
Abstract
PURPOSE In the United States, primary care practices rely on scarce resources to deliver evidence-based care for children with behavioral health disorders such as depression, anxiety, other mental illness, or substance use disorders. We estimated the proportion of practices that have difficulty accessing these resources and whether practices owned by a health system or participating in Medicaid accountable care organizations (ACOs) report less difficulty.
METHODS This national cross-sectional study examined how difficult it is for practices to obtain pediatric (1) medication advice, (2) evidence-based psychotherapy, and (3) family-based therapy. We used the National Survey of Healthcare Organizations and Systems 2017-2018 (46.9% response rate), which sampled multiphysician primary and multispecialty care practices including 1,410 practices that care for children. We characterized practices’ experience as “difficult” relative to “not at all difficult” using a 4-point ordinal scale. We used mixed-effects generalized linear models to estimate differences comparing system-owned vs independent practices and Medicaid ACO participants vs nonparticipants, adjusting for practice attributes.
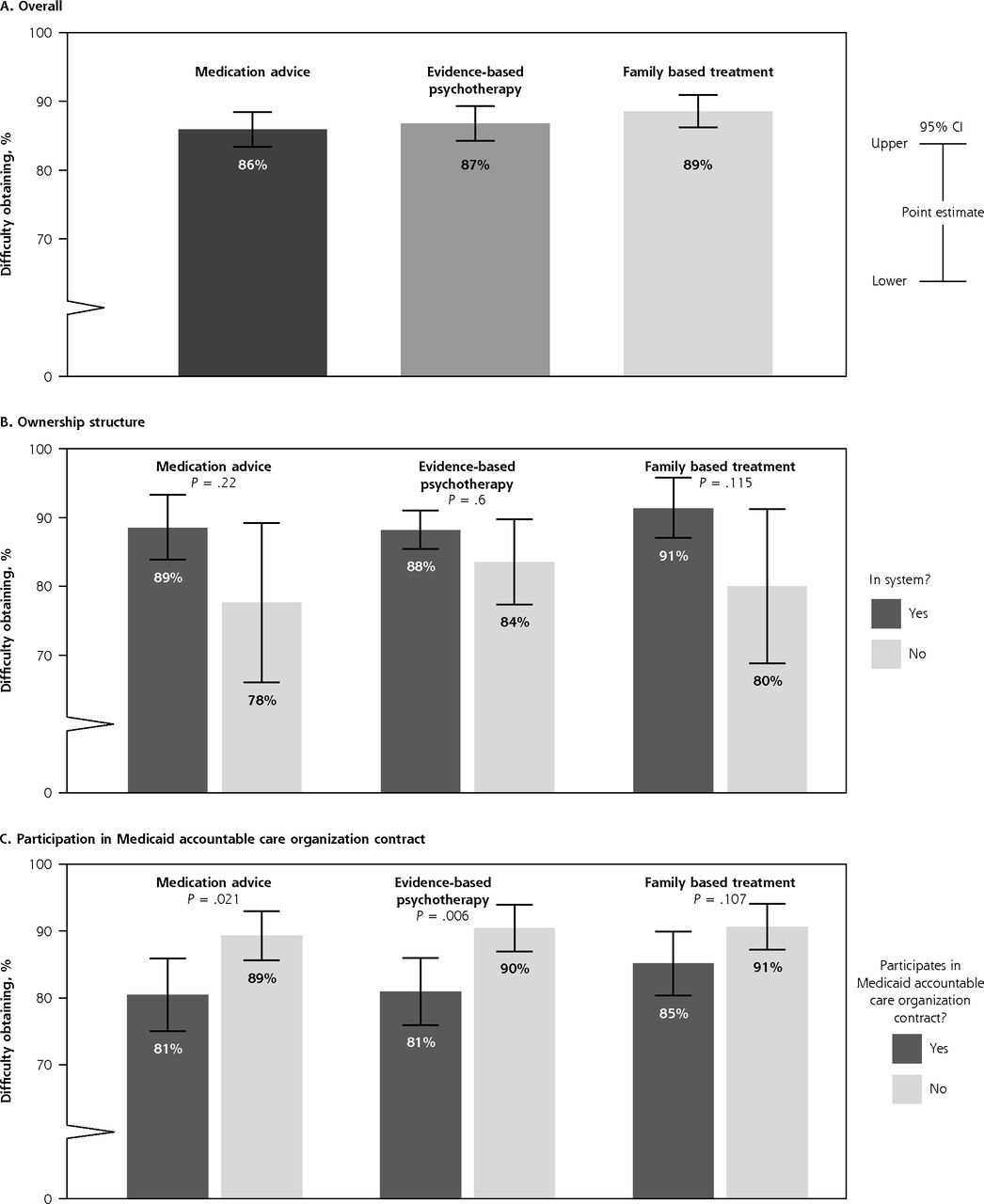
RESULTS More than 85% of practices found it difficult to obtain help with evidence-based elements of pediatric behavioral health care. Adjusting for practice attributes, the percent experiencing difficulty was similar between system-owned and independent practices but was less for Medicaid ACO participants for medication advice (81% vs 89%; P = .021) and evidence-based psychotherapy (81% vs 90%; P = .006); differences were not significant for family-based treatment (85% vs 91%; P = .107).
CONCLUSIONS Most multiphysician practices struggle to obtain advice and services for child behavioral health needs, which are increasing nationally. Future studies should investigate the source of observed associations.
- accountable care organizations
- behavior
- child
- psychotherapy
- therapeutics
- Medicaid
- pediatrics
- primary health care
INTRODUCTION
In the United States, behavioral health problems such as depression, anxiety, other mental illness, or substance use disorders are increasing among children, and this trend is expected to extend beyond the COVID-19 pandemic.1-9 When used appropriately, psychotropic drugs, evidence-based psychotherapy, and family-based treatments are cornerstones of effective treatment10-13 but are challenging to deliver broadly given the ongoing national shortage of child behavioral health professionals.14-16 Primary care practices are at the frontline of delivering pediatric behavioral health services because they provide a familiar, nonstigmatizing context in which behavioral health issues can gain attention.1,17,18
Several randomized trials and systematic reviews found that primary care practices can deliver high-quality, evidence-based behavioral health care for children if practices establish collaborative relationships with behavioral health professionals (psychiatrists, psychologists, therapists) or formally integrate such experts into their practices.19-21 However, we do not know how easily practices can cultivate such relationships outside of participating in a clinical trial.20,22-28 According to the latest nationally representative survey on this issue, completed in 2004-2005, two-thirds (67%) of primary care physicians reported being unable to obtain high-quality outpatient mental health services for their patients,29 but that survey did not distinguish child from adult behavioral health services.29
Meanwhile, physician practices have been undergoing dramatic changes in organization that might have put behavioral health personnel in closer organizational proximity to primary care physicians. Practices have grown in size, adopted team-based models of care,30-32 joined other practices, or have been bought by health systems.33-35 Today more than in the past, primary care practices are more likely to belong to larger organizations that might, in theory, directly employ clinicians with behavioral health expertise or have other types of clinicians (eg, patient navigators) who can help obtain behavioral health services for patients when needed.
Contemporaneously, practices have been engaging in alternative payment models that might support practices’ efforts to test new models of care, especially those that prioritize ongoing management of chronic conditions over that for acute, self-limited disease.36 Such payment models can benefit patients with behavioral health conditions directly if behavioral health conditions are of focus within contracts (eg, Medicaid accountable care organization [ACO] contracts)37,38 or indirectly via more general practice improvements (eg, the Centers for Medicare and Medicaid Services’ [CMS] Comprehensive Primary Care Plus [CPC+] programs).39 Although alternative payment models tend to be designed with adults in mind, adult-oriented, value-based ventures can have positive spillover effects on pediatric care quality.40-43 If practices are striving to improve, their pediatric care might improve too.
We hypothesized that most practices in the United States find it difficult to obtain the behavioral health advice and services needed to care for children with behavioral health disorders and that practices owned by health systems and practices participating in alternative payment models might report less difficulty obtaining this care.
METHODS
Study Design and Data Sources
This national cross-sectional study focused on 1,410 multiphysician primary and multispecialty care practices that cared for children and responded to the 2017-2018 National Survey of Healthcare Organizations and Systems (NSHOS) questions regarding difficulty obtaining services for children with behavioral health service needs.44,45 The NSHOS drew a stratified random sample of physician practices from IQVIA’s OneKey database, a repository of US physicians, practices, hospitals, and systems and the ownership relationships among these entities.46,47 Multiphysician practices were defined as those with ≥3 primary care physicians (family medicine, internal medicine, geriatrics, general practitioner). The NSHOS posed questions about practices’ organizational structures, capabilities, and care processes using multiple modes (mail, telephone, Internet) to reach leaders within practices. Respondents were medical directors, physician managers, and practice managers. Of the 4,976 practices that the NSHOS sampled, 2,333 (46.9%) responded, and 2,190 (44.3%) were confirmed as being in the sample frame—multiphysician primary care or multispecialty practices with at least 3 primary care physicians (general practice, family practice, internal medicine, or geriatrics).44,45 We included 1,410 multiphysician primary and multispecialty care practices that answered all 3 child-related behavioral health questions, had information available on Medicaid ACO contract participation, had a zip code that could be mapped to rural-urban commuting areas, and had an ownership relationship that fit our ownership categories.44-46 Supplemental Appendix 1 presents additional information on practice sample selection and item nonresponse. This study was approved by Dartmouth College’s Committee on the Protection of Human Subjects, which waived documentation for informed consent.
Primary Outcomes
After presenting respondents with a definition of behavioral health (“behavioral health includes depression, anxiety, other mental illness, or substance use disorders”), the NSHOS asked practice leaders, “How difficult is it to obtain: (i) medication advice from a child psychiatrist or psychiatric nurse practitioner; (ii) evidence-based psychotherapy; and (iii) family-based treatment?” Responses of “very difficult,” “somewhat difficult,” and “slightly difficult” were characterized as “difficult” relative to “not at all difficult” after the distribution of responses was reviewed.
Practice Attributes
Supplemental Appendix 2 presents detailed variable definitions and sources for each practice attribute below.
System vs Independent Practice Ownership
Because in theory, system-owned practices might have access to a larger network of pediatric behavioral health professionals either within the practice itself or at other practices within the same system, we evaluated how system ownership was associated with our primary outcomes. As in prior research,48 we used the OneKey database to classify practice ownership into the following 4 mutually exclusive types: (1) independent practices, with no ownership relationships beyond the practice itself, (2) medical group practices, owned by an organization that owns ≥2 practices but no hospital, (3) simple system practices, owned by an organization that owns practices and ≥1 hospital, and (4) complex system practices, owned by an organization that itself owns ≥1 medical group or system (ie, a system within a system). Practices were considered system owned if they were owned by medical groups, simple systems, or complex systems; otherwise practices were considered independent.
Practice Size and Workforce
We used OneKey data to determine practice size (total number of clinicians, total number of physicians) and physician specialty. We achieved this by mapping National Provider Identifiers to a taxonomy based on the American Board of Medical Specialties. We identified the following 3 groups of physicians, each with slightly different training related to pediatric behavioral health: (1) primary care physicians who are trained in pediatrics and frequently care for patients aged 0-18 years (family medicine practitioners, obstetrician-gynecologists, medicine-pediatrics physicians), (2) general and child psychiatrists, and (3) general and specialty pediatricians (who are trained to identify and manage child behavioral health issues). The total number of nonphysician clinicians (nurse practitioners, physician assistants, licensed social workers) could be counted, but we lacked the necessary information to further define their roles in practices as being directed toward behavioral health.
Orientation Toward Socioeconomically At-Risk Patient Populations
Because practices that serve a large share of socioeconomically at-risk patients can develop clinical expertise in the care of children with behavioral health conditions and corresponding infrastructures and workflows, we used the NSHOS to characterize practices’ revenue sources (percentage of total annual practice revenue coming from commercial payers, Medicare, Medicaid, or other sources [eg, self-pay]), whether revenue from Medicaid was in the top quartile (ie, >25%) across practices, whether a practice had federally qualified health center (FQHC) or FQHC look-alike status, and whether a practice was located in a rural zip code (using the rural-urban commuting area classification method).49
Participation in Payment or Delivery Reform Initiatives
The NSHOS asked, “Has your practice ever participated in any of these payment and delivery reform initiatives?” Practices were provided the following list of options: primary care improvement and support programs, pay for performance programs, capitated contracts with commercial health plans, Medicaid ACO contracts, and commercial ACO contracts. If practices answered, “Yes, currently” we counted them as participating in the corresponding initiative, and placed those answering “Yes, previously but not now” or “No, never” in the reference group. CMS CPC+ participation was ascertained by linking respondents of the NSHOS survey to participant lists published by CMS; both lists share practice attributes (eg, name, location, etc).50
Statistical Analysis
We used descriptive statistics to describe the distribution of practice attributes across the 4 practice ownership types (Table 1). For unadjusted analyses, significant differences across ownership types were determined using F-statistics for continuous variables and χ2 tests for categorical variables, setting significance at P < .05.
Practice Attributes by Ownership Structure
We estimated the adjusted percent of practices reporting difficulty obtaining services for children with behavioral health disorders. Separately, for each behavioral health service examined, we fit mixed-effects generalized linear models (ie, linear probability models) estimating whether a practice reported difficulty obtaining that service as a function of practice ownership type (medical group, simple system, complex system vs independent) and practice participation in a Medicaid ACO. Models controlled for practice size, CPC+ program participation, orientation toward socioeconomically at-risk populations, and practice workforce characteristics as specified in Table 2. Models also included an indicator for the state in which a practice is located, to account for underlying state-by-state differences in behavioral health resources and Medicaid state policies.51,52 To account for the hierarchical nature of the data (practices are nested within systems), models included a random intercept for each health system (or medical group). All estimates were weighted to be representative of the stratified sample frame and to account for survey nonresponse.47 We performed our analyses using Stata 15 (StataCorp LLC). For ease of presentation, we also used estimates from the models described above to compare adjusted outcomes for all system-owned practice types combined (medical group, simple, or complex system) to independent practices.
Adjusted Percentage-Point Difference Compared With Referent in Difficulty Obtaining Pediatric Behavioral Health Advice and Services
RESULTS
Practice Attributes
Of the multiphysician practices caring for children, 26.0% were independent practices, 17.4% belonged to medical groups, 15.8% were members of simple systems, and 40.8% were members of complex systems (Table 1). For almost all attributes examined, system-owned practices differed significantly from independent practices. System-owned practices (medical group, simple, or complex) tended to be larger, more likely to employ psychiatrists and general pediatricians, and more likely to participate in a delivery or payment reform initiative. Independent practices and simple systems were more likely to receive large shares of revenue from Medicaid (ie, top quartile across practices), to be located in rural zip codes, and to be located in the South. The percent of practices with any pediatric-trained primary care physicians did not differ significantly by ownership type. There appeared to be more differences among system-owned practices than between system-owned practices relative to independent ones with respect to annual practice revenues from commercially insured sources and practice locations in the Northeast and West.
Difficulties Obtaining Psychiatric Advice and Related Behavioral Health Services
Adjusting for the practice characteristics shown in Table 2, most practices (>85%) found it difficult to obtain pediatric behavioral health services, regardless of service type (Figure 1; Supplemental Appendix 3). The percent experiencing difficulty did not differ significantly between system-owned and independent practices, but practices participating in a Medicaid ACO reported less difficulty obtaining medication advice (80.5% vs 89.3%; P = .021) and evidence-based psychotherapy (81.0% vs 90.4%; P = .006); the difference was not significant for family-based treatment (85.1% vs 90.6%; P = .107).

Difficulty obtaining pediatric behavioral health services, by service type.
In multivariate models including the attributes shown in Table 2, the presence of behavioral health expertise within practices showed no significant associations with difficulty obtaining pediatric behavioral health medication advice or related services. Similarly, participants in CMS’ CPC+, an alternative payment model targeting primary care practices, were no less likely to have difficulty obtaining such services.
Notably, in adjusted analyses, practices in rural locations had significantly greater difficulty obtaining pediatric behavioral health advice and related services relative to their nonrural counterparts. These practices were more likely to have difficulty obtaining all 3 types of behavioral health services examined—medication advice, evidence-based psychotherapy, and family-based treatment by +15.2 (P = .002), +11.7 (P = .005), and +9.3 (P = .021) percentage points, respectively (Table 2). Lastly, relative to independent practices, medical group practices were more likely to have difficulty obtaining family-based treatment by +12.3 percentage points (P = .049).
DISCUSSION
In this nationally representative sample of multiphysician practices in the United States, practice leaders rated how difficult it was for their practices to obtain the advice and services needed to deliver evidence-based treatment for children with behavioral health disorders. We document 3 main findings.
First, most practices—more than 85%—reported difficulty obtaining help caring for pediatric behavioral health conditions.19-21 This exceeds the 67% noted in the most recent comparable study based on a 2004-2005 survey; however, the 2004-2005 study did not distinguish child from adult behavioral health services.29 The present finding is concerning because rates of childhood anxiety, depression, self-injurious behavior, and suicide were already increasing before the current COVID-19 pandemic, which has exacerbated this preexisting trend.1-9 The difficulty levels also varied in an expected way; given the scarcity of child behavioral health professionals, it makes sense that delivering evidence-based treatments and family-based therapy might be viewed as more difficult to obtain than medication advice.14-16 Despite advances in our understanding of the biologic basis of behavioral health conditions, improved treatments, and federal legislation designed to expand access to behavioral health care (eg, the Mental Health Parity and Addiction Equity Act of 2008; the Patient Proection and Affordable Care Act of 2010), significant barriers to behavioral health treatment remain. For example, behavioral health experts are still scarce, and treatments are often unaffordable.53 If primary care practices are to fulfill their role as the nation’s frontline for identifying and treating or referring patients with pediatric behavioral health disorders, the present study finds practices in clear need of collaborative or integrative relationships with behavioral health experts.
Second, we found that system-owned practices fared no better than independent practices in terms of the difficulty they experience in obtaining pediatric behavioral health advice and services. Even though system-owned practices are far larger and more likely to have personnel (eg, psychiatrists, nurse practitioners, physician assistants) who could serve as behavioral health resources, the present study does not support the notion that ownership alone can extend the reach of scarce behavioral health resources to the primary care frontline. Future studies should examine whether these associations change as new organizational forms mature to develop integrative or collaborative behavioral health service models.
Third, comparing otherwise similar practices, Medicaid ACO participants reported less difficulty than nonparticipants in obtaining needed services. This finding warrants further investigation to understand whether joining a Medicaid ACO can cause this type of change, or whether organizations are better equipped to link children to needed services for other reasons. It could be that Medicaid ACO contract participation merely reflects how attuned practices are to the behavioral health needs of their patient populations rather than facilitating the creation of collaborative or integrative relationships needed to deliver behavioral health care.37 Early evidence suggests that all of the above are possible,54-56 but more empirical work is necessary to understand this finding.
The present study has several limitations. First, the main outcome was a self-reported measure from practice managers, and it might not reflect how frontline clinicians would rate their experiences. However, the practice perspective is important for prioritizing practice-wide clinical quality improvement efforts. Second, we assessed a single cross-section in time (2017-2018); however, these years are critically important from a payment reform perspective—they capture the timeframe in which Medicaid-sponsored ACO efforts started proliferating and follow after 5 to 10 years of experience with primary-care–focused alternative payment models sponsored by commercial payers and Medicare.57-59 Third, although the sample frame of multiphysician primary care or multispecialty practices did not include physician practices focused on pediatrics, the results remind us of how frequently family medicine physicians care for children, especially as they enter adolescence.60 Fourth, limited power to detect effects might have obscured greater difficulty obtaining care by complex system practices compared with independent practices. Fifth, in this cross-sectional study, observed associations could reflect unobserved confounding (eg, practice finances). Still, this national study provides a rare but important glimpse into the services being provided to pediatric patients by family medicine physicians in the United States. Going forward, it is important to appreciate the crucial role that diverse multispecialty primary care practices play in caring for children, especially in rurally located practices.
In summary, this first-of-its-kind study set in the United States offers a glimpse into the accessibility of clinical care for children’s behavioral health as American health care undergoes broad changes in structure and incentives. The news is sobering—the challenge of providing behavioral health treatments for children is a hefty one, and much progress needs to be made.
Acknowledgments
This paper is dedicated to the memory of Lisa Schwartz, MD, MS, our remarkable partner, colleague, and friend who proposed this research. Dr Schwartz died before publication of this article.
Footnotes
Conflicts of interest: authors report none.
Read or post commentaries in response to this article.
Funding support: This study was funded by the Agency for Healthcare Research and Quality U19 HS024075-05 (principal investigator: E. Meara).
Disclaimer: The statements, findings, conclusions, views, and opinions contained and expressed in this article are based in part on data obtained under license from IQVIA information services (OneKey subscription information services 2010-18; IQVIA Inc; all rights reserved). The statements, findings, conclusions, views, and opinions contained and expressed herein are not necessarily those of IQVIA Inc or any of its affiliated or subsidiary entities. The American Medical Association (AMA) was the source for the raw physician data; statistics, tables, and tabulations were prepared by the authors using data from the AMA Physician Masterfile.
Previous presentation: This study was presented at The Dartmouth Institute’s U19 Center of Excellence on Comparative Health System Performance; November, 2019; Lebanon, New Hampshire.
- Received for publication December 17, 2020.
- Revision received May 21, 2021.
- Accepted for publication June 21, 2021.
- © 2022 Annals of Family Medicine, Inc.




{kind=link}