
Abstract
PURPOSE Physicians’ interruptions have long been considered intrusive, masculine actions that inhibit patient participation, but a systematic analysis of interruptions in clinical interaction is lacking. This study aimed to examine when and how primary care physicians and patients interrupt each other during consultations.
METHODS We coded and quantitatively analyzed interruption type (cooperative vs intrusive) in 84 natural interactions between 17 primary care physicians and 84 patients with common somatic symptoms. Data were analyzed using a mixed-effects logistic regression model, with role, gender, and consultation phase as predictors.
RESULTS Of the 2,405 interruptions observed, 82.9% were cooperative. Among physicians, men were more likely to make an intrusive interruption than women (β = 0.43; SE, 0.21; odds ratio [OR] = 1.54; 95% CI, 1.03-2.31), whereas among patients, men were less likely to make an intrusive interruption than women (β = −0.35; SE, 0.17; OR = 0.70; 95% CI, 0.50-0.98). Patients’ interruptions were more likely to be intrusive than physicians’ interruptions in the phase of problem presentation (β = 0.71; SE, 0.23; OR = 2.03; 95% CI, 1.30-3.20), but not in the phase of diagnosis and/or treatment plan discussion (β = −0.17; SE, 0.15; OR = 0.85; 95% CI, 0.63-1.15).
CONCLUSIONS Most interruptions in clinical interaction are cooperative and may enhance the interaction. The nature of physicians’ and patients’ interruptions is the result of an interplay between role, gender, and consultation phase.
- office visits
- primary care
- interactions
- communication
- interruptions
- verbal behavior
- physician-patient relations
- professional practice
- practice-based research
INTRODUCTION
Physicians’ interruptions during medical visits have been found to occur after an average of just 18 seconds.1 These instances of overlapping talk that break the rule of one speaker at a time have long been considered as negative actions that inhibit patients’ symptom presentation and participation.2–4
Evidence shows that interruptions can be supportive or cooperative in the interaction, however.5–14 A cooperative interruption preserves the content and flow of the interaction. For example, the physician may establish common ground by requesting clarification, as in this exchange (text enclosed by slashes indicates overlapping speech and “eh” indicates a brief hesitation):
Patient: … whether it has to do with balance that eh / that / …
Physician: … / how / long—how long does it take?
In contrast, an intrusive interruption impairs the content and flow of the interaction, for example, when the physician changes the topic, as in this exchange:
Patient: I already read that it / would / …
Physician: … / how long / did you need to wait?
Intrusive interruptions, such as topic changes and disagreements, are perceived as more negative, typical interruptions than cooperative interruptions, such as clarifications and agreements.15
In addition to the notion of interruptions as physicians’ ignorant actions, interruptions have long been associated with masculinity and male dominance,16–18 although others have questioned this direct link between gender and interruptions.19,20 With regard to specific types of interruptions in medical interaction, women have been found to make more cooperative interruptions than men, but no gender differences have been found for intrusive interruptions.6,7,11
Particular moments in a medical interaction may also predict the nature of an interruption.21 The phase of problem presentation and the phase of discussing a diagnosis and/or treatment plan are characterized by specific tasks and conversational goals for the physician and patient.21,22 The problem presentation phase is the only phase in which “patients are licensed to present their concerns in their own way.”22 The discussion of the diagnosis and treatment plan, on the other hand, is considered “the task of the physician, and as an area in which the physician has legitimate expertise.”22
A systematic analysis of cooperative and intrusive interruptions in various consultation phases of clinical practice interactions is lacking. In this study, we examined whether speaker role (physician vs patient) and speaker gender predict the type of interruption in these particular consultation phases.
METHODS
Of 393 primary care consultations about common somatic symptoms that were video recorded as part of the CATMUS (Clinical Assessment as Therapy in Managing Medically Unexplained Symptoms) study conducted in the Netherlands,23 we selected 84 consultations for the current study. We did so to match 4 gender dyads (with 21 consultations for each) on patient age, physician assessment of symptom origin (medically explained or unexplained), and consultation type (first or follow-up visit). Matching was done blind to the content of the interactions to prevent bias (Supplemental Appendix 1). The study was approved by a research ethics committee, and all physicians and patients gave written informed consent.
Physician and patient characteristics are shown in Table 1. The consultations were conducted by 17 Dutch primary care physicians (mean age = 44.3 years; SD, 11.3) and involved 84 patients (mean age = 55.1 years; SD, 14.9) with equal numbers of women and men. All physicians and patients self-identified as a woman or man, resulting in 4 gender dyad compositions.
Characteristics of Physicians and Patients
Consultation characteristics are shown in Table 2. On average, the consultations lasted 870 seconds (14.5 minutes), with a range from 275 seconds (4.5 minutes) to 2,091 seconds (almost 35 minutes).
Characteristics of Consultations, Overall and by Dyad Composition
For the analysis, we focused on the problem presentation phase and the diagnosis and/or treatment plan phase, given that they are characterized by particular tasks and goals for the physician and patient.21,22 We manually coded and analyzed interruptions occurring during these phases using both the video data and the transcript data to improve feasibility and reliability of the coding. The physician’s first exploring question was considered the start of the phase of problem presentation, for example, “How are you doing?” or “What can I do for you today?” or “So, what are we going to discuss?” This exploring question explicitly invited the patient to present symptoms and concerns in their own way. The start of the diagnosis and/or treatment plan phase was most often marked by the physician’s initial thoughts on a potential diagnosis and/or treatment plan. When patients presented new symptoms during this phase, these instances were considered as a (new) part of the problem presentation and coded as such.
We did not include in analyses interruptions during the opening, physical examination, and ending of the consultation. The opening phase and ending phase of consultations are often less medically oriented and may partly take place outside of the consultation room (eg, when the physician meets the patient in the waiting room). The physical examination phase is medically oriented, but usually takes place in another room, outside of the camera’s reach.
On average, the length of the 2 included phases combined was 683 seconds (almost 11.5 minutes), with a range from 85 seconds (nearly 1.5 minute) to 1,696 seconds (more than 28 minutes) (Table 2).
Coding Categories
Drawing from the literature, we defined interruptions as instances wherein a new speaker started talking during an audibly incomplete turn of the current speaker, which most often involved overlap of speech.24–26 We did not include instances of overlapping speech when the turn was potentially complete and thus relevant for speaker change.2 Backchannels and minimal responses that explicitly confirmed the listener’s role, such as “yeah,” “okay,” and “hmhm,” were not considered as full turns, and therefore not as instances of interruption.20,27 We did not include silent interruptions, that is, without overlap, as research has shown it is difficult to determine whether the current speaker is going to continue their incomplete utterance.28
We focused on interruptions by physicians and patients; interruptions made by others were not analyzed. Only 101 (4%) of the interruptions in our data were made by a third speaker, either a relative of the patient or a second primary care physician briefly entering the room. Because of this small proportion, we decided to focus on the physicians’ and patients’ interruptions only. We also did not include external interruptions, such as telephone calls or door knocks.12,29
Two independent coders (I.P. and Caya van Dijk) coded whether interruptions were cooperative or intrusive, and comparison of their results indicated substantial intercoder agreement (κ = 0.70). In Supplemental Appendix 2, we give examples of cooperative and intrusive interruptions, as well as their possible subtypes (eg, clarification),7 with instances from the data that were translated to English at the sentence level.
Procedure and Analysis
All physicians’ and patients’ utterances were divided into turn constructional units, that is, the smallest distinguishable linguistic speech segments, which can be single words, clauses, or full sentences.2,30 In the verbatim transcripts of the 84 consultations, we noted the exact time (from the start of the first consultation phase) and place (by means of square brackets) of the interruptions within the turn constructional units. Ten percent of the interruptions were coded by an independent second coder (Caya van Dijk).
We conducted analyses using R version 4.1.0, and RStudio version 1.4.1717 (the R Foundation). Data were analyzed using a mixed-effects logistic regression model for the binary dependent variable of interruption type (cooperative vs intrusive). To assess the effects of speaker role (physician vs patient), speaker gender (woman vs man), consultation phase (problem presentation vs diagnosis and/or treatment plan), and dyad type (mixed gender vs same gender) on the dependent variable, we conducted a 4 × 2 model with these predictors and their interactions as fixed effects. First, we specified a null model for random intercepts with the best model fit. We included the patient identification as a random intercept in the final model. Second, we added the predictors and interactions to the model, as well as covariates that were associated with the dependent variable (Supplemental Appendix 1). Covariates and interactions were excluded from the model if they did not improve the model fit. We used the Akaike information criterion to compare the goodness of fit of the various models, and to choose the final model. When we found a significant interaction between predictors, we performed stratified analyses.
RESULTS
Interruption Characteristics
All consultations had at least 1 interruption, with an average of about 29 interruptions per consultation. Of the 2,405 total interruptions identified, 1,994 (82.9%) were cooperative and 304 (12.6%) were intrusive. For the remaining 107 interruptions (4.4%), the type of interruption was unclear, most often because of inaudible speech.
Patients made 55.5% of all interruptions, 55.0% of cooperative interruptions, and 58.9% of intrusive interruptions. Physicians made the first interruption in 56% of the 84 consultations, an average of 36.3 seconds after the start of the problem presentation phase, and 89% of these interruptions were cooperative.
Predictors of Interruption Type
Table 3 shows results of the final mixed-effects logistic regression model for predictors of interruption type. The results revealed a significant main effect of speaker role whereby patients were significantly more likely than physicians to make an intrusive interruption (odds ratio [OR] = 3.17; 95% CI, 1.83-5.50). Furthermore, the model showed a significant main effect of speaker gender in that men were significantly more likely than women to make an intrusive interruption (OR = 1.67; 95% CI, 1.05-2.65). We also found a significant main effect of consultation phase whereby the odds of an intrusive interruption were significantly higher in the diagnosis and/or treatment plan phase than in the problem presentation phase (OR = 2.24; 95% CI; 1.46-3.43). The model did not reveal a significant effect of gender dyad type.
Predictors of Intrusive vs Cooperative Interruption Type
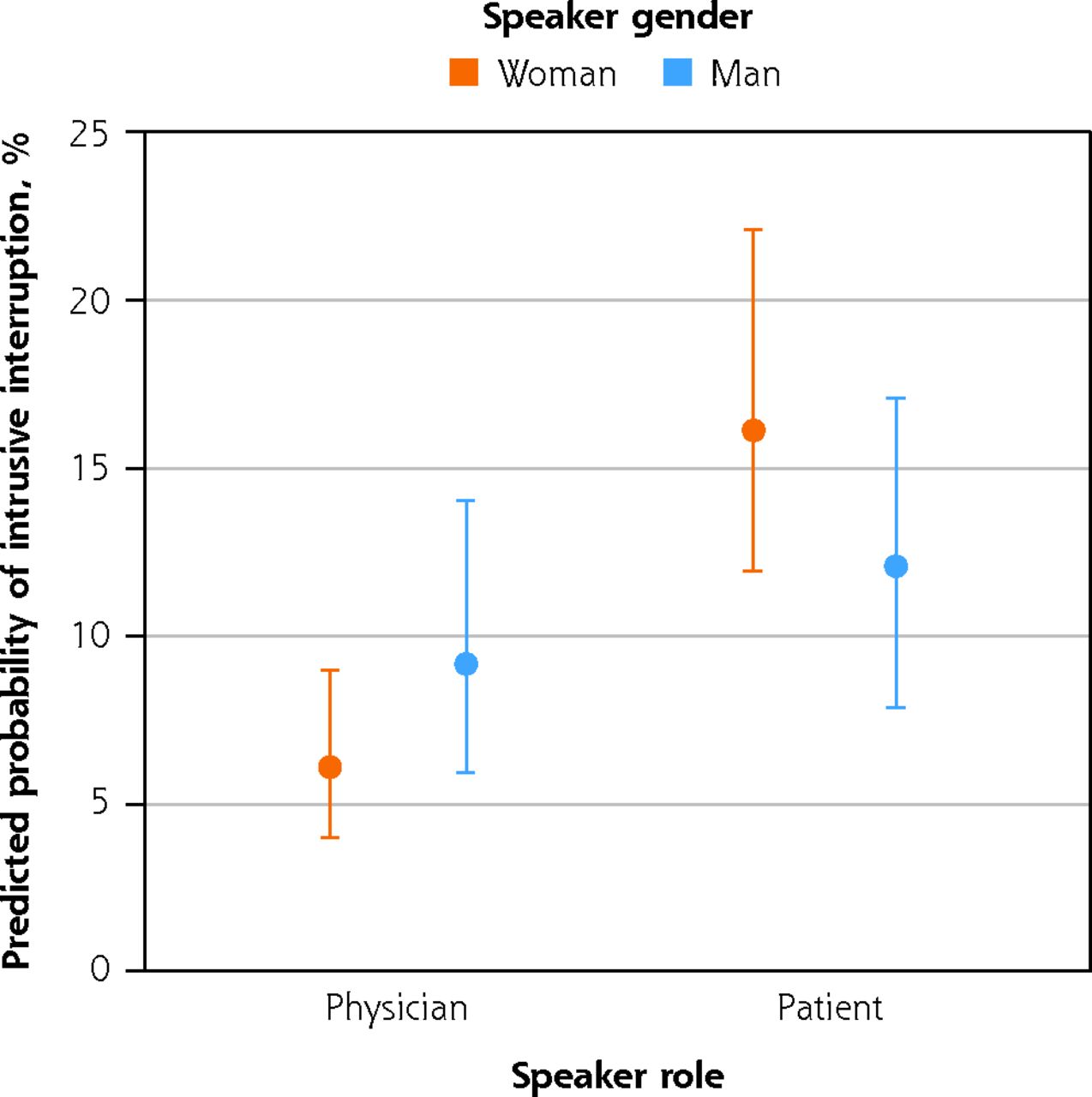
In addition, we found a significant interaction term whereby the type of women’s and men’s interruptions varied between physicians and patients (OR = 0.41; 95% CI, 0.22-0.77) (Table 3). Stratified analyses showed that in the physician group, men were more likely to make an intrusive interruption than women (β = 0.43; SE, 0.21; OR = 1.54; 95% CI, 1.03-2.31), whereas in the patient group, men were less likely to make an intrusive interruption than women (β = −0.35; SE, 0.17; OR = 0.70; 95% CI, 0.50-0.98) (Figure 1).

Predicted probability for intrusive interruption according to speaker role and speaker gender.
The model also revealed a significant interaction term indicating that the type of physicians’ and patients’ interruptions varied between consultation phases (OR = 0.44; 95% CI, 0.25-0.75) (Table 3). Stratified analyses revealed that in the problem presentation phase, patients’ interruptions were more likely to be intrusive than physicians’ interruptions (β = 0.71; SE, 0.23; OR = 2.03; 95% CI, 1.30-3.20), but this difference was not significant in the diagnosis and/or treatment plan phase (β = −0.17; SE, 0.15; OR = 0.85; 95% CI, 0.63-1.15) (Figure 2).

Predicted probability for intrusive interruption according to consultation phase and speaker role.
Lastly, we found a significant effect of patient’s age, whereby the odds of patients and physicians making an intrusive interruption were significantly higher with older patients (OR = 1.21; 95% CI, 1.06-1.38) (Table 3).
Table 4 shows numbers and percentages for the 2 types of interruptions by consultation phase, speaker role, and speaker gender.
Interruption Type by Consultation Phase, Speaker Role, and Speaker Gender (N = 2,298 Interruptions)
DISCUSSION
Although physicians’ interruptions of patients have long been considered intrusive actions that should be avoided,1,3,4 our findings demonstrate that most of the interruptions physicians make are actually not intrusive. Rather, our study provides empirical evidence for previously described, empirically untested intuitions that some interruptions are cooperative actions that may actually enhance the medical interaction.8
In slightly more than one-half of the consultations in our data, physicians made the first interruption, after an average time of 36 seconds, which is longer than the previously reported 18 and 23 seconds.1,3 The physicians in our study mainly interrupted patients to express understanding and support, or to ask for clarification, thereby aligning with the patients’ ongoing narration and thus with the patient’s role as the primary speaker. Hence, physicians’ cooperative interruptions in the initial phase of the consultation may actually improve, rather than hinder, the quality of communication.8,31–33
Speaker Role and Gender, and Phase
Our study is the first to provide a systematic analysis of when and how physicians and patients interrupt each other in clinical practice interactions. The findings show that patients interrupted physicians more frequently than vice versa, and also more often in an intrusive manner. Although patient participation in clinical consultations varies across cultures,34 our findings correct the intuitive assumption that it is mainly the physician who acts intrusively during medical interaction.1,3
To examine the association between gender and interruption behavior in clinical practice interactions, we analyzed interruptions in 4 gender dyad compositions.35–39 Our findings do not provide evidence for differences between mixed-gender dyads and same-gender dyads in interruption behavior in clinical consultations. This result indicates that the physicians in our data did not more frequently intrusively interrupt women’s stories than men’s,7,29 and that women physicians were not more often intrusively interrupted than men physicians.40 In our data, men physicians and women patients were most likely to make intrusive interruptions, and women physicians and men patients were most likely to interrupt in a cooperative manner. Regarding patients, these findings may indicate that women patients participate in medical interactions more assertively than men patients,41,42 although it could also be interpreted as a result of women patients feeling less heard and understood in medical interactions.43–45 With regard to physicians, our finding that women physicians used more cooperative interruptions than men physicians is in line with previous research on physicians’ patient-centeredness35,46 and supportive turn taking.6
Our study is the first to explore interruption behavior in 2 important consultation phases. Physicians and patients use interruptions for various purposes, which reflect the particular tasks and opportunities for each.21,22,47–49 Our findings showed that physicians were less likely than patients to intrusively interrupt the other in the phase of problem presentation, which indicates that the physicians in our study acknowledged the control of the patient in this initial and critical phase. On the other hand, in the phase of diagnosis and/or treatment plan discussion, physicians made almost as many intrusive interruptions as patients, which suggests more tension or time pressure, and a repeating exercise of authority in taking and keeping the conversational floor.50
Strengths, Limitations, and Future Directions
We conducted a quantitative analysis to investigate interruptions in a large data set of 84 clinical interactions, and we considered several relevant covariates such as consultation length and age. In our data, patients’ age played a role, which should be explored further in future research. With the present data, we cannot rule out the possibility that interruption type may be influenced by other factors, such as patient’s level of education,7,51 socioeconomic status and race,52 and severity of symptoms,7 and physician’s status and experience,6,29,53 which we consider to be relevant factors for future research. Likewise, studies could explore physicians’ experienced time pressure in consultations and the extent to which time pressure is associated with interruption behavior.54 Furthermore, we acknowledge that the 4 gender dyad compositions in our study do not represent all gender identities. We therefore encourage future research on interruption patterns in clinical consultations to attempt including nonbinary and transgender patients and physicians. Additionally, we recommend future studies to examine how patients react to cooperative and intrusive interruptions with or without an explicit excuse or explanation,8 and to explore the effects of interruptions on patient outcomes such as feeling of control, satisfaction, and recall.29,33,55–57
Furthermore, it should be noted that the interruption patterns found in our data—primary care consultations in the Netherlands—may differ from interruption patterns in other health care settings and (non–Western European) cultures, and interactions in other languages.11,58,59 Also, our data were collected 7 years ago. Future studies are encouraged to analyze interruption patterns in more recently collected data.
Although the use of video recording in clinical consultations does not affect the behavior of physicians and patients,60,61 we cannot know to what extent our findings represent physicians’ and patients’ interruptions in consultations that are not video recorded. Likewise, we did not analyze interruptions made during the phase of physical examination. Future studies may consider the use of audio recording when collecting data on interruptions in clinical interaction. Finally, we hope that this article will inspire future research, education, and practice to consider the more fine grained nuances of interruptions in medical interaction.
Conclusions
Physicians’ and patients’ interruptions are often cooperative actions that may actually enhance the clinical interaction, and subsequently the physician-patient relationship. Especially in the phase of problem presentation, physicians’ interruptions to show agreement or to ask for clarification acknowledge the patient in their role as primary speaker, recognize the content of the patient’s story, and demonstrate engagement in the interaction.
Acknowledgments
We thank Caya van Dijk (Radboud University Nijmegen, The Netherlands) for her assistance with transcribing and coding a subset of the data. We would also like to thank prof dr Judith Rosmalen (Rijksuniversiteit Groningen, The Netherlands) for commenting on the final draft of the manuscript.
Footnotes
Conflicts of interest: authors report none.
Funding support: This study was supported by ZonMw (funding No. 849200013).
Disclaimer: The views expressed are solely those of the authors and do not necessarily represent official views of the authors’ affiliated institutions or funder.
- Received for publication February 1, 2022.
- Revision received April 15, 2022.
- Accepted for publication May 4, 2022.
- © 2022 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}