
Article Figures & Data
Tables
Embedded Programs (n = 15) Standalone Programs (n = 12) Key Features Example Quote Key Features Example Quote Activities to address social needs were embedded within existing clinical care management programs. Motivated to address needs that impacted clinical care
Provided referrals to CBOs
Provided information, coached patients, assisted with paperwork, attended appointments
Relied on existing care management staff
Patients were enrolled in care management due to clinical conditions or recent hospitalization
Social needs often identified after enrollment
“When we’re monitoring them, they’ve either been uncontrolled or been in the hospital in the last six months, so they’ll either be monthly or biweekly calls. And when they’re just, multiple chronics, multiple hospitalizations, then we want to go to bimonthly or weekly calls.” (Practice; O14; case management staff) Focused on addressing social needs independent of clinical activities.
Motivated to address social needs because of their mission
Addressed social needs regardless of clinical need or complexity
Provided information, coached patients, assisted with paper-work, attended appointments
Primarily staffed by community health workers and social workers
Social needs identified via screening or provider referral
“It typically looks like a personal introduction by the clinic that’s serving the member or patient, so that they’re saying, ‘As your care team, we want to bring in [community health worker] as a part of the care team to be a part of our work with you, and we’d really like to have her come out to your home and meet you or whatever you would prefer. Would you be willing to engage in that?’ They’re really trying to do a warm intro and hand-off, and then that person is following up through whatever mechanism the patient said they preferred, a phone call, a text, a visit.” (System; O5; executive leadership) CBOs = community-based organizations; O = organization.
Type of Assistance Low Intensity Medium Intensity High Intensity Range of activities “…give them the address and information to take.” (Practice; O26; program management) “…help you go through this process of completing the eligibility paperwork.” (System; O5; executive leadership) “This was a couple that was homeless. Two of the [staff] worked together and they just got everything together for this couple. They got them a home. They got them furnishings, whatever they needed.” (System; O12; case management staff) Interactions with CBOs “I’ll call first. Because a lot of these resources, they’re here one day and gone the next.” (Practice; O16; case management staff) “The referral navigator may call and make an appointment for them right then, and really take it one step further.” (System; O3; program management) “We’re becoming authorized representatives, which is a fancy word to say that we can speak on the behalf of the patient.” (System; O21; case management staff) Patient follow-up “I think that when the patient presents again that conversation does happen. Just to make sure that they had the services, they’re able to access those services.” (System; O13; program management) “They would provide the information through the mail and call and be like ‘Did you get this?’ Make sure they actually handed it in.” (System; O2; program management) “Then the next step is follow-up daily to confirm that client is accessing the resources identified and/or has implemented the plan.” (Practice; O8; program management/practicing clinician) CBOs = community-based organizations; O = organization.
Social Care Approach Organizational Approach and Example Quotes Program structure for treating social needs Treated as an acute condition
“If you have a Medicaid patient who has transportation needs to health care visits. That’s easy to solve. You can solve that in one phone call.” (System; organization 8; executive leadership)
“So that to me is short-term case management. That’s one, maybe two visits. It’s problem-solving, and then you move it through.” (System; organization 21; executive leadership)Treated as a chronic condition
“I’m looking at some of the patients that I’m working with now and it may take several home visits or several calls just to complete one task. So they will be staying with you for a while. It’s hard to say, but in general a few months maybe.” (System; organization 12; case management staff)Program design of staff and patient collaboration for development of social care plans Health care staff drove the care plan
“I tell them I will make a care plan for your needs.” (Practice; organization 16; case management staff)
“She wanted her Medicaid [renewal]. But in looking over her papers, we noticed that […] she hadn’t paid her taxes in I don’t know how many years […]. We said, “You know what? This is the most important thing. This is what’s going on right now.” (Practice; organization 15; case management staff)Patients drove the care plan
“The patient may identify a different set of goals than what you would have guessed looking at that screener. We spend a lot of time working on motivational interviewing and really person-centered goal setting.” (System; organization 8; executive leadership)Extent of health care organizations encouraging staff to partner with patients to address social needs Patients were primarily responsible
“It’s essentially connecting them and giving them the information and then it’s up to the patient to contact those organizations and move the steps forward.” (Practice; organization 1; program management)
“So, we try to empower our patients, and so if it’s a patient who either can certainly do things on their own, they just don’t know how to access resources, they’ll teach them or talk to them about what’s available. They’ll sit with them to make phone calls if they need to.” (System; organization 12; executive leadership)Staff and patients were a team
“Years ago he had lost his birth certificate. He was living in his truck down by the river. […] Our case manager worked with him through an entire process […] Once that [identification] got here then she assisted him to complete the housing applications that he needed to complete. Once that was done he actually got a house, or an apartment. Then she continued to follow up with him for I think it was six months. And he’s doing fantastic.” (Practice; organization 18; case management staff)Operational Challenges Example of Challenge Example of How Challenge was Managed Strategiesa Engaging CBOs
Referrals require interaction with CBOs
CBOs may have capacity challenges
CBOs may want a role in developing programs
CBOs may work with multiple health care organizations
“We also have […] a large health system in our region, and they are also implementing [referral platform]. However, they’ve rebranded theirs [website name] and so they’ve caused a little bit of confusion in the community.” (Organization 3; program management) “We did a survey of our community organizations and asked them what it was like to work with health systems. And they found that there were three major issues….” (Organization 23; executive leadership) Engage with CBOs early when developing programs that rely on their services or expertise
If choosing a platform, ensure CBO buy-in before purchasing
Foster both leader-to-leader and staff-to-staff relationships between health care organization and CBOs
Buy-in among clinical staff
Nurses, medical assistants, and physicians are often not trained in social care
Staff may already feel Overwhelmed
“Before we started our community health worker program our nurses and social workers […] were struggling to work at the top of their license. […] they had at first try to deal with the social determinants.” (Organization 12; executive leadership) “It’s training somebody up and it has to be somebody who just has that knack. They’re compassionate, they can just connect with the patient, build rapport. It’s harder than you think…” (Organization 6; program management) Train staff to deliver assistance that is culturally competent and is sensitive to patients’ experiences
Assign staff with skills in motivational interviewing, emotional intelligence, and community navigation
Patients’ perspectives
Some patients may not want assistance
Patients may prioritize needs differently
Patients may have existing relationships with CBOs
“Why they will follow up with us and why they will not […]. We’ve got these wonderful programs, and people screen positive for something, why don’t they want to do something about that?” (Organization 24; executive leadership) “’Would you like help? Would you like me to meet with you? Would you like some assistance working on some of these challenges’ and then engage in a relationship with that patient to establish patient goals and then to create some plans to meet those goals.” (Organization 8; executive leadership) Engage patients when developing programs
Patients can provide input into available resources and experiences using resources
Engage patients in defining goals, providing assistance, and prioritizing referrals to CBOs
Program sustainability
How to measure success?
Organizational commitment for short-term versus long-term
“So having that capability [social worker] in house has made a huge difference, even though it’s not necessarily remunerated, which is a problem.” (Organization 28; practicing clinician) “I think the key thing is how do we pay for this. I think that’s got to be on the top of everyone’s list right now. We’re paying for all of that. What’s the return on that investment? I don’t know.” (Organization 8; executive leadership) Establish goals for the program before starting
Organizations with fewer resources may choose embedded programs which typically rely on existing staff
CBOs = community-based organizations.
↵aStrategies are based on suggestions from interviewees and expanded by authors through analysis.
Additional Files
Supplemental data
- Fraze.pdf -
PDF file
- Fraze.pdf -
Visual abstract
.png file
In Brief
Resource Brokering: Efforts to Assist Patients With Housing, Transportation, and Economic Needs in Primary Care Settings
Taressa K. Fraze and colleagues
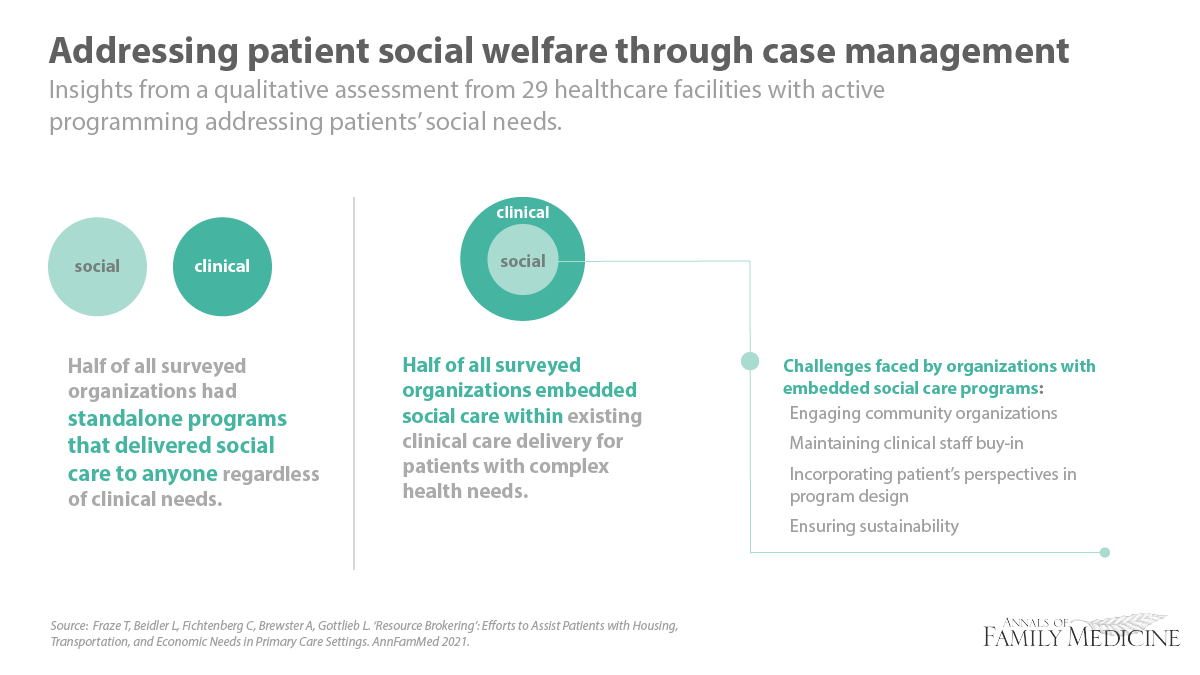
Background Health professionals recognize that social factors such as food, housing and economic insecurity, affect health outcomes. Researchers conducted a qualitative study to gain practical insights into strategies used by clinicians, leaders and policymakers to address patients’ social needs in the United States. They selected sites to ensure diversity in ownership, structure, geography and urbanicity, ranging from small primary care practices to multi-state health systems. Interviews focused on how organizations develop and implement case management-style programs to assist patients with social needs including staffing, assistance intensity and use of referrals to community-based organizations.
What This Study Found The authors identified four barriers to addressing patients’ social needs including: 1) effectively engaging CBOs; 2) obtaining buy-in from clinical staff; 3) considering patients’ perspectives; and 4) ensuring program sustainability.
Implications
- Researchers conclude that many health care organizations will likely develop or rely on case management approaches to address patients’ social challenges and may require support to address the key operational challenges.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.