
Abstract
People working on behalf of population health, community health, or public health often experience confusion or ambiguity in the meaning of these and other common terms—the similarities and differences and how they bear on the tasks and division of labor for care delivery and public health. Shared language must be clear enough to help, not hinder people working together as they ultimately come to mutual understanding of roles, responsibilities, and actions in their joint work. Based on an iterative lexicon development process, the authors developed and propose a definitional framework as an aid to navigating among related population and community health terms. These terms are defined, similarities and differences clarified, and then organized into 3 categories that reflect goals, realities, and ways to get the job done. Goals include (a) health as well-being for persons, (b) population health as that goal expressed in measurable terms for groups, and (c) community health as population health for particular communities of interest, geography, or other defining characteristic—groups with shared identity and particular systemic influences on health. Realities are social determinants as influences, health disparities as effects, and health equity as both a goal and a design principle. Ways to get the job done include health care delivery systems for enrollees and public health in population-based civic activities—with a broad zone of collaboration where streams of effort converge in partnership with served communities. This map of terms can enable people to move forward together in a broad zone of collaboration for health with less confusion, ambiguity, and conflict.
THE IMPERATIVE AND THE PROBLEM
The terms population health, community health, and public health are often used interchangeably, yet imprecisely, leading to conceptual and practical misunderstandings. Each term relates in its own way to primary care and larger care delivery systems. Shared definitions enable people to create an agenda for shared work, making it possible for people from different disciplines, roles, types of organizations, and age groups to work together1,2 on behalf of the larger goal of population health improvement.3,4 Often people say they are doing “population health,” but mean very different things. Knowing they are in it together, people working in the crucibles of population health improvement are passionate, but often don’t share sufficient common language to proceed with their work without asking, “What do you mean by that?” or “Is this the same thing as that?” (Table 1). This goes beyond mere ambiguity to strong feelings about the importance of language and meanings in your own discipline or “guild”5; words or professional practices that are precious, protected, and not to be misunderstood or appropriated.
Common Meanings for “Population” From Different Standpoints
This paper doesn’t try to eliminate strongly held meanings or local usage, but offers an example of language based in common understandings and hopefully is good enough to help people move forward together with less confusion, ambiguity, and conflict.
The COVID-19 pandemic amplified the need for care delivery systems, public health, and other sectors to work together at an accelerated pace with even less energy available for misunderstanding and ambiguity.6-8 Shared language for shared work is important not only for division of labor, but for teaching clinicians, public health students, and others to work effectively, one with the other, in different settings.9 Shared language is also important for policy and advocacy, making the subjects more consistent and intelligible to policy makers or funders, who otherwise confuse words that sound similar but are used differently by people in different professional settings.
Coming Together on Shared Language for Shared Work
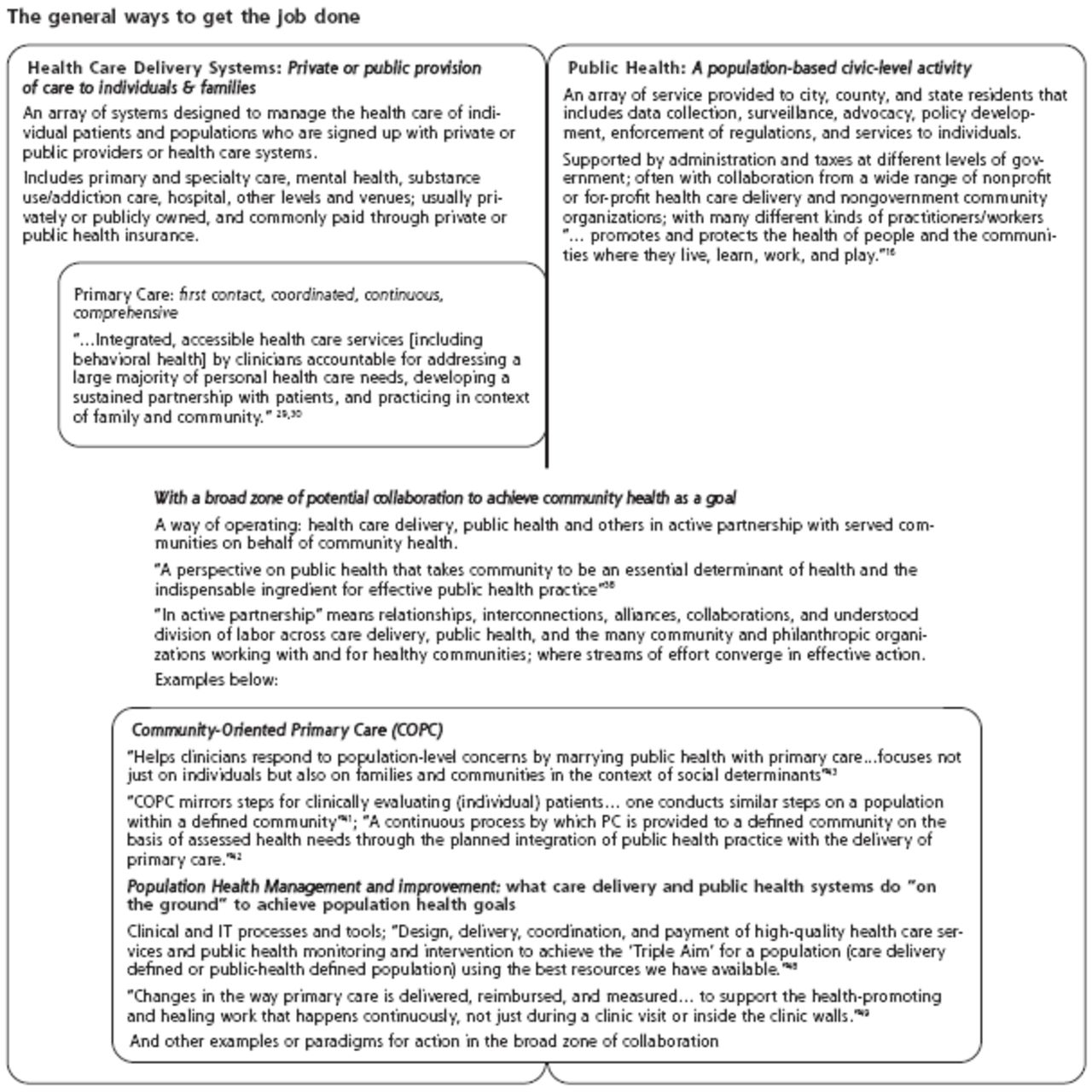
In this article, we attempt to define and distinguish commonly used terms in a manner that helps people share enough common language to get work done together. We propose a framework of definitions (Figure 1) as an aid to navigation for related population and community health terms. If you wish to view, download, or print the figure in its original large 1-page form, please go to https://www.AnnFamMed.org/lookup/suppl/doi:10.1370/afm.2708/-/DC1. . This lexicon places terms in a relational context—from goal-oriented language at the top to “how-to” language at the bottom. The illustration was created by the authors, a sample of professionals working in crucibles10 of population health who agree that shared language propels practical work forward in the push-pull of differing roles and responsibilities. The authors believe that the goal of population health is achievable—with better collaboration between primary care and public health, a supportive environment at the policy and health system level, and attention to the social and environmental realities that affect the health of communities and individuals. Figure 1 suggests what such a depiction can look like and how shared meanings can be articulated.


Population and community health terms: navigating the territory.
IT = information technology; COPC = community-oriented primary care; PC = primary care.
If you wish to view, download, or print the figure in its original large 1-page form, please go to https://www.AnnFamMed.org/lookup/suppl/doi:10.1370/afm.2708/-/DC1
These definitions will surely evolve as new disciplines, methods, sources, and stakeholders join the fray—people beyond the present authors—including patients, community members, public health practitioners, and other groups focused on health inequities. This lexicon is intended to be useful now—as a reflection of current reality—not as an ideal future reality, nor as a set of definitions for all time, generated by all people. At the same time, it incorporates definitions and meanings from published accepted language.
How We Arrived at the Lexical Diagram
A group of US colleagues working on population health initiatives were asked to provide feedback to the University of Minnesota (UMN) authors on an early version of Figure 1. Subsequently, the Annals of Family Medicine and the Robert Graham Center jointly sponsored synchronous and asynchronous virtual communications in which C. J. Peek devised and facilitated an iterative consensus process with a panel of 10 professionals with expertise in population health. A modified Delphi process was used to establish “good enough” shared language, placed in a relational context and describing current reality, to create a revised figure.
A TOUR OF THE LEXICON DIAGRAM
Top Rows—Goals and Expressing Them Measurably
Health and Population Health
In 1948 the World Health Organization (WHO) defined health as not merely the absence of disease or infirmity, but as a dynamic state of physical, mental, spiritual, and social well-being.11 This definition focused primarily on the welfare of individuals. Six decades later, WHO specified the need to achieve better health for all by reducing exclusion and social disparities in health.12 Kindig defined this goal as “population health,” with emphasis on health outcomes of a group of individuals, in addition to the distribution of outcomes within the group.13,14 The Centers for Disease Control and Prevention (CDC) goes further to acknowledge that conditions in which people are born, grow, live, work, and age, as well as the distribution of money, power, and resources, all influence population health.15,16
Population Health as a Goal With Measures
Population health as a goal with measures may be encountered in different ways for different purposes, eg, good health status in a population or delineated subpopulation, improvement of health in that population, or reduced variability (greater equity) of health status across members or subgroups. “Everyone has a fair opportunity to attain their full health potential.”17 Population health measures might be encountered as a snapshot in time or as a change trend, for a whole geographically or otherwise defined population, or for specific subpopulations for purposes of understanding health disparities.
Population Health Management
Population health as a goal with measures is distinct from the concept of population health management (shown in the bottom row), which is used to refer to tools and methods used by delivery systems or public health, to achieve such population health goals and are reflected in specific population health measures.
Community Health as a Goal
Community health as a goal, on the other hand, defines population health goals for particular communities with a shared identity, as defined by common interests, problems, fate, or those who live in a common environment, and with whom several primary care clinicians interact over time.18 Specific communities of interest share an identity and benefit from their systemic influences, resulting in overall community health greater than the sum of the health of individuals within the group.19,20 A particular community might have better (or poorer) health than the larger population of which it is a part, due to strong salutogenic (or pathogenic) features of that community. Influences on health of a community as a whole could include presence or absence of sanitation systems, refrigeration, electricity or Internet, accessible transportation, walkable cities, neighborhood safety with well-used public areas, access to care and nutritious groceries, school attendance, or literacy. Communities are seen as having collective assets and strengths enabling them to serve as “communities of solution” to achieve population health.21-23
Middle Rows: Realities That Affect and Shape How Goals Can Be Achieved
Social Determinants of Health, Health Disparities, and Health Equity
Numerous social determinants of health (influences) can either positively or adversely affect community and population health outcomes.12,15,24 These result in health disparities (consequences).25,26 Health equity is both a goal and a design principle: The goal is the absence of avoidable or remediable health differences among groups of people defined socially, economically, or by other means—the opportunity to attain full health potential.27 As a design principle, health equity means health-linked systems are redesigned to address and eliminate unjust, potentially reversible health disparities among socially disadvantaged populations, while accepting the effects of historical injustice.28 Examples of background realities affecting determinants, disparities, and equity are shown beneath all 3 in the figure.
Bottom Rows: Ways to Get the Job Done
Health Care Delivery System and Primary Care
To date, the goal of traditional US health care delivery systems has been to provide cost-effective, quality care for enrollees in private or public health plans. Government, military, and commercial insurance programs fund primary, specialty, hospital, and other levels of care. Primary care forms the foundation of a strong health care system.29,30 Many primary care clinicians have transformed their practices into “patient-centered medical homes,” or similarly named entities, to provide coordinated, comprehensive, team-based care.31,32 These new care models were developed specifically to achieve the Institute of Health Improvement’s (IHI) Triple Aim to improve the health of populations, reduce per capita cost of health care, and improve patient experience.33 As the primary care specialty committed to first contact, comprehensive, continuous, and coordinated care for patients of all ages,22 family medicine has a broad scope of practice, a focus on prevention, and a community orientation that invites effective collaboration and partnership with public health colleagues and community organizations who are committed to community health.34,35
Public health
Public health is a population-based civic-level activity to prevent disease, prolong life, and promote the health of people in the jurisdictions where they live, learn, work, and play.36,37 Functions typically include collecting region-specific health data, conducting disease surveillance, advocating and enforcing health-related policies and regulations, and providing some medical services in response to community need. Public health departments are primarily government-funded, civic agencies comprised of many different kinds of practitioners, using tax dollars to serve those living in defined geographic areas, even as they often and widely collaborate with nonprofit, or for-profit community entities. Differences in funding sources and accountabilities associated with the private nature of care delivery and the public nature of public health often complicate collaboration.
A BROAD ZONE OF COLLABORATION
The authors believe the goals of population health can be accomplished by robust cooperation and practical division of labor between care delivery and public health to achieve community health as a goal.38 This broad zone of collaboration has limitless possibilities for health care delivery, public health, and other private or public entities to build active partnerships with served communities. People working in this zone cultivate connections, alliances, and collaboration with a mutual understanding of the division of labor across care delivery and public health, along with philanthropic organizations working for healthy communities. Streams of effort converge in effective action. Each stream has its own main job, even when there is overlap. For example, the care delivery job is stereotypically oriented to treatment of conditions for individuals, whereas the public health job is primarily oriented to protecting or improving health for neighborhoods, communities, or populations.39
Community-Oriented Primary Care
Community-oriented primary care (COPC) has a long history of helping clinicians respond to population-level health concerns through collaboration with public health and communities.40,41 Essential to COPC is community engagement and co-leadership, whereby community stakeholders identify health issues and culturally appropriate interventions to address relevant concerns, focusing on families and communities, not only individuals.42,43 The 2012 Patient Protection and Affordable Care Act provided added impetus for such collaboration.44 Not-for-profit health systems, now required to complete community health needs assessments, often look to local departments of public health for assistance. Recent reports of successful primary care-public health collaborations designed to improve health in particular populations are encouraging.45 At their inception, federally qualified health centers and their neighborhood health center predecessors were rooted in this philosophy, recognizing community itself as an essential determinant of health.46,47
Population Health Management and Improvement
Population health management and improvement, a modern and system-oriented term, refers to clinical and information technology (IT) processes, tools, and techniques available within the broad zone of collaboration of care delivery and public health that can help both achieve population health goals. This concept became well known in context of care delivery systems’ Triple Aim but applies equally well to public health tools and techniques.48,49
There are surely other examples, programs, traditions, or paradigms that could be added to these 2 examples of active partnership of care delivery with public health.
CONCLUSION
The goal of population health is achievable with better collaboration between primary care, public health, and others at the local community health level, attention to the social and environmental realities that affect the health of communities and individuals,50 and a responsive environment at the policy and care delivery system level. To prevent people talking past each other, shared language with common meaning is necessary for effective collaboration. But collaboration requires broadly shared language and meaning. Previous lexicon work in emerging fields enhanced shared understanding51 needed for action and policy development.2,52
The figure is a pragmatic start to common language for moving shared work forward in an environment sufficiently shaken by pandemic and racial injustice so that positive change, previously unfathomable, may now be possible. We hope the figure helps those engaged in population and community health work navigate current reality with less confusion or misunderstanding, while encouraging conversations about envisioning and building stronger relationships between care delivery systems and public health on behalf of health equity for all people and communities. Shared language for shared work is only a first step in an effort to realize a more ideal future.
We encourage readers to share this navigational aid with clinicians, researchers, learners, funders, and community members, particularly when starting new clinical initiatives, research projects, or partnerships. We welcome feedback as to how this figure can be improved and examples of how this lexicon has been used to facilitate shared work.
Acknowledgments
The authors thank Annals of Family Medicine and the Robert Graham Center for co-sponsoring the interactive process to develop this paper and its figure. More specifically, Ellen McCarthy and John Holkeboer of the Annals of Family Medicine editorial team and Jack Westfall of the Robert Graham Center, who is a co-author. We thank Glen Mays of the University of Colorado for his contributions at the initial live interactive session.
Thanks also goes to Nancy Baker, who felt a strong need for shared language in resident and medical student curricula on population and community health. She instigated this work by pulling together her University of Minnesota colleagues (with thanks to Christopher Reif) to develop the first iteration of the figure, took the lead in writing the initial submission for publication, and wisely helped shape article content and editorial choices at every stage.
Footnotes
Conflicts of interest: authors report none.
To read or post commentaries in response to this article, go to https://www.AnnFamMed.org/content/19/5/450/tab-e-letters.
- Received for publication September 30, 2019.
- Revision received January 11, 2021.
- Accepted for publication January 25, 2021.
- © 2021 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}