
Abstract
Vaccination delivery and efforts to counter vaccine hesitancy have become focal issues for family medicine teams as the COVID-19 pandemic has evolved. Conducting action research, our team developed an interactive web-based guide to improve clinical conversations around a broad range of vaccine hesitancies presented by patients. The paper presents a step-by-step account of the guide being codesigned with family physicians—its targeted end users—in a process that included validation interviews; role-play interviews; and user-tested design. The validation interviews sought to understand the pragmatic realities of vaccine hesitancy in family medicine clinical practice relative to relevant psychological theories. The role-play interviews drew out conversational strategies and advice from family physicians. The principles of motivational interviewing—an evidence-based approach to vaccine hesitancy conversations that supplements information deficit approaches—were used to codesign the content and layout of the guide. User counts, stakeholder engagement, and web-based analytics indicate the guide is being used extensively. Formal evaluation of the guide is presently underway.
Originally published as Annals “Online First” article.
INTRODUCTION
COVID-19 has brought new twists on familiar challenges in family medicine. At both societal and clinical levels, COVID-19 has brought new twists and urgency to familiar challenges in family medicine. At the societal level, politically and socially determined inequalities in COVID-19 outcomes have reminded us of abiding disparities in access to care1-3 and the rise of COVID-19 vaccine hesitancy has brought into question the very way we citizens conduct our political lives.4 In primary care’s operational context, family physicians have encountered the familiar policy challenges of integrating community-based responses with those of public health and acute care5-8 and ensuring broader systems recognize primary care’s response potential.9,10
Central among these new twists have been efforts to contain the COVID-19 pandemic through vaccination.11,12 From delivering mass vaccinations13,14 to countering vaccine hesitancy,15-17 family physicians, with their well-known trusting relationships with patients, are key to improving vaccine uptake. With the literature indicating that the decision to be vaccinated is a “trust-sensitive” one,18-20 our team of “action researchers”21 identified an urgent need to bolster family physicians’ understandings of the varied and emerging factors that contribute to COVID-19 vaccine hesitancy.
In January 2021, as family physicians became de facto COVID-19 vaccine counselors, we at the University of Calgary learned there was a need for a clinical resource that would provide focused and dynamic support for that counseling work. In this article, we describe the codesigned knowledge mobilization that led to the launch of a Vaccine Hesitancy Guide (“the guide”) (https://www.vhguide.ca). The guide is a pragmatic support tool for clinical conversations in primary care about COVID-19 vaccine hesitancy. It was codesigned with, and is tailored to the needs of, family physicians as they talk with patients who present a range of vaccine hesitancy.
BACKGROUND
The psychology literature indicates there are at least 3 types of vaccine hesitancy.22 Specifically, vaccine hesitancy has been shown to originate in personally held: (1) socio-political orientations and identities,23-25 (2) basic fears,26 and (3) trauma.27,28 Commitments to libertarian or “anti-science” identities have been shown to be at the root of a generalized mistrust of the government and health institutions that promote and deliver vaccines.17,29,30 Overconfidence,31 coupled with short- and long-term personal safety fears around being vaccinated,32 and previous traumas, have been identified as key factors in individuals’ vaccine hesitancy33 with anti-vaccine activists particularly exploiting these trauma-based hesitancies.34 Traumas negatively affecting vaccine confidence may not just have occurred during individual interactions with health systems, but with formal institutions and structural racism more broadly.35 Efforts to counter these political, fear, and trauma-based hesitancies have often focused on education efforts that follow an “information deficit model.”36 Under the deficit model, vaccine counselors provide facts, scientific detail, or information to their patients.37 Research, however, has shown that relying on facts in hesitancy conversations that are, from the patient’s perspective, about anxieties and values rather than scientific information, often backfires.38 Vaccine hesitancy and its related behavior, vaccine refusal, have been shown to be complex culturally informed activities in which people deploy conversational tactics aimed at avoiding rather than actively opposing advice to vaccinate.39 As such, working with patients to get to the core issues takes time and trust.
“Vaccine hesitancy” is sometimes used to refer to delays in vaccination that do not stem from psychological states, concerns about safety, or previous traumas, but instead are related more to disparities in access to vaccines and vaccination sites.40 Because our resource does not target these broader access-to-care issues, we did not focus on access as a part of our hesitancy framework.41 While there is a place for family medicine in setting up COVID-19 vaccination clinics, and so improving access,13,14 our approach assumed these geographically and culturally specific access-to-care issues had been dealt with, and that family physicians needed conversational strategies to help them address vaccine hesitancy rooted in psychological states and previous traumas.40
METHODS
In January 2021, our team contacted family physicians to investigate if, and how, the types of vaccine hesitancy identified in the literature were presenting in adult patients in the Canadian jurisdictions of Alberta, British Columbia, Ontario, Saskatchewan, and Yukon. This preliminary research leveraged our ongoing relationships with the family medicine community established over the course of the pandemic.42-44 As such, our initial recruitment strategy was opportunistic and relied on existing research networks. We shifted to snowball sampling, and also actively solicited participants by contacting medical associations and departments of health in the named jurisdictions. We constituted ourselves as action researchers undertaking “collective, self-reflective inquiry [alongside] participants so they can understand and improve upon the practices in which they participate….”21 Indeed, we took an explicit “alongsider” approach to codesigning the research and its knowledge mobilization products.45 Alongsider action research positions the researcher as neither an insider, nor an outsider, but rather an ally in the production of innovative processes and practices.46 As action researchers,21 our focus was on shortening the cycle between investigation and pragmatic knowledge mobilization. The specific questions we went into the field with were:
What types of vaccine hesitancy are family doctors encountering in their daily practice?
How are these types linked to, or separate from, the political narratives, fears, and traumas identified in the literature?
How are family physicians responding to the different types of vaccine hesitancy they encounter?
How are more effective conversational strategies for engaging patients with vaccine hesitancy best organized and presented in a web-based tool?
To answer these questions, we took a 4-step approach (Table 1). Each of the steps focused on ensuring the buy-in of our family physician participants, and, ultimately, the usefulness and usability of the guide. Specifically, the hypothesized types of hesitancy generated out of our literature review were presented in the validation interviews (n = 10) as possibilities that were open to, and in need of, clinical interpretation. Thus, the validation interviews focused on understanding if and how the origins of vaccine hesitancy—the political views, fears, and traumas in the psychology literature—were manifesting in everyday clinical conversations about the vaccines.
Methodological Steps Taken to Turn Theoretical Concepts Into Pragmatic Conversational Strategies for the Guide
As clinically valid, and not merely hypothetical, types of hesitancy emerged from those interviews, we began developing role-play profiles and moved to validate them. Validation involved checking with family physician participants on whether the role-play profiles we were developing “felt real.” We asked if the profiles sounded like patients they or their colleagues had encountered in practice, or could imagine encountering in future patient visits. In this way, as we shifted to conducting role play interviews (n = 15) we were simulating the speech and attitudes of patients that our participants had encountered, expressing our validated typology as discreet vaccine hesitancy personas. This attention to clinical experience was central to achieving buy-in from our participants. As with simulated patients in the medical education context,47 those physicians responded in the role-play interviews as if they were in a clinical conversation with a given type of hesitant patient. These interviews aimed to collect conversational strategies family physicians were using to counter a broad range of hesitancies. We diverged from the traditional use of simulated patients to evaluate or assess learners, instead using simulation to gather and document emerging conversational strategies and clinical wisdom from family physician participants.
Both the role-play interviews, and our analyses of the resulting transcripts were structured by the principles of motivational interviewing (MI).48 The MI approach, which is concordant with the principles of “trauma-informed care”49 and specifically designed to overcome the limitations of the “information deficit model,” seeks to work with patients’ particular perspectives, values, and motivations. Motivational interviewing techniques have been effective at improving the uptake of vaccines among hesitant patients in acute care and community contexts.50,51 Using an MI framework, we would debrief multiple times during a role-play interview, reflecting with the physician participant on how a particular vaccine hesitancy–countering strategy they were deploying was more or less aligned with MI best practices. In this way, MI principles were used to identify, discuss, and refine highly effective conversational strategies during the interviews. “Highly effective” in this sense was determined out of an iterative mix of MI best practices filtered through individual clinicians’ experiences and instincts. We again used MI principles as we analyzed and coded the interview transcripts to extract and categorize examples of strategies and “clinical pearls” that would be included in the guide.
This approach led us to develop 4 touch points for engaging with patients in culturally safe, respectful ways. Those 4 touch points emphasize the physician’s role as an ally on the patient’s health journey rather than as an expert with evidence to present. They are also consistent with best practices in vaccine deployment52 and are described in the guide as the “EAASE steps.” That acronym stands for: Engage, Affirm, Ask permission, then Share information, and Evoke. The guide’s content provides users with practical examples of family doctors: engaging with their hesitant patients; affirming their patient’s concerns; asking them for permission before sharing new information and perspectives on the concerns; and evoking future states that motivate patients to reconsider their hesitancy. While there is much room for interpretation across these steps, and so adaptation to an individual clinician’s style, key operational definitions grounded in MI include:
approaching engagement as an informed and empathetic ally rather than a detached expert
enacting allyship by finding common areas of experience and concern rather than entering into confrontation
approaching affirmation as an exercise in first understanding and then validating whatever concerns, regardless of how foreign they may seem, a patient brings to their vaccination decision
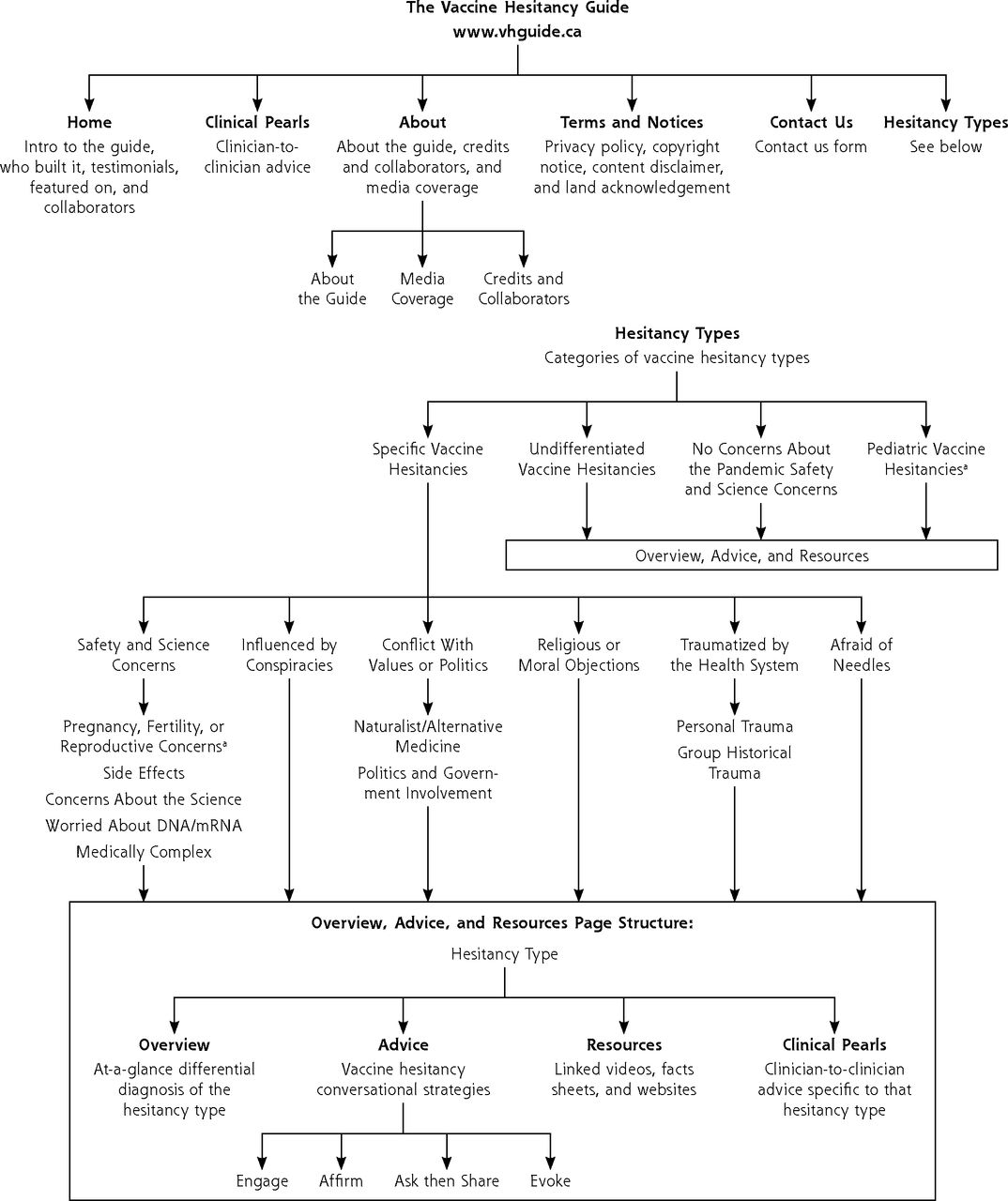
Based on data gathered from these validation and role-play sessions, we organized the guide’s content in direct collaboration with an information designer and web developer. Our content, design, and development teams worked iteratively with our data to design a high-fidelity prototype interface, and then deploy it as a live website. To ensure the guide’s prototype designs were user friendly and intuitive for targeted end users (eg, primary care clinicians in Canada), we conducted user tests (n = 7) with family physician participants. These test sessions involved a supervised Zoom call with our information designer, who guided participants through specific tasks on the proposed interface, asking them to provide feedback while doing so. This feedback was used to iterate the final design of the guide. The overarching principle behind the guide’s design was that a user should proceed toward specificity and density of information as they navigated the site, rather than beginning their journey on pages saturated in text. As such, data were organized to reinforce the differences between the types of hesitancy identified in Stage 1. Similarly, standardized overview, advice, and resource pages were developed for each type of hesitancy, and the EAASE steps were used to break effective conversational strategies into easily readable portions. Figure 1 presents a site map highlighting this user-tested information architecture.
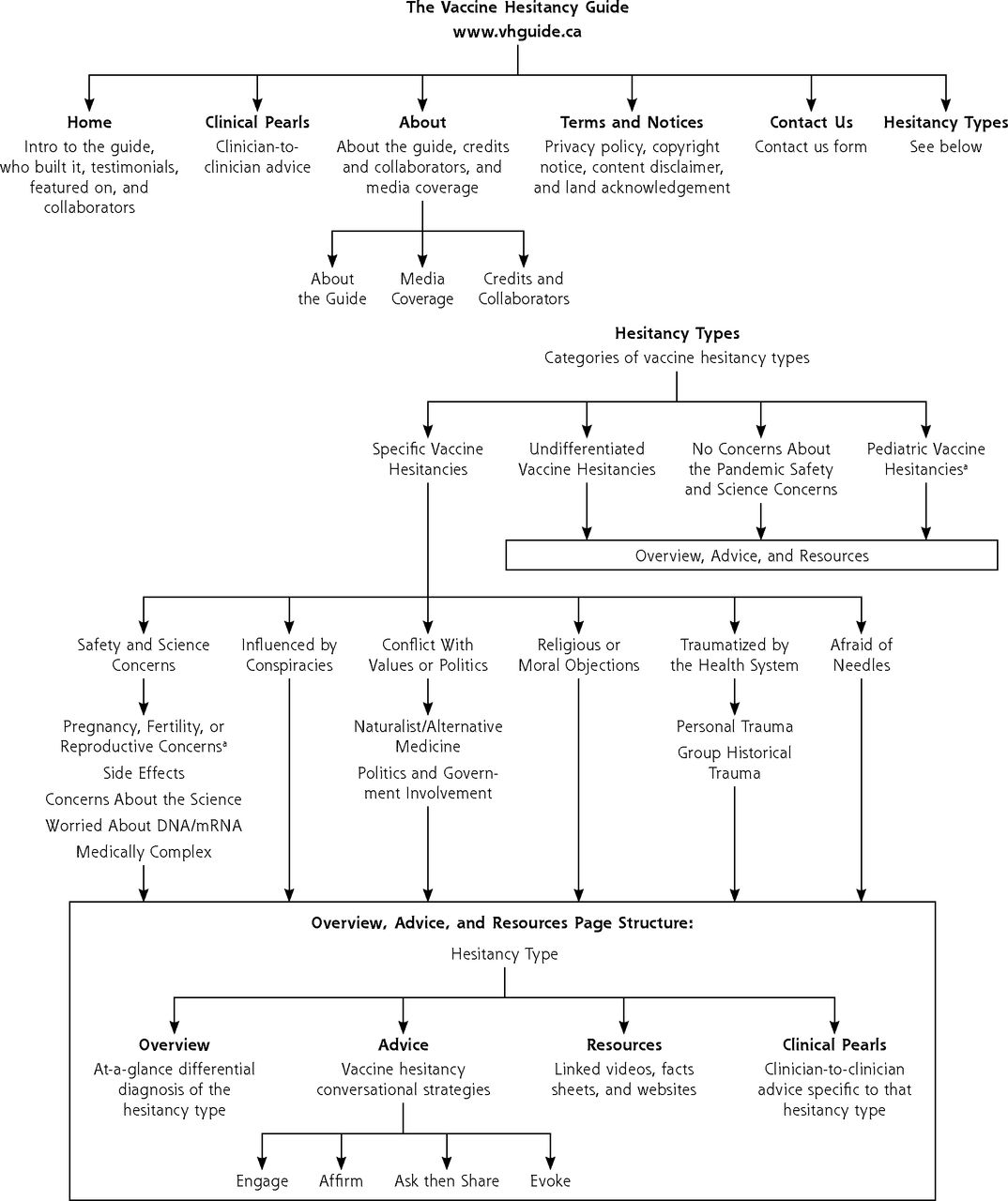
Full sitemap displaying the information architecture of the guide.
DNA = deoxyribonucleic acid; mRNA = messenger ribonucleic acid.
a These pages contain not just Overview, Advice, and Resources, but also their own Clinical Pearls sections.
RESULTS
Our role-play interviews revealed 32 differentiated presentations of vaccine hesitancy commonly encountered in family medicine clinics across Canada. These hesitancy types formed the basis of our qualitative codebook (Supplemental Table 1), which was used to structure our data and build the guide’s website. The guide was launched on July 12, 2021 with support from a range of family medicine dissemination partners, including: The Alberta College of Family Medicine,53 the primary care–focused Centre for Effective Practice in Ontario,54 the Innovation Support Unit at the University of British Columbia,55 the Alberta56 and Ontario Medical Associations,57 and the 19 to Zero project.58 Our partners are committed to supporting the long-term development and successful deployment of the guide. As of January 2022, the guide has had over 21,000 users and 147,000 page views.
Content on the guide continues to be updated to reflect emerging priorities and vaccine hesitancy trends. For instance, it now includes conversational material on how to counsel patients who reference the Centers for Disease Control and Prevention’s (CDC’s) Vaccine Adverse Event Reporting System (VAERS), Ivermectin, and breakthrough infections—all topics which were not initial concerns included in the original release. These updates have been informed by additional, follow-up interviews (n = 5) with primary care clinicians following the same structure and methodological steps from our original validation and role-play sessions, using new hesitancies identified by our team through news and social media. Although users have always been able to contact us with suggestions or questions, we are presently conducting a formal evaluation of the guide that deploys user surveys and leverages website usage analytics.
DISCUSSION
We used a 4-stage participatory “action research” approach to build a dynamic COVID-19 vaccine hesitancy resource for primary care clinicians. This resource was built alongside family physicians, helping to validate theoretical vaccine hesitancy literature in the clinical realities of the pandemic. Using an adapted version of “simulated patients” in role-playing sessions, our team sourced vaccine counselling strategies and advice from a wide range of physicians. The result is a web-based resource that has been used by thousands of primary care clinicians around the world. Further evaluation is needed to understand the guide’s impact on vaccine hesitancy discussions in primary care, and patient vaccine confidence.
Footnotes
Conflicts of interest: authors report none.
Funding support: Portions of this research were funded by the Canadian Natural Science and Engineering Research Council (Encouraging Vaccine Confidence in Canada competition).
- Received for publication September 18, 2021.
- Revision received February 1, 2022.
- Accepted for publication March 2, 2022.
- © 2022 Annals of Family Medicine, Inc.




{kind=link}