
Article Figures & Data
Figures
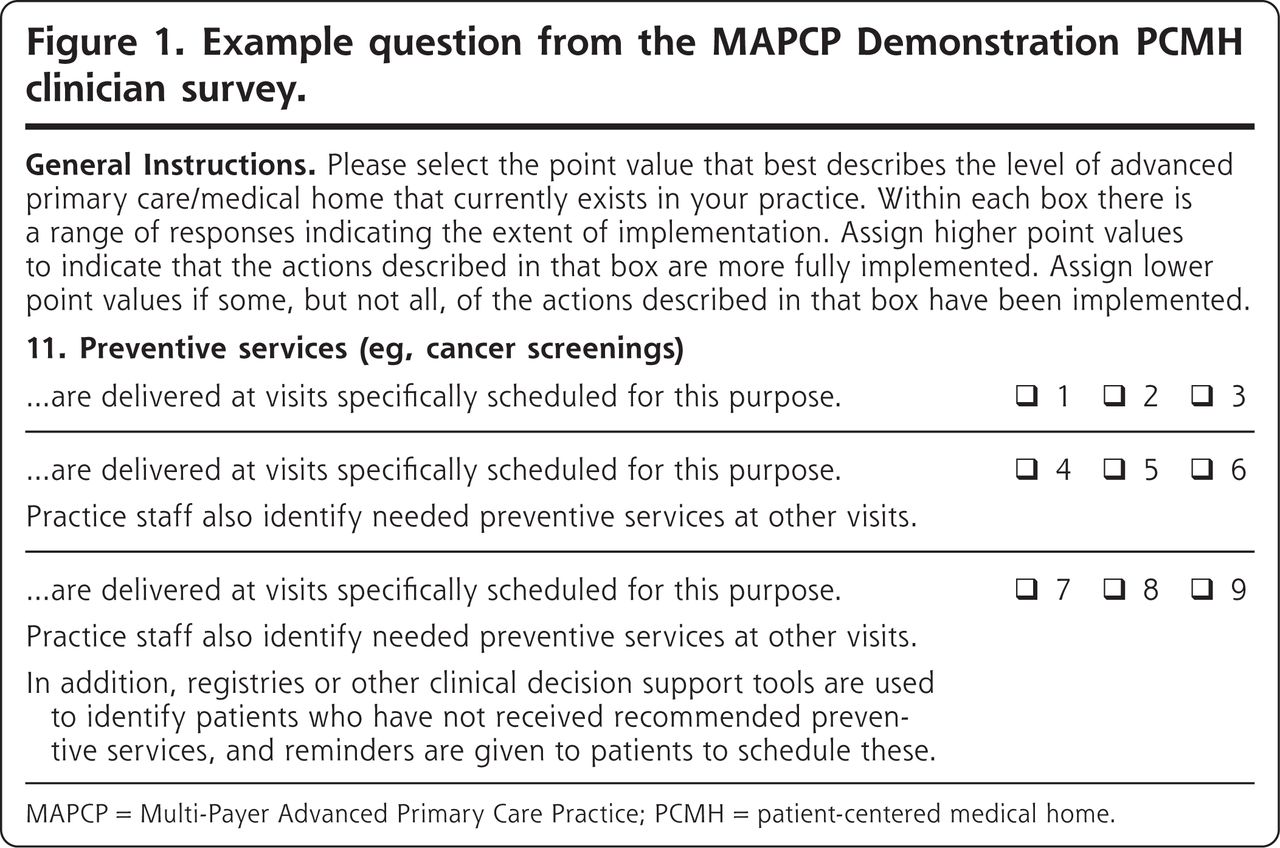
- Figure 1.
Example question from the MAPCP Demonstration PCMH clinician survey.
MAPCP = Multi-Payer Advanced Primary Care Practice; PCMH = patient-centered medical home.
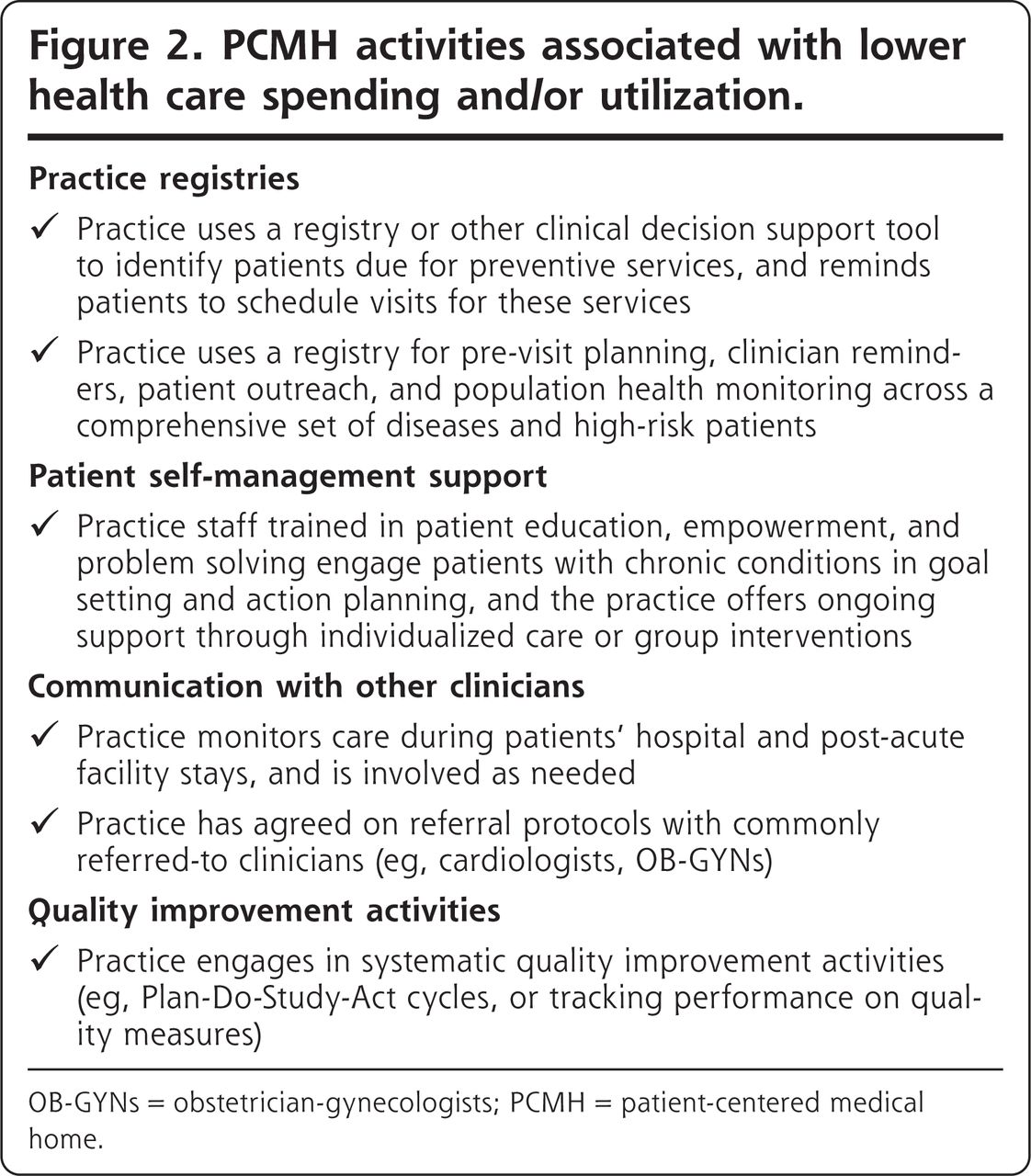
- Figure 2.
PCMH activities associated with lower health care spending and/or utilization.
OB-GYNs = obstetrician-gynecologists; PCMH = patient-centered medical home.

Tables
Characteristics Value Number of practices, No. 394 Number of clinicians, No. 19,456 Number of clinicians per practice, mean 49.38 Number of clinicians per practice, median 19 Practice type, % Office-based practice 79.44 Federally qualified health centera 11.42 Critical access hospital outpatient clinicb 2.54 Rural health clinicc 6.60 Location of practices’ attributed Medicare beneficiaries,d % Metropolitan 69.06 Micropolitane 15.10 Rural 15.84 MAPCP = Multi-Payer Advanced Primary Care Practice.
↵a Federally qualified health centers serve an underserved area or population, offer a sliding fee scale, provide comprehensive services (including dental, mental health, substance abuse, and transportation services), have an ongoing quality assurance program, and have a governing board of directors.
↵b Critical access hospitals are located in a rural area at least 35 miles away from another hospital, have no more than 25 inpatient beds, maintain an annual average length-of-stay of no more than 96 hours for acute inpatient care, and offer 24-hour/7-day-a-week emergency care.
↵c Rural health clinics are located in rural areas that have health care shortage designations, and provide outpatient primary care services and basic laboratory services by a team that includes a mid-level clinician (eg, nurse practitioner, physician assistant, or certified nurse midwife).
↵d Reflects the average percentage of attributed Medicare beneficiaries that reside in metropolitan, micropolitan, or rural areas among the 394 practices.
↵e Micropolitan areas contain an urban core of 10,000-49,999 people.
- Table 2.
Characteristics of Medicare Fee-For-Service Beneficiaries in the Third Year of the MAPCP Demonstration, N = 302,719
Characteristics Value Demographicsa Age, %, y <65 24.76 65-75 44.28 76-85 21.84 >85 9.13 Age, mean, y 68.44 White race, % 88.18 Urban place of residence, % 59.04 Female, % 57.70 Dually eligible for Medicare and Medicaid, % 27.14 Disabled, % 31.77 End-stage renal disease, % 0.81 Institutionalized, % 0.96 Health statusa Hierarchical Condition Categoryb score, mean 1.02 Low risk (< .48), % 24.87 Medium risk (0.48-1.25), % 51.96 High risk (>1.25), % 23.17 Charlson comorbidity indexc score, mean 0.76 Low (= 0), % 64.72 Medium (0 <1), % 17.69 High (>1), % 17.59 MAPCP = Multi-Payer Advanced Primary Care Practice.
↵a Demographic and health status characteristics calculated using the Medicare enrollment database and claims data for the 1-year period before a Medicare beneficiary was first attributed to a practice, after the start of the MAPCP Demonstration.
↵b Hierarchical Condition Category scores use demographic information (age, sex, Medicaid dual eligibility, disability status) and major medical conditions in a base year to predict Medicare spending in the following year. A score of 1.02 means the Medicare beneficiaries in this group were predicted to be 2% more costly than the average Medicare fee-for-service beneficiary.
↵c Charlson Comorbidity Index predicts patients’ mortality or higher health care utilization based on which of the 18 clinical conditions in the index a patient received medical care for in the year before their attribution to a practice. A score of 0 indicates that no comorbidities were found, while a higher score indicates a higher likelihood of mortality or higher health care utilization.
- Table 3.
PCMH Activities Associated With Slower Growth in Spending and Utilization From the Baseline Period to the 3rd Year of the MAPCP Demonstration
PCMH Activity Total Health Care Expenditures PBPM ($) Acute-Care Hospital Expenditures PBPM ($) All-Cause Hospital Admissions Ratea ED Visit Ratea Registries used to identify patients due for preventive services and patients reminded to schedule these visits –69.77b,c
(P = 0.000)–36.62b,c
(P = 0.000)–6.78b
(P = 0.003)–11.05b
(P = 0.05)Registries used for pre-visit planning, clinician reminders, patient out-reach, and population health monitoring across a comprehensive set of diseases and high-risk patients –29.31b
(P = 0.05)–11.64
(P = 0.13)–1.93
(P = 0.21)–5.49
(P = 0.18)Practice staff, trained in patient education, engage patients with chronic conditions in goal setting and action planning, and ongoing support is available through individualized care or group interventions –17.75
(P = 0.34)–14.13
(P = 0.09)–4.62b
(P = 0.01)–11.53b,c
(P = 0.000)The practice monitors patients’ care during hospital and post-acute facility stays, and is involved as needed –22.56
(P = 0.21)–22.06b
(P = 0.03)–2.05
(P = 0.20)–4.99
(P = 0.22)Relationships with commonly referred-to practices (eg, cardiology) are formalized with practice agreements and referral protocols –16.57
(P = 0.28)–8.21
(P = 0.25)–2.10
(P = 0.25)–11.62b,c
(P = 0.000)Quality improvement activities are based on systematic approaches
(eg, Plan-Do-Study-Act, tracking performance on quality measures) and used to meet organizational goals–7.83
(P = 0.71)–4.17
(P = 0.71)–0.20
(P = 0.94)–13.47b,c
(P = 0.000)ED = emergency department; MAPCP = Multi-Payer Advanced Primary Care Practice; PBPM = per beneficiary per month; PCMH = patient-centered medical home.
Note: A negative value indicates slower growth in spending or utilization among beneficiaries served by practices that engaged in a particular PCMH activity relative to beneficiaries in practices that did not, which is considered a favorable outcome. A positive value indicates faster growth among beneficiaries served by practices that engaged in a particular PCMH activity relative to beneficiaries in practices that did not, which is an unfavorable outcome.
↵a Utilization measures are the number of hospital admissions or the number of emergency department visits not leading to a hospitalization per 1,000 beneficiary quarters.
↵b Statistically significant at the 95% confidence level without correction for multiple comparisons.
↵c Statistically significant after correction for multiple comparisons.
- Table 4.
PCMH Activities Lacking Significant Differences in Spending and Utilization From the Baseline Period to the 3rd Year of the MAPCP Demonstration
PCMH Activity Total Health Care Expenditures PBPM ($) Acute-Care Hospital Expenditures PBPM ($) All-Cause Hospital Admissions Ratea ED Visit Ratea Appointment systems have the capacity for walk-ins or same-day visits 7.34
(P = 0.79)5.76
(P = 0.60)–1.06
(P = 0.64)2.24
(P = 0.53)Clinician/practice team has a system to triage patient problems through telephone or e-mail communications or face-to-face visits, with same-day visits usually available 6.30
(P = 0.82)–1.37
(P = 0.92)–0.95
(P = 0.72)–1.54
(P = 0.73)After-hours access to the practice team for urgent care is available by telephone, and in-person during some evenings or weekends; The practice also coordinates ED care, and follows-up with patients after ED visits 3.53
(P = 0.80)–5.49
(P = 0.49)–0.69
(P = 0.67)0.50
(P = 0.90)Alternate types of contact (e-mail, web portal, text message) are used in patient-practice communication, and responses are provided within a timely and consistent timeframe 7.89
(P = 0.67)–7.37
(P = 0.44)–0.48
(P = 0.81)–7.66
(P = 0.06)Tracking and follow-up with patients for important referrals is consistently done –8.59
(P = 0.64)–5.97
(P = 0.50)2.21
(P = 0.41)0.67
(P = 0.83)Patient referral information to specialists, hospitals, and other medical care providers is consistently transmitted by the practice 14.09
(P = 0.62)5.47
(P = 0.75)–1.02
(P = 0.62)2.66
(P = 0.68)Practices follow up with patients who have been referred to behavioral health supports or community-based resources (eg, social services) 17.20
(P = 0.26)13.83
(P = 0.11)0.28
(P = 0.90)–2.86
(P = 0.46)Follow-up with patients seen in the ED or hospital is done routinely after receiving notification from the ED or hospital –31.05
(P = 0.16)–15.03
(P = 0.17)–1.65
(P = 0.37)–5.96
(P = 0.11)Visit focus is organized around the reason for a patient’s visit, but with attention to ongoing chronic care and prevention needs –16.67
(P = 0.42)–13.93
(P = 0.21)–1.93
(P = 0.36)–2.03
(P = 0.58)Medication review for patients on multiple medications is done during care transitions, when patients receive new medications, and during all regularly scheduled visits 11.51
(P = 0.48)–1.04
(P = 0.93)2.29
(P = 0.21)10.03
(P = 0.19)Practice identifies complex patients who may benefit from clinical care management, and actively coordinates their care management with other clinicians and caregivers –13.48
(P = 0.48)–2.89
(P = 0.76)–3.44
(P = 0.12)–10.14
(P = 0.13)Tracking and follow-up with patients about test results is consistently done for all tests –9.25
(P = 0.60)–16.94
(P = 0.09)–1.51
(P = 0.58)–5.41
(P = 0.32)Care plans for patients with chronic conditions are recorded in patient medical records, used to guide care, and are given to the patient –16.53
(P = 0.22)–9.65
(P = 0.17)–1.53
(P = 0.31)–0.64
(P = 0.84)Assessing patient values and preferences (eg, for end-of-life care, role in decision-making) is done for all patients with significant health problems or who articulate values and preferences themselves –15.92
(P = 0.28)–10.93
(P = 0.13)–0.28
(P = 0.85)–7.12
(P = 0.16)Involving patients in shared decision-making is a priority and systematically done, through clinical decision aids, motivational interviewing, and/or teach-back techniques 5.17
(P = 0.74)7.93
(P = 0.37)0.85
(P = 0.65)–5.54
(P = 0.12)Feedback to the practice from patients is regularly and formally collected (eg, through a patient survey or focus group) and informally (eg, through specific patients’ concerns), and used to improve the practice 0.46
(P = 0.97)2.67
(P = 0.75)1.00
(P = 0.63)–5.31
(P = 0.13)ED = emergency department; MAPCP = Multi-Payer Advanced Primary Care Practice; PBPM = per beneficiary per month; PCMH = patient-centered medical home.
Note: A negative value indicates slower growth in spending or utilization among beneficiaries served by practices that engaged in a particular PCMH activity relative to beneficiaries in practices that did not, which is considered a favorable outcome. A positive value indicates faster growth among beneficiaries served by practices that engaged in a particular PCMH activity relative to beneficiaries in practices that did not, which is an unfavorable outcome.
↵a Utilization measures are the number of hospital admissions or the number of emergency department visits not leading to a hospitalization per 1,000 beneficiary quarters.
Supplemental Appendix
Supplemental Appendix
Files in this Data Supplement:
- Supplemental data: Appendix - PDF file
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Sustainability of Evidence-Based Practice Improvement Programs in Abu Dhabi Ambulatory Healthcare Services for more than a decade and During the COVID-19 Pandemic
- Revitalizing Primary Care, Part 2: Hopes for the Future
- Can You Hear Me Now? Refining the PCMH Model and an Overlooked Disability Affecting Seniors