
Abstract
PURPOSE The coronavirus disease 2019 (COVID-19) pandemic is an unprecedented global public health crisis. Mass vaccination is the safest and fastest pandemic exit strategy. Mass vaccination clinics are a particularly important tool in quickly achieving herd immunity. Primary care physicians have played a crucial role in organizing and running vaccination clinics. In this special report, we synthesize existing guidelines and peer-reviewed studies to provide physicians with practical guidance on planning and implementing COVID-19 mass vaccination clinics.
METHODS PubMed, Ovid MEDLINE and Embase were used to search for relevant literature using search terms that included COVID-19, mass vaccination, and best practice. We also identified and analyzed national and international guidelines.
RESULTS Forty-six relevant articles, reports, and guidelines were identified and synthesized. Articles included mass vaccination clinic guidelines and studies before and during the COVID-19 pandemic. Key considerations for COVID-19 mass vaccination clinics include leadership and role designation, site selection, clinic layout and workflow, day-to-day operations, infection prevention, and communication strategies.
CONCLUSIONS Planning and implementing a successful COVID-19 mass vaccination clinic requires several key considerations. Primary care plays an important role in organizing clinics and ensuring populations made vulnerable by social and economic policies are being reached. Ongoing data collection is required to evaluate and continuously improve COVID-19 mass vaccination efforts. As the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccine rollout occurs in various countries, research will be required to identify the main factors for success to inform future pandemic responses.
INTRODUCTION
In just 2 years, the pandemic of coronavirus disease 2019 (COVID-19) has resulted in 380 million confirmed cases and 10 million deaths, with numbers continuing to rise.1 Public health measures played an important role in reducing the spread of this novel virus but have also had enormous social and economic impacts worldwide.2 Achieving herd immunity is the only pandemic exit strategy.3
Estimates of the herd immunity threshold range from 55% to 82%.4 For wildtype SARS-CoV-2, which has a fatality ratio of approximately 1 in 100 cases,5 achieving herd immunity through natural infection would result in significant morbidity and mortality. For example, a herd immunity threshold of 55% would translate into ~43 million global deaths and would take years to achieve. During the 3 major flu pandemics of the 20th century, herd immunity was achieved through multiple waves of natural infections over 2 to 5 years.6 Mass vaccination provides the safest and fastest way of achieving herd immunity, especially with surges due to variants of concern.
The rollout of vaccines for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) to the general population represents the largest mass vaccination campaign in history.7 As of winter 2022, over 10 billion doses had been administered worldwide.8 Primary care has been called upon to organize and implement mass vaccination clinics, both in primary care clinics and in nontraditional settings. For example, primary care played an important role in the rapid vaccine rollout in Israel9,10 and the United Kingdom,11 supporting proactive practice outreach to at-risk individuals, organizing local clinics, and tracking adverse events. As the demand for mass vaccination decreases in these countries, the role of primary care physicians will continue and grow. For instance, in the United States, COVID-19 vaccination clinics are increasingly transitioning from large venues like convention centers to primary care clinics.12
Despite the progress made over the past year, the role of mass vaccination clinics in achieving herd immunity is not achieved yet. Although 61% of people worldwide have received at least 1 vaccine dose, only 10% of people in low-income countries have.8 Also, only 13% of the world population has received a booster dose.8 Primary care will continue to be essential in organizing mass vaccination clinics in large venues and in primary care settings.
To our knowledge, no study has yet synthesized peer-reviewed studies and public health guidelines to summarize best practices for organizing mass vaccination clinics. This special report aims to provide easy-to-follow, practical guidance for those planning and implementing COVID-19 mass vaccination clinics.
METHODS
Search Criteria for Study Inclusion and Selection
We sought reports, manuals, and peer-reviewed papers that addressed the planning of mass vaccination clinics before and in context of the COVID-19 pandemic. Studies that involved human participants and reported in English were included.
We searched PubMed, Ovid MEDLINE, and Embase for publications from January 1, 1947 through November 25, 2020. We used the COVID-19 filter adapted for search strategies created by Library and Knowledge Services of the National Health Services,13 and used the following search terms: coronavirus disease 2019, COVID-19, severe acute respiratory syndrome coronavirus 2, SARS-CoV-2, mass vaccination, mass immunization, campaign* or surveillance or best practice* or policy* or principle* or standard* or clinic* or strategy* or planning. We also searched for official national and international guidelines for mass vaccination clinics and included COVID-19–specific guidelines as they emerged.
Data Collection and Analysis
We used the Appraisal of Guidelines, Research and Evaluation reporting checklist to guide assessment of reports and to synthesize what is known about planning and implementing mass vaccination clinics.14 A simple analytical framework, Search, AppraisaL, Synthesis and Analysis (SALSA) was employed,15 and a narrative summary of the results is presented.
RESULTS
A total of 46 relevant articles, reports, and guidelines were identified and synthesized. Of the 26 peer-reviewed studies identified (Supplemental Appendix 1) 14 were conducted in the United States, 6 in Canada, 3 in Australia, 1 in China, and 2 involved more than 1 country. Of the 20 guidelines identified, 2 were from the World Health Organization, 7 from the United States, 4 from Australia, 3 from the United Kingdom, 2 from Canada, and 2 from New Zealand (Supplemental Appendix 2).
Initial Steps in Planning Clinics
The initial steps in organizing a mass vaccination clinic are to establish leadership and coordinate clinic operations. Experienced leadership is an important factor in a vaccine program’s effectiveness.16–18 These clinics require close coordination across all levels of government and among public health agencies, external organizations, and community partners. An organization and coordination team, in which members represent a wide array of expertise,19 may help to identify opportunities for collaboration, and to negotiate agreements in advance (eg, for supplies, clinic sites, human resources).17
The Public Health Agency of Canada recommends selecting sites based on location, accessibility, and amenities.17 Preferred locations are known to the community and allow for large crowds. Consider high-density areas and proximity to targeted populations.17 Sites accessible by public transport and vehicles will allow patients and supplies to easily reach the site.17 The US Department of Defense also recommends choosing a venue with sufficient equipment and rooms (eg, for storage, management of medical emergencies).20
Facilities and Layout
Venues must have a large area that allows for physical distancing and lines.20 Guidelines agree that spaces can be outdoors (eg, sports arena, open field), or indoors when well-ventilated (eg, schools, university campuses, shopping malls, conference centers).16,17,19 Separate entry and exit for unidirectional flow prevents infections and improves efficiency.17,19,21
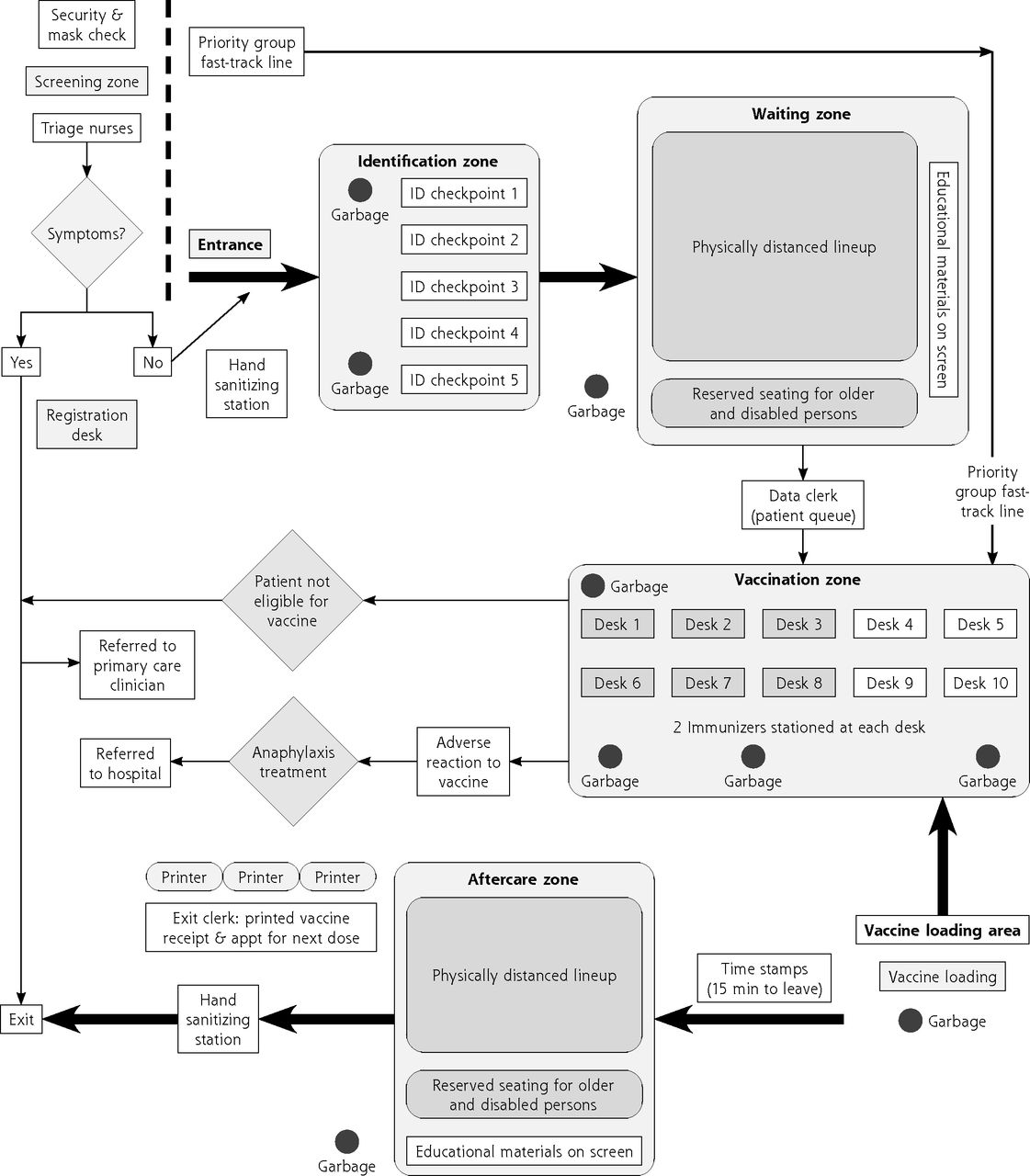
The clinic layout will vary depending on the site, but should follow a logical, unidirectional flow.17,21,22 Defined areas include (1) greeting and screening, (2) registration, (3) immunization, (4) after care, and (5) exit (see Figure 1 for an example).17,20,23–27

Example of a mass immunization clinic layout.
Appt = appointment; ID = identification; min = minutes.
Note: Adapted fron Toronto Public Health; personal correspondence.
At the immunization station, the immunizer assesses and vaccinates the patient. The person performing the procedure must obtain consent, pursuant to the relevant legislation. Consent can be implicit (eg, patient rolls up sleeve) or explicit.28 Typically, for patient safety, the same immunizer would prepare and administer the vaccination.28 In the setting of a mass vaccination clinic, however, syringes can be preloaded for efficiency.17,28
Practices on post-vaccination monitoring vary by jurisdiction and vaccine type. Guidelines from the United States, Canada, and Australia suggest observing patients for 15 minutes post vaccination.17,19,20,29 For patients with a history of anaphylaxis, a 30-minute observation period is recommended.30,31 Public Health England makes similar recommendations for recipients of Moderna and Pfizer vaccines, but requires no observation period for the AstraZeneca vaccine.32,33 In contrast, New Zealand’s Ministry of Health recommends monitoring all for 20 minutes.34
A report on other vaccines, before COVID-19, found that adverse events following immunization were uncommon, and that most reactions are mild.35 As such, 2 studies on influenza mass vaccination clinics suggest that replacing a clinic’s monitoring area with a first aid station is safe, increases the clinic’s capacity and efficiency, and reduces the risk of viral transmission.24,36 For the 2020 influenza season, New Zealand’s Immunisation Advisory Centre recommended reducing the post-vaccination wait from 20 minutes to 5 minutes to assess for any immediate adverse events following immunization due to the risk of exposure to infectious disease in waiting rooms. Patients were considered low risk if they had no history of allergic reactions, were accompanied, were able to contact emergency services, and were able to seek medical advice.37
Day-to-Day Operations
Refining clinic operations during and after each mass vaccination event maximizes efficiency25 and may reduce staffing and hours required.21 Use of simulation analysis can aid the planning and assessment of clinic functions and guide improvements.23,38–41 Identifying and avoiding patient bottlenecks may improve flow and reduce infection risk.20 Use of a reservation system is crucial in controlling crowds and ensuring appropriate clinic volume.19,25 Patients may prefer to reserve their appointment by telephone or online.25
Staff acting as traffic guides can improve operations by directing patients through the one-way flow, to the appropriate line or station, and out of the clinic through the designated exit.19,25 Vests or uniforms improve efficiency by allowing staff to be easily identified.21 Guidelines suggest that individuals with disabilities and families with children be directed to a designated vaccination line.17,19,25 Registration and immunization time may vary by age and special needs (eg, adults and seniors take 32 to 45 seconds longer to register than children, presumably due to their more complex medical histories).39 Consider express lanes as appropriate (eg, for health care workers).17
Infection Prevention and Control
SARS-CoV-2 transmission is expected to occur in mass vaccination clinics and requires infection control measures.23,42
The following infection control measures are recommended during the COVID-19 pandemic16,17,19:
Use online processes for registration and screening
Provide specific appointment times
Perform screening before admittance. Clients who screen positive are ineligible for vaccination and should be encouraged to reschedule their appointment in 2 weeks.31
Establish staff as traffic guides to manage crowds and ensure unidirectional patient flow
Limit the total number of individuals in the clinic at any given time
Arrange separate hours or areas for individuals at increased risk of COVID-19 complications
Select large clinic facilities to allow physical distancing
Use outdoor spaces where possible
Use well-ventilated areas
Disinfect clinic areas frequently
Ensure availability of hand sanitizer and hand washing stations with soap and water at entrances and vaccination stations
Maintain 1 to 2 meters between patients
Require that all individuals in the facility wear face coverings
Require that staff wear a mask throughout their shift
Train staff on appropriate hand hygiene. Gloves are not necessary for vaccines, including SARS-CoV-2 vaccines.
Training
All immunizers must be trained on vaccination protocol.22,43
Receiving sufficient and clear training is important for immunizers working in pandemic mass vaccination clinics.44 Ensuring that all staff members receive standardized training before working in the clinic has been shown to reduce the number of staff members and hours required.21
Options for training include online videos and just-in-time training. Online training allows for convenient access and standardization.19 For example, the CDC’s web-based training course, You Call the Shots, covers the most recent guidelines in vaccine practice.45 Just-in-time training on the day of the clinic has been shown to be useful in mass vaccination clinics.18,25
Staff should be informed of their clinic shifts and roles in a timely manner to enable them to prepare for and feel competent in their roles.44 Communications may include meetings before each clinic day, briefings before and after shifts, team huddles, bulletin boards, and teleconferences.17
Staffing
Studies vary on the roles and quantity of staff. Staff often include immunizers (eg, nurses, physicians, paramedics, pharmacists), community health workers, volunteers, administrators, security personnel, and information technology specialists.17,19,25 Specialized or additional staff may be needed for certain populations (eg, interpreters). Additional staff may be sourced internally by redirection from other programs or from external agencies.17 Clinics may be more successful with experienced and knowledgeable immunizers who can clearly and confidently articulate the safety and benefits of vaccination.18 To reduce the burden on health care during the pandemic, volunteers can effectively replace health staff for all non-clinical roles.24
Adverse Events Post-immunization
Adverse events must be reported in accordance with jurisdictional protocols. The evidence shows that most adverse events following immunization are minor (eg, injection site reactions).46 Urgent medical issues following immunization include anaphylaxis and syncope. Anaphylaxis after SARS-CoV-2 mRNA vaccines is rare, with 80% occurring within 15 minutes of mRNA vaccine administration, and 89% occurring within 30 minutes.47 Anaphylaxis is also rare with the AstraZeneca vaccine.29 Although rare, anaphylaxis can be fatal. Health care workers trained in the assessment and management of anaphylaxis should be readily available at the clinic.30 Clinics should have procedures in place to manage anaphylaxis, including medical directives for delivering the medication and transport to a health facility.
Presyncope and syncope are anxiety-related events that can occur after any vaccination process.48 Prevention strategies include giving patients a drink or snack, providing reassurance, and having the patient sit or lie down while being vaccinated.49 Risk factors include younger age groups and a prior history of similar events.48 Syncope typically occurs during or within 2 minutes of immunization. If an episode occurs, the patient should be placed in a supine position with their legs elevated,50 and be monitored until they regain consciousness.49 Most events resolve with supportive care.48
Documentation
Vaccination must be documented on the patient’s legal health record: product, lot number, dose, route of administration, site, clinician name, and date. In mass vaccination clinics, electronic systems are superior to paper-based systems due to cost-effectiveness and rapid availability of data that improves clinic efficiency and accuracy.51,52
Immunizers must provide proof of vaccination53 and may encourage patients to keep a digital vacination record.54
Supplies and Waste
Many guidelines offer checklists of suggested supplies.17,19,55,56 Supplies include but are not limited to surgical masks, face shields, face coverings for patients, emergency medical kits, infection control supplies (eg, biohazard containers, hand hygiene stations), syringes, needles, alcohol swabs, and vaccine information statements. Sharps should be disposed in containers that are closable, puncture-resistant, leak-proof, and labeled.56
Vaccine Storage
Vaccine supply and storage problems are common.18 Vaccine coordinators may be required to ensure that vaccines are stored and handled correctly.57 Vaccines must be stored at the correct temperature in a safe and secure location. Guidelines recommend that vaccines be shipped directly to the clinic site, or transported using portable refrigerated containers.22,43 Protocols for delays in vaccine delivery and compromised vaccinations should be in place.26 Upon arrival at the vaccination clinic the cold chain must be maintained and temperature should be documented at least twice during each clinic shift. The Pfizer-BioNTech SARS-CoV-2 vaccine must be stored between −80°C and −60°C, but may be stored between −25°C and −15°C for 2 weeks.58 Vials may be thawed and stored in the refrigerator (2°C to 8°C) for 31 days.58 The Moderna SARS-CoV-2 vaccine is stored between −25° and −15°C, but can be refrigerated at 2° to 8°C for 30 days before first use.59 Both vaccines must be stored in the original carton to protect from light. Product monographs should be referenced for details and updates regarding vaccine storage, stability, and handling.58,59
Communication Considerations
Vaccine hesitancy is a significant barrier to vaccine uptake.60,61 Ensuring SARS-CoV-2 vaccine confidence is crucial.60–62 Education campaigns highlighting vaccine safety and efficacy should begin before and continue during the clinic rollout.60 Primary care clinicians need to address the uncertainties and mixed public messaging regarding the duration of immunity to the virus, risk of reinfection, and appropriate dose scheduling. Public concerns and new information will continue to emerge rapidly throughout the vaccine rollout. In response, communications should be coordinated, timely, and transparent.63 Transparency about what is known and what is not known improves trust.64 Social media can be used to quickly address misinformation and to respond to concerns in real time.60
Primary care physicians are crucial for countering vaccine hesitancy.65,66 Patients concerns should be discussed. Concerns about SARS-CoV-2 vaccine safety include new vaccine technology, rapidity of the development and approval process, and possible side effects.60 Studies show improved vaccine uptake and confidence when family physicians and nurses strongly recommend vaccination, share personal anecdotes, and speak confidently about safety and benefits.18,60
Clincal promotion should be targeted and scaled to the number of vaccines available.26 Core messages include eligibility and clarity (eg, priority groups, requiring appointment or prescreening), clinic logistics (eg, location, hours), and vaccination information (eg, benefits, safety, myths).17,26 Patients should be asked to wear appropriate clothing (eg, short sleeve shirts) to improve clinic efficiency and to eat before arrival to reduce fainting.17 Marketing strategies and materials will vary based on the targeted group (Table 1). For example, vaccine clinics targeting university students used e-mails, coffee cups, sidewalk chalk messages, and newspaper articles.67,68
Examples of Materials, Media, and Formats for Communication With the Public
Vaccine acceptance and uptake in previous pandemics varied by community and race.69 Barriers included mistrust of the health care system and community-level informal messaging that ran counter to public health campaigns.60,69 To ensure health equity, campaigns must involve trusted community leaders and organizations, and include linguistically and culturally sensitive materials.60,70
DISCUSSION
In this special report, we synthesized peer-reviewed studies and guidelines on mass vaccination clinics to provide practical guidance for primary care clinicians as they plan, implement, and expand efforts. Key considerations include management, logistics, infection control, human resources, adverse events post-immunization, documentation, supplies and waste, vaccine storage and handling, and communications. This report also provides suggestions for anticipated challenges (eg, vaccine supply, vaccine hesitancy).
Mass vaccination clinics are crucial for quickly immunizing a population and ending the pandemic. Compared with scheduled doctor’s visits, mass vaccination clinics are more cost effective,71 have shorter wait times, and patients are more likely to receive vaccine information statements.72 Traditional (eg, hospitals, long-term care, retirement homes, physicians’ offices, pharmacies73,74) and nontraditional settings (eg, community centers, arenas, stadiums, drive-through clinics39,41) should be used in a coordinated fashion to vaccinate the greatest number of people in the shortest period of time.72 In this pandemic, family doctors have played a huge role outside of traditional settings—organizing and setting up vaccination clinics, working as immunizers, and building vaccine confidence in patient encounters.
As the proportion of the population with immunity grows, and mass vaccination clinics transition from large venues to primary care clinics, themes for improving efficiency and reducing viral transmission risk remain the same. Strategies include online screening, registration, and appointment reservations; a unidirectional clinic layout, and uniformed staff to direct flow; continuously refining operations, including identifying and avoiding patient bottlenecks; and providing standardized staff training and regular briefings.
Certain considerations were not found in the literature. For example, although studies support the importance of scheduled appointments in ensuring efficiency and an appropriate clinic turnout,25 appointments may not be feasible for certain populations, such as individuals experiencing homelessness. Moreover, as more people are vaccinated and the number of scheduled appointments decrease, clinics will transition to a majority of walk-in appointments.75 In refining operations, physicians may find that a mix of walk-in and scheduled appointments are most appropriate for their community. Therefore, practices may vary based on local status of the pandemic.
Practices also vary based on the clinic’s targeted population. Health equity has been central to the COVID-19 mass vaccination approach. Partnering with trusted community leaders and organizations improves vaccine confidence and uptake, particularly in historically disadvantaged groups.76 Partners with existing and trusted relationships allow communities to self-determine their approach, address specific vaccine concerns, ensure access for hard-to-reach populations, and arrange transport for those in need of assistance.70,77
In determining best practices, many guidelines were in harmony. Recommended post-vaccination monitoring periods varied by state, virus, vaccine, and patient characteristics. Organizers should follow the recommendations of their jurisdiction, given the novelty of the SARS-CoV-2 vaccines.
This report is limited by the restriction to English language. The English-speaking countries analyzed are high income countries. Many best practices, however, such as unidirectional flow and the use of traffic guides, can be implemented regardless of setting. The report is also limited by the emergent nature of the COVID-19 pandemic. New evidence is continuously emerging. As mass vaccination clinics roll out worldwide, in more diverse settings, further research will be required to determine factors crucial to running successful clinics and to inform ongoing and future pandemic responses.
Acknowledgments
We thank Nazi Torabi, an information specialist with Health Sciences Library, Unity Health Toronto, for assistance with literature searches.
Footnotes
Conflicts of interest: authors report none.
Funding support: Drs Pinto and Kiran are supported as Clinician Scientists by the Dept of Family and Community Medicine, Faculty of Medicine, at University of Toronto and St Michael’s Hospital, and by the Li Ka Shing Knowledge Institute, St Michael’s Hospital. Dr Kiran is the Fidani Chair in Improvement and Innovation at University of Toronto. Dr Pinto is also supported by a fellowship from the Physicians’ Services Incorporated Foundation and as the Associate Director for Clinical Research at University of Toronto Practice-Based Research Network (UTOPIAN). The opinions, results, and conclusions in this article are those of the authors and independent from any funding sources.
Previous presentation: Some findings and ideas were presented at rounds for the Public Health and Preventive Medicine Residency Program, University of Toronto, and are based on approaches to mass vaccination developed at Toronto Public Health.
- Received for publication May 13, 2021.
- Revision received August 13, 2021.
- Accepted for publication September 8, 2021.
- © 2022 Annals of Family Medicine, Inc.




{kind=link}