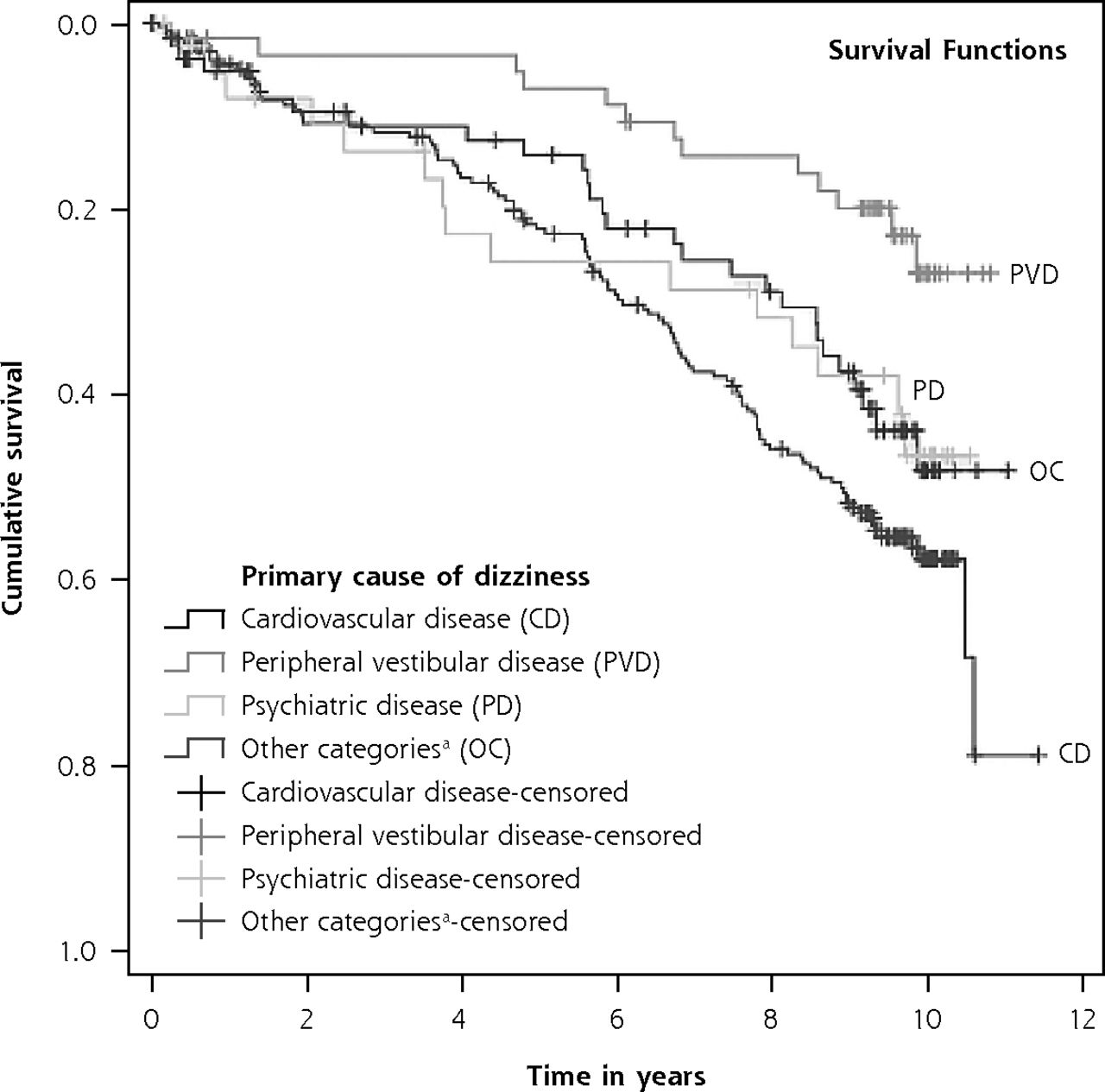
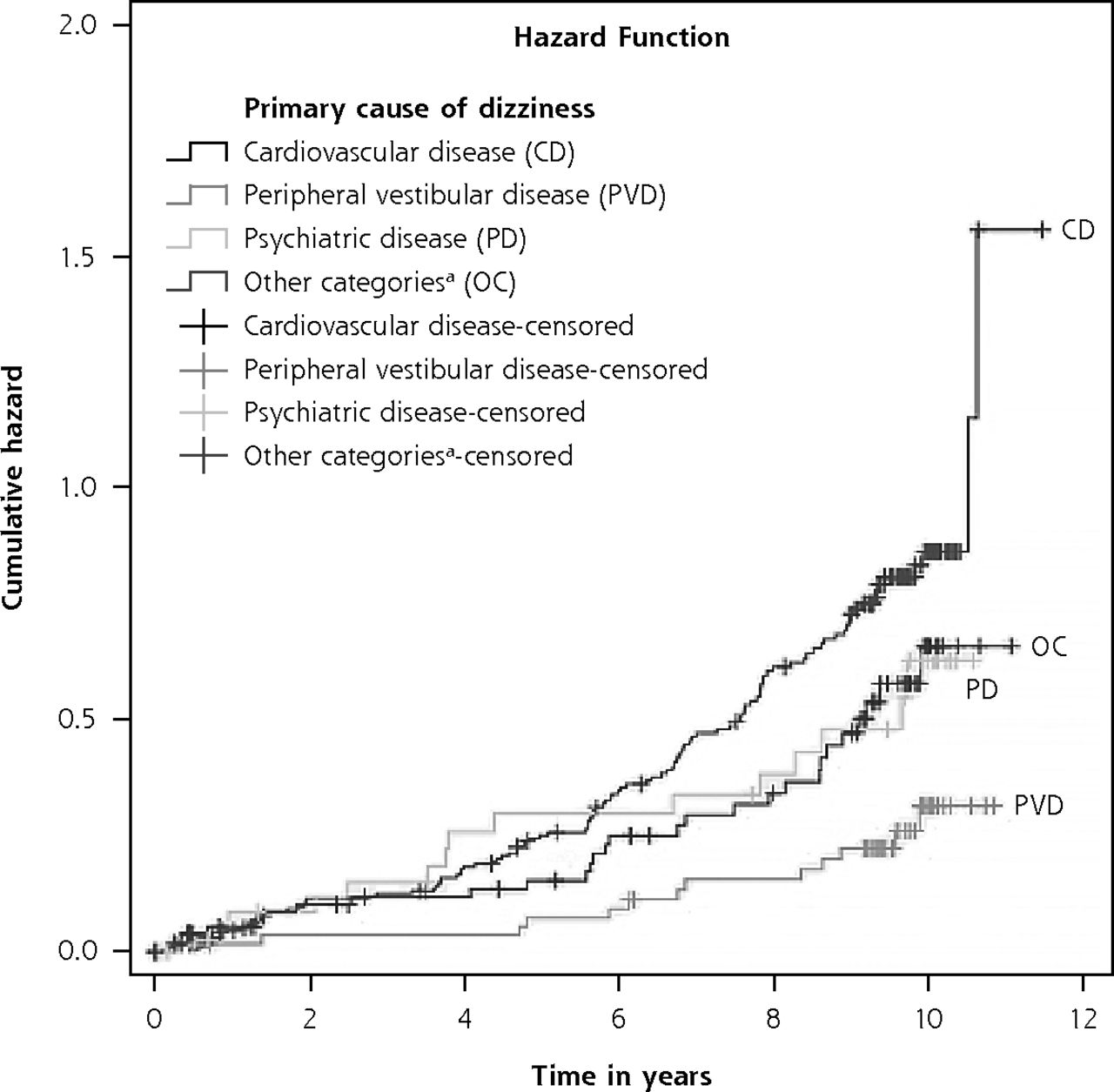
- Figure 2
Kaplan-Meier survival curves for patients with different primary causes of dizziness.
aLocomotor disease, neurologic disease (excluding cerebrovascular disease), adverse drug effect, metabolic or endocrine conditions, impaired vision, other causes, and unclear cause.


Tables
Characteristic Value Demographics Age, mean (range), y 79 (65.0-95.0) Sex, female, No. (%) 307 (73.6) Ethnic background, No. (%) Dutch native 342 (82.0) Western immigrant 31 (7.4) Non-Western immigrant 44 (10.6) Level of education Low, No. (%) 297 (71.2) Middle or high, No. (%) 120 (28.8) Living situation, community-dwelling, No. (%) 397 (95.2) Smoking, No. (%) 62 (14.9) Medical history Cardiovascular disease, No. (%) Hypertension 239 (57.3) Ischemic heart disease 111 (26.7) Arrhythmia 94 (22.5) Heart valve disease 58 (13.9) Myocardial infarction 57 (13.7) Ear, nose, and throat disease, No. (%) Benign paroxysmal positional dizziness 40 (9.8) Ménière’s disease 27 (6.5) Acoustic neuroma 1 (0.2) Neurologic disease, No. (%) Migraine 79 (18.9) Stroke 66 (15.8) Parkinson disease 7 (1.7) Epilepsy 6 (1.4) Multiple sclerosis 1 (0.2) Locomotor disease, No. (%) Osteoarthritis of the knee 120 (28.8) Osteoarthritis of the hip 78 (18.7) Psychiatric illness, No. (%) Depressive disorder 101 (24.2) Anxiety disorder 75 (18.0) Other, No. (%) Diabetes 78 (18.7) Cataract 199 (47.7) Macular degeneration 27 (6.5) Drugs per patient, mean (SD) 4 (3.0) Polypharmacy (>5 drugs), No. (%) 138 (33.0) Dizziness characteristics Onset of dizziness symptoms, No. (%) 2-4 weeks 30 (7.2) 1-6 months 98 (23.5) 6-24 months 110 (26.4) 2-10 years 120 (28.8) >10 years 59 (14.1) Characteristic Value Demographics Age, mean (range), y 79 (65.0-95.0) Sex, female, No. (%) 307 (73.6) Ethnic background, No. (%) Dutch native 342 (82.0) Western immigrant 31 (7.4) Non-Western immigrant 44 (10.6) Level of education Low, No. (%) 297 (71.2) Middle or high, No. (%) 120 (28.8) Living situation, community-dwelling, No. (%) 397 (95.2) Smoking, No. (%) 62 (14.9) Medical history Cardiovascular disease, No. (%) Hypertension 239 (57.3) Ischemic heart disease 111 (26.7) Arrhythmia 94 (22.5) Heart valve disease 58 (13.9) Myocardial infarction 57 (13.7) Ear, nose, and throat disease, No. (%) Benign paroxysmal positional dizziness 40 (9.8) Ménière’s disease 27 (6.5) Acoustic neuroma 1 (0.2) Neurologic disease, No. (%) Migraine 79 (18.9) Stroke 66 (15.8) Parkinson disease 7 (1.7) Epilepsy 6 (1.4) Multiple sclerosis 1 (0.2) Locomotor disease, No. (%) Osteoarthritis of the knee 120 (28.8) Osteoarthritis of the hip 78 (18.7) Psychiatric illness, No. (%) Depressive disorder 101 (24.2) Anxiety disorder 75 (18.0) Other, No. (%) Diabetes 78 (18.7) Cataract 199 (47.7) Macular degeneration 27 (6.5) Drugs per patient, mean (SD) 4 (3.0) Polypharmacy (>5 drugs), No. (%) 138 (33.0) Dizziness characteristics Onset of dizziness symptoms, No. (%) 2-4 weeks 30 (7.2) 1-6 months 98 (23.5) 6-24 months 110 (26.4) 2-10 years 120 (28.8) >10 years 59 (14.1) Frequency, No. (%) Continuous 42 (10.1) Daily 195 (46.8) Weekly 105 (25.2) Monthly 50 (12.0) Annually 25 (6.0) Duration of symptoms, No. (%) <10 seconds 110 (26.4) 10-60 seconds 78 (18.7) Several minutes 71 (17.0) Several minutes to 1 hour 22 (5.3) >1 hour 35 (8.4) Constant when present 26 (6.2) Combination of durations 75 (18.0) Diagnostic tests Psychiatric diagnosis according to PRIME-MD PHQ, No. (%) Major depressive syndrome 53 (12.7) Panic disorder 19 (4.6) Other anxiety syndrome 42 (10.1) MDS, PD, or OAS 90 (21.6) Panel evaluation Dizziness subtype, No. (%) Presyncope 288 (69.1) Vertigo 171 (41.0) Disequilibrium 166 (39.8) Other dizziness 7 (1.7) No consensus 16 (3.8) Number of dizziness subtypes per participant, No. (%) 1 217 (52.0) 2 137 (32.9) 3 47 (11.2) No consensus 16 (3.8) Primary cause of dizziness, No. (%) Cardiovascular disease (including cerebrovascular disease) 237 (56.8) Peripheral vestibular disease 60 (14.4) Other (psychiatric illness, locomotor disease, neurologic disease [excluding stroke], adverse drug effect, impaired vision, metabolic or endocrine conditions, or unclear disease) 120 (28.8) MDS = major depressive syndrome; OAS = other anxiety syndrome; PD = panic disorder; PRIME-MD PHQ = Primary Care Evaluation of Mental Disorders Patient Health Questionnaire.
Dizziness Subtype No. of Persons No. of Deaths Person Years Incidence Rate (95% CI) per 1,000 Person Years Compared With Participants Without This Subtype Unadjusted HR (95% CI) Adjusted HR (95% CI)a Vertigo 171 58 1,213 47.81 (36.30-61.80) 0.64 (0.47-0.88) 0.62 (0.40-0.96) Presyncope 288 126 1,903 66.21 (55.15-78.83) 1.36 (0.96-1.92) 1.23 (0.82-1.85) Disequilibrium 161 65 1,039 62.55 (48.27-79.72) 1.09 (0.80-1.49) 1.26 (0.85-1.87) Other dizziness 7 2 48 41.70 (5.50-150.63) 0.67 (0.17-2.71) 0.76 (0.18-3.18) HR = hazard ratio; PRIME-MD PHQ = Primary Care Evaluation of Mental Disorders Patient Health Questionnaire.
↵a Adjusted for age, sex, ethnicity, level of education, preexistent cardiovascular disease and/or stroke, diabetes, polypharmacy (defined as >5 types of daily medication), an anxiety or depressive disorder according to the PRIME-MD PHQ, and the number of assigned dizziness subtypes.
- Table 3
Hazard Ratios of Mortality in Participants for Different Primary Causes of Dizziness
Primary Cause of Dizziness No. of Persons No. of Deaths Person Years Incidence Rate per 1,000 Person Years (95% CI) Unadjusted HR (95% CI) Adjusted HR (95% CI)a Cardiovascular disease 237 113 1,495 75.61 (62.31-90.90) Reference Reference Peripheral vestibular disease 60 13 495 26.25 (13.98-44.89) 0.32 (0.18-0.56) 0.46 (0.25-0.84) Psychiatric disease 41 15 264 56.88 (31.84-93.82) 0.72 (0.42-1.20) 0.89 (0.49-1.61) Other causesb 79 28 516 54.42 (36.04-78.38) 0.69 (0.46-1.05) 0.66 (0.43-1.02) HR = hazard ratio; PRIME-MD PHQ = Primary Care Evaluation of Mental Disorders Patient Health Questionnaire.
↵a Adjusted for age, sex, ethnicity, level of education, preexistent cardiovascular disease and/or stroke, diabetes, polypharmacy (defined as >5 types of daily medication), an anxiety or depressive disorder according to the PRIME-MD PHQ and the number of assigned dizziness subtypes.
↵b Locomotor disease (n = 15), neurologic disease (excluding cerebrovascular disease) (n = 12), adverse drug effect (n = 10), metabolic or endocrine conditions (n = 3), impaired vision (n = 2), other causes (n = 3), and unclear cause (n = 34).
DHI Score No. of Persons Mean DHI Score, No. (SD) Sustantially Impaired (DHI ≥30), % Baseline (n = 415) 415 36.3 (19.9) 60.7 6-month follow-up (n = 374) 374 28.0 (23.6) 42.2 10-year follow-up (n = 103) 103 31.1 (25.0) 47.7 Patterns of substantial impairment due to dizziness (DHI ≥30) (n = 100)a Never substantially impaired 34 Substantially impaired at 1 or 2 measurements 40 Substantially impaired at all 3 measurements 26 DHI = dizziness handicap inventory.
↵a Only participants who completed a DHI at baseline, 6-month, and 10-year follow-up were included in this analysis. Although 103 participants filled out the 10-year measurement, 3 of these participants missed the 6-month measurement.
- Table 5
Mean Differences in DHI Scores and Odds Ratios to Develop Substantial Dizziness-Related Impairment After 10 Years for Dizziness Subtypes (N = 103)
Subtypes No. of Persons Baseline Values Compared With Participants Without This Subtype Mean DHI (SD) DHI ≥30, % Unadjusted MD in DHI Score (95% CI) Adjusted MD in DHI Score (95% CI)a Unadjusted OR for DHI ≥30, OR (95% CI) Adjusted OR for DHI ≥30, OR (95% CI)a Vertigo 47 34.6 (19.3) 48.9 8.24 (1.12-15.37) 5.13 (−2.66 to 12.91) 1.25 (0.64-2.43) 1.15 (0.44-2.96)c Presyncope 68 29.5 (16.5) 47.1 −3.74 (−11.39 to 3.90) −8.07 (−16.03 to −0.10) 0.89 (0.44-1.79) 0.54 (0.21-1.40) Disequilibrium 66 33.0 (18.3) 51.4 6.20 (−1.29 to 13.69) 2.84 (−5.80 to 11.49) 1.73 (0.85-3.49) 1.73 (0.64-4.66) Other dizziness 3 46.0 (21.1) 66.7 2.15 (−19.48 to 23.78) 0.47 (−18.50 to 19.43) 1.08 (0.16-7.15) 0.87 (0.18-4.21) DHI = dizziness handicap inventory; MD = mean difference; OR = odds ratio; PRIME-MD PHQ = Primary Care Evaluation of Mental Disorders Patient Health Questionnaire
↵a Adjusted for age, sex, ethnicity, level of education, preexistent cardiovascular disease and/or stroke, diabetes, polypharmacy (defined as >5 types of daily medication), an anxiety or depressive disorder according to the PRIME-MD PHQ, and the number of assigned dizziness subtypes.
- Table 6
Mean Differences in DHI Scores and Odds Ratios to Develop Substantial Dizziness-Related Impairment After 10 Years for the Primary Cause of Dizziness (N = 103)
Primary Cause of Dizziness No. of Persons Baseline Values Unadjusted MD in DHI Score (95% CI) Adjusted MD in DHI Score (95% CI)a Unadjusted OR for DHI ≥30, OR (95% CI) Adjusted OR for DHI ≥30, OR (95% CI)a Mean DHI (SD) DHI ≥30, % Cardiovascular 50 28.8 (17.4) 42.0 Reference Reference Reference Reference Peripheral vestibular 23 34.1 (18.1) 56.5 2.60 (−6.67 to 11.87) 3.10 (−5.14 to 11.34) 1.33 (0.56-3.20) 1.46 (0.52-4.08) Psychiatric 12 38.5 (23.2) 58.3 3.39 (−8.44 to 15.22) 1.31 (−9.43 to 12.06) 1.22 (0.43-3.44) 1.01 (0.32-3.25) Other causesb 18 30.6 (17.8) 50.0 −1.00 (−11.11 to 9.12) 3.76 (−5.24 to 12.76) 1.22 (0.48-3.12) 1.63 (0.61-4.30) DHI = dizziness handicap inventory; MD = mean difference; OR = odds ratio; PRIME-MD PHQ = Primary Care Evaluation of Mental Disorders Patient Health Questionnaire.
↵a Adjusted for age, sex, ethnicity, level of education, preexistent cardiovascular disease and/or stroke, diabetes, polypharmacy (defined as >5 types of daily medication), an anxiety or depressive disorder according to the PRIME-MD PHQ, and the number of assigned dizziness subtypes.
↵b Locomotor disease (n = 0), neurologic disease (excluding cerebrovascular disease) (n = 2), adverse drug effect (n = 5), metabolic or endocrine conditions (n = 0), impaired vision (n = 1), other causes (n = 1), and unclear cause (n = 9).
Supplemental Appendixes, Figures, & Table2
Files in this Data Supplement:
- Supplemental data: Appendixes - PDF file
The Article in Brief
Prognosis and Survival of Older Patients With Dizziness in Primary Care: A 10-Year Prospective Cohort Study
Vincent A. van Vugt , and colleagues
Background Dizziness is a common problem among older patients in primary care but is complex for clinicians to measure and diagnose. The diagnostic process is particularly challenging in older patients with dizziness, because the cause of their dizziness is usually multifactorial. Determining the cause of dizziness might help in choosing an appropriate treatment. The research team originally conducted a 2006 prospective cohort study with 417 older adults with dizziness (mean age 79 years) in primary care. At that time, participants received a full diagnostic evaluation by a physician and were classified into four dizziness subtypes: presyncope, vertigo or disequilibrium. The participants were further classified by causes of dizziness, with cardiovascular disease and peripheral vestibular disease being the most common causes. The objective of the current study was to follow participants ten years later to investigate the long-term prognosis of older patients with dizziness in primary care and their mortality and impairment outcomes.
What This Study Found In this 10 year follow up study, 169 (40.5%) of the participants from the previous study had died. Many of the patients still alive at follow-up reported experiencing substantial dizziness-related impairment (47.7%). There was no significant difference in substantial impairment between different subtypes or primary causes of dizziness. Those classified in the vertigo subtype had significantly lower mortality rates than the other subtypes after 10 years. Patients with dizziness caused by peripheral vestibular disease had a lower mortality rate than that of patients with cardiovascular disease.
Implications
- These results provide new insights in the prognosis of older patients with dizziness in primary care. The large percentage of older patients that report experiences of long-term substantial dizziness-related impairment indicates that current treatment strategies in primary care may be suboptimal.




{kind=link}
{kind=link}
{kind=link}
{kind=link}