
Abstract
PURPOSE Cerebral palsy (CP) and spina bifida (SB) are pediatric-onset disabilities. Adults living with CP/SB are in a greater need of preventive care than the general population due to their increased risk for chronic diseases. Our objective was to compare White/Black and White/Hispanic inequities in the use of preventive services.
METHODS Using 2007-2017 private claims data, we identified a total of 11,635 adults with CP/BS. Of these, 8,935 were White, 1,457 Black, and 1,243 Hispanic. We matched health-related variables (age, sex, comorbid conditions) between White adults and those in each minority subpopulation. Generalized estimating equations were used and all models were adjusted for age, sex, comorbidities, income, education, and US Census divisions. Outcomes of interest were: (1) any office visit; (2) any physical/occupational therapy; (3) wellness visit; (4) bone density screening; (5) cholesterol screening; and (6) diabetes screening.
RESULTS The rate of recommended services for all subpopulations of adults with CP/SB was low. Compared with White adults, Hispanic adults had lower odds of wellness visits (odds ratio [OR] = 0.71, 95% CI, 0.53-0.96) but higher odds of diabetes screening (OR = 1.48, 95% CI, 1.13-1.93). Compared with White adults, Black adults had lower odds of wellness visits (OR = 0.50, 95% CI, 0.24-1.00) and bone density screening (OR = 0.54, 95% CI, 0.31-0.95).
CONCLUSIONS Preventive service use among adults with CP/SB was low. Large White-minority disparities in wellness visits were observed. Interventions to address physical accessibility, adoption of telehealth, and increased clinician education may mitigate these disparities, particularly if initiatives target minority populations.
INTRODUCTION
The population of individuals living with disabilities is increasing.1–3 Cerebral palsy (CP) and spina bifida (SB) are the most common congenital conditions that cause permanent movement disorders.4,5 Cerebral palsy refers to a group of brain disorders that affect muscle and body movement.4 Spina bifida is a condition characterized by incomplete development of the brain, spinal cord, or meninges.5 The severity of disability caused by CP or SB is variable, with some individuals needing lifelong care and others having a relatively minor impairment.4,5 The incidence and prevalence of secondary chronic illnesses such as osteoporosis6–8 and cardiometabolic conditions9–11 are disproportionately higher among adults with CP/SB, compared with adults without the disability. Given the higher burden of noncommunicable diseases in these populations, the use of preventive services is important to reduce both the risks of developing secondary conditions and associated complications.
Patients with disabilities are at higher risk for multimorbidity and adverse health events than the general population.12–15 Furthermore, systematic racism16—economic deprivation, provider bias, and living in segregated/disadvantaged areas—makes it more challenging for some racial/ethnic subpopulations of adults with disabilities to access preventive care.17,18 As the lifespan of individuals with congenital disabilities increases, timely access to preventive services plays a critical role in maintaining health and independence.19–23 Most of the health services research related to congenital disabilities has been focused on the pediatric population. There is a pressing need to assess the use of preventive services among adults with CP/SB.24,25 Prior research has revealed disparities in access to health care and health outcomes for disadvantaged minorities living with disabilities.26,27 Having health insurance coverage is an important first step in enabling the use of preventive care,28,29 and as an enabling factor has been associated with reducing racial/ethnic inequities in access to care.30–32 For example, among individuals with SB, those who are privately insured are more likely to have bowel and bladder continence and less likely to have pressure sores.26 Health insurance coverage alone, however, is not sufficient to achieve racial/ethnic equity in care coordination and access.33 For instance, despite having coverage via Medicare, older Black and Hispanic adults are less likely than White adults to get the flu vaccine.34 There is a void in the literature pertaining to racial/ethnic inequities in use of preventive services among privately insured adults living with congenital disabilities. Although disabilities affect people of every race/ethnicity and economic class, disadvantaged groups experience greater inequities in health and access to care.25
In this study, we used private insurance claims data from 2007-2017 to assess racial/ethnic disparities in use of preventive services among adults living with CP/SB. To conduct this study, we quantified the definition of racial/ethnic inequity as defined by the National Academy of Medicine: a difference in treatment or access not justified by the differences in health status or preferences of the groups.35 We anticipated low rates of preventive service use among all subpopulations of adults with CP/SB.36 We hypothesized that White adults with CP/SB would have higher preventive service use, compared with minority adults with CP/SB. The rationale for our hypothesis came from prior research that revealed the intersectionality of disability and systematic racism exacerbates access barriers to care or health outcomes for disadvantaged groups.25
METHODS
Data Source
Data from the 2007-2017 Clinformatics Data Mart (OptumInsight) were used for this report. The database contains deidentified national private insurance claims data of over 80 million people having commercial insurance. All health care encounters including inpatient, outpatient, and emergency visits were included throughout participants’ enrollment period. The study was deemed exempt by the University of Michigan Institutional Review Board.
Sample Selection
We included individuals aged 18 to 64 years at the time of their insurance enrollment. All persons with 4 years of continuous enrollment were included. To allow a 4-year follow-up, the starting years were 2007 through 2013.37 We used the International Classification of Diseases, Ninth Revision, Clinical Modification (Supplemental Table 1) to select patients that had a diagnosis of CP/SB during a 1-year look back period. Co-occurring CP and SB is considered clinically infeasible and we excluded a small number of people who had both diagnoses. We retained White (8,935), Black (1,457), and Hispanic (1,243) individuals with CP/SB and excluded 3,111 whose race/ethnicity was missing/unknown. Asian individuals were excluded due a small sample size of only 295 persons. Supplemental Figure 1 presents the schematic flow diagram of our sample.
Outcomes
We calculated the use of the following preventive services for White, Black, and Hispanic adults during their 4-year enrollment: (1) any office visit; (2) any physical/occupational therapy; (3) wellness visit; (4) bone density examination; (5) cholesterol examination; and (6) diabetes examination. We chose these measures of preventive care because individuals with CP/SB are at a much higher risk for cardiometabolic conditions, low bone density, and fractures than the general population.7,9,10 Furthermore, these services are reliably captured in claims data. Use of these services was identified using Current Procedural Terminology or Healthcare Common Procedure Coding System codes (Supplemental Table 2).
Covariates
The covariates considered for risk adjustment included age; sex; year of enrollment; patient’s educational attainment; household income; diagnosis of any psychological, cardiovascular, and musculoskeletal illnesses; Elixhauser comorbidity score; and location based on the 9 US Census Divisions (New England, Middle Atlantic, South Atlantic, East North Central, East South Central, West North Central, West South Central, Mountain, and Pacific). Age was a continuous variable. Educational attainment was categorized as less than high school degree, high school degree and some college, or bachelor’s or graduate degree. Annual household income categorized as less than $40,000, $40,000 to $99,000, and more than $100,000. Psychological, cardiovascular, and musculoskeletal conditions were identified in the first 12 months of the patients’ enrollment on the insurance plan (Supplemental Table 3). To capture full comorbidity history, the first year of enrollment was used to identify comorbid conditions. All analyses were conducted at a patient level with race or ethnicity being proxies for racial/ethnic inequities in the use of preventive care.16 We compared our adjusted predicted outcomes between White and Black adults and White and Hispanic adults.
Statistical Analysis
All analyses were conducted using SAS version 9.4 (SAS Institute). Statistical testing was 2-tailed with a significance level of 0.05.
Bivariate analysis of baseline demographics and characteristics of White, Black, and Hispanic adults with CP/SB were examined. For categorical variables, percentages were compared between White and other racial/ethnic groups using the X2 test. For continuous variables, means and standard deviations were used for the analysis. Asian adults were excluded from analysis due to a small sample size, however, we described their unadjusted demographics, comorbid conditions, and use of preventive services in the Supplemental Table 4, Supplemental Table 5, and Supplemental Figure 2.
Measuring Racial/Ethnic Inequity
To measure racial/ethnic inequity, we quantified the definition provided by the National Academy of Medicine.27 Racial/ethnic inequity is defined as a difference in access or treatment provided to members of different racial or ethnic groups that is not justified by the underlying health conditions or treatment preferences of patients.27,28 We used a 3-step procedure to estimate inequity in use of preventive services. First, we matched White with Black adults and White with Hispanic adults, separately, based on their health-need variables—including age, sex, Elixhauser comorbidity score, and any psychological, cardiometabolic, and musculoskeletal conditions. Matching was performed using a caliper size of 0.0001 with a 1:1 matching ratio without replacement. Post-hoc comparisons on matched variables were performed to ensure covariate balance on the matching variables between White. and Hispanic adults (Supplemental Table 6) and White and Black adults (Supplemental Table 7). Second, for each outcome variable, we fitted 2 multivariate regression models to compare White adults with Black and Hispanic adults. Multivariable generalized linear models with repeated measures using a generalized estimating equations approach were performed. We used a binomial distribution and log link function with a compound symmetry covariance structure for any use of services. Additionally, interaction terms of race or ethnicity by income, education, and rolling year were included in each regression model. Adjusted predicted values and odds ratios were calculated. Finally, inequity was calculated as the adjusted predicted difference between White adults, and Black and Hispanic adults, separately.
RESULTS
Table 1 presents the unadjusted and unmatched characteristics of privately insured White, Black, and Hispanic adults with CP/SB. The average age was 45.5 years with a standard deviation of 17.6. With approximately 56% of the sample being female, there were no differences in sex among our subpopulations. Compared with White adults, Black adults had a higher comorbidity score and Hispanic adults had a lower comorbidity score.
Characteristics of White, Black, and Hispanic Adults With Cerebral Palsy/Spina Bifida
Black and Hispanic adults had lower educational attainment. Having less than a high school degree was more common among Hispanic (4.1%, P <.001) and Black adults (0.4%, P <.001) compared with White adults (0.2%). A greater proportion of White adults (16.5%) had a bachelor’s degree or higher, compared with Black (4.5%, P <.001) and Hispanic adults (10.0%, P <.001). Furthermore, there were income differences between the subgroups; household income of less than $40,000 was more common among Black (40.8%, P <.001) and Hispanic adults (28.5%, P <.001), compared with White adults (19.9%). About 30.3% of White adults compared with 16.3% of Black (P <.001) and 10.2% of Hispanic adults (P <.001) had an annual income of $100,00 or greater.
Table 2 compares the rates of different psychological, cardiometabolic, and musculoskeletal conditions between subgroups. There were no differences in rates of psychologic conditions between White and Black adults with CP/SB. Diabetes (16.5%, P <.001), hypertension (39.9%, P <.001), chronic kidney disease (4.7%, P <.001), heart failure (5.6%, P <.001), and hypercholesterolemia (12.3%, P = .019) were more prevalent among Black adults compared with White adults. Compared with Hispanic adults with CP/SB, White adults were more likely to be diagnosed with an adjustment disorder (2.7% vs 1.5%, P = .016), anxiety (10.4% vs 8.4%, P = .027), or mood disorder (13.3% vs 9.7%, P <.001). Hypertension was also less prevalent among Hispanic adults (22.3% vs 28.2%, P <.001) compared with White adults.
Prevalence of Psychological, Cardiometabolic, and Musculoskeletal Conditions Among White, Black, and Hispanic Adults With Cerebral Palsy/Spina Bifida
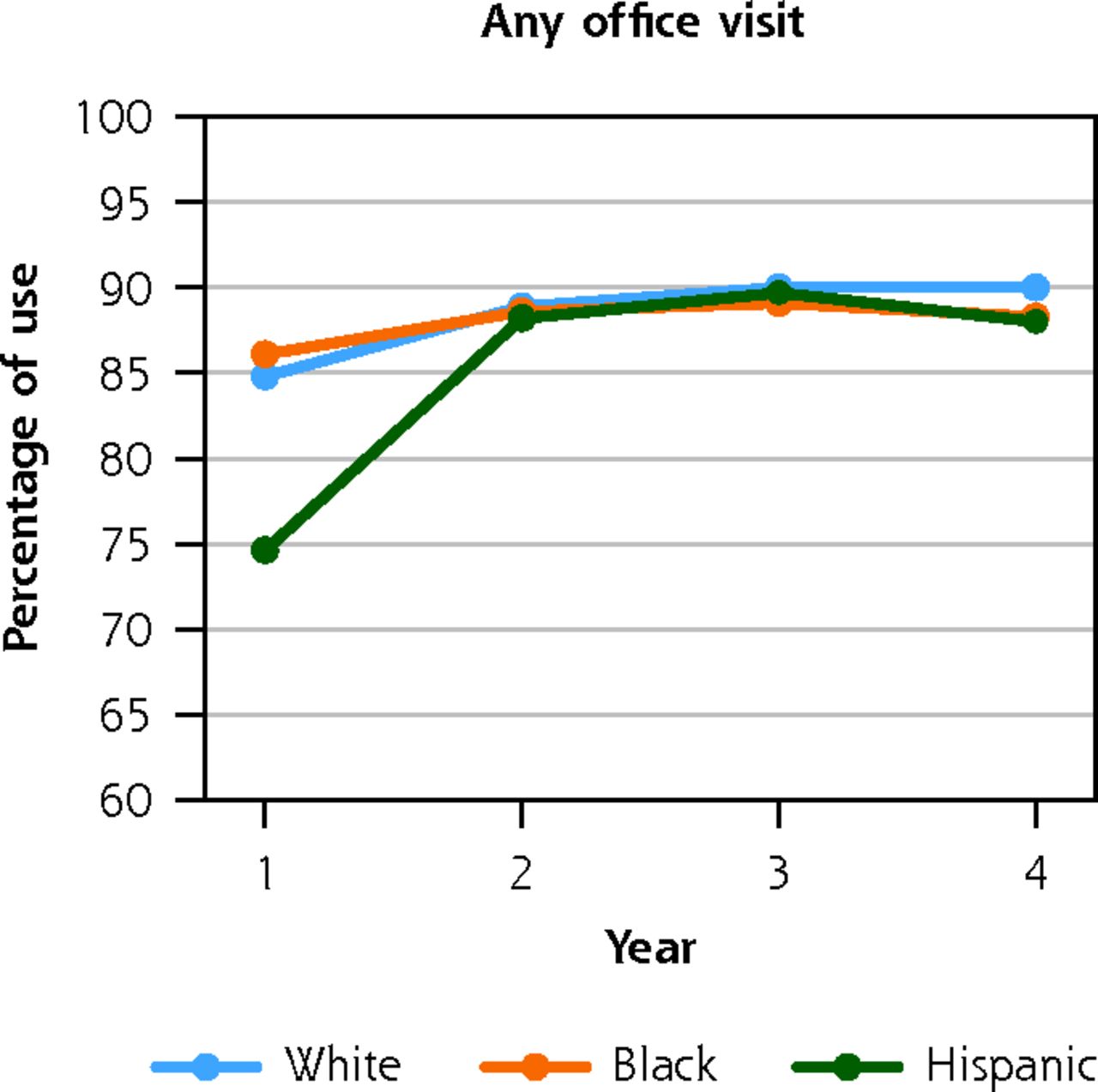
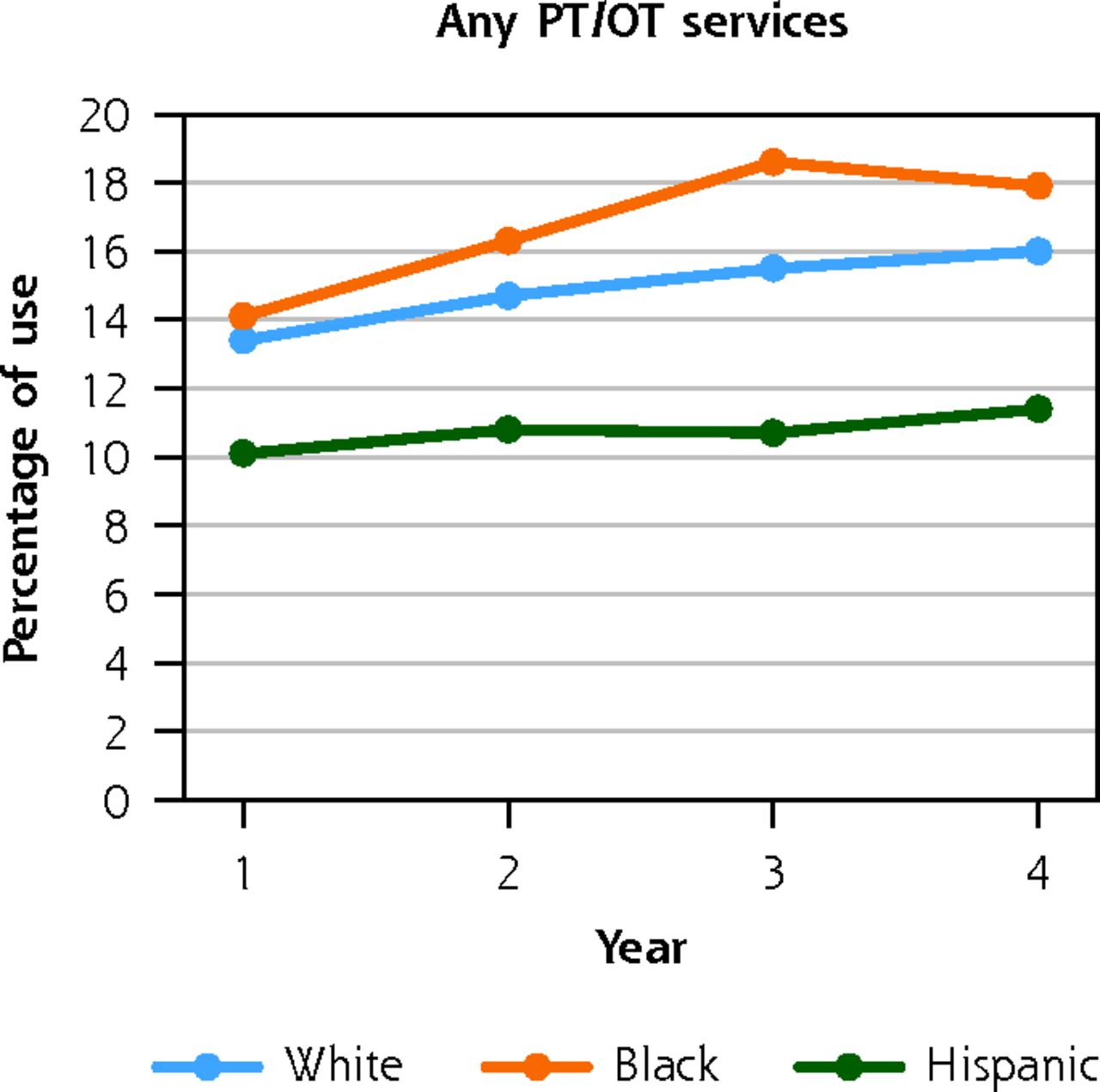
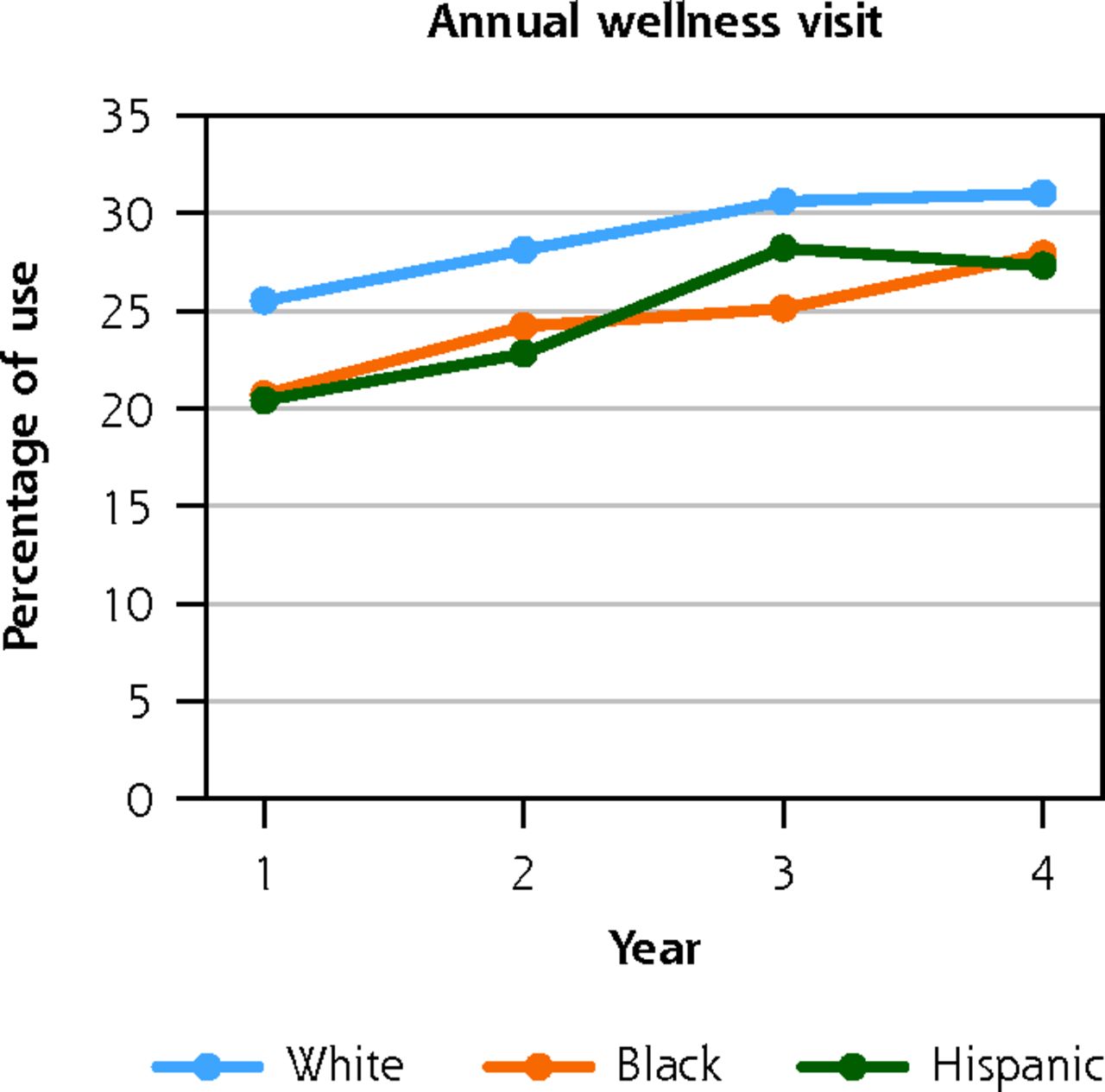
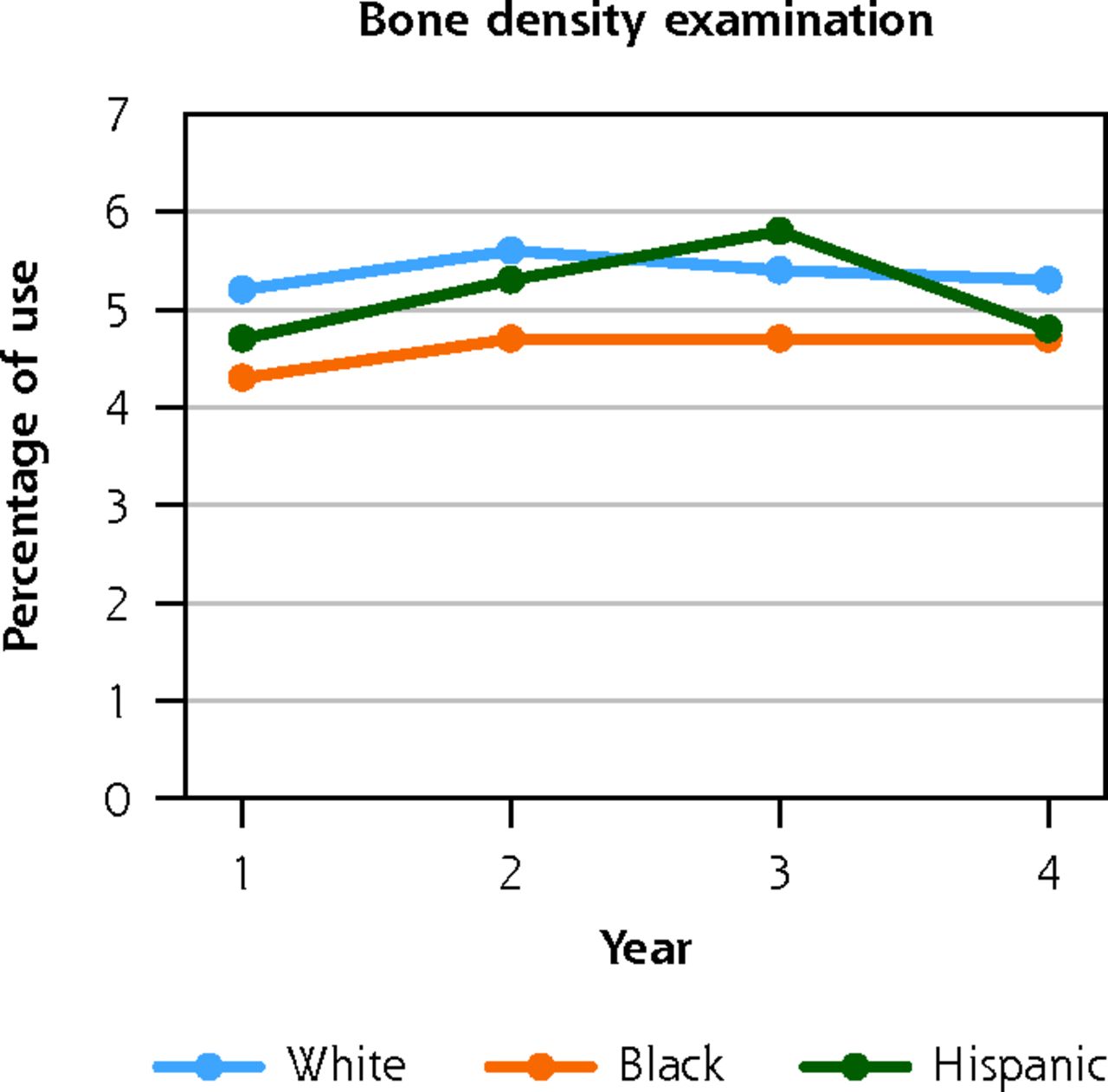
Figure 1 presents the unadjusted rates of preventive service use, by race/ethnicity during the follow-up period. There were large differences in wellness visits, with White adults having the highest rate compared with both Black and Hispanic adults. The percentage of wellness visits increased over time among all racial/ethnic groups. For example, in year 1, 25.5% of White adults, 20.7% of Black (P <.001) and 20.4% of Hispanic (P <.001) adults had an annual wellness visit; by year 4, the percentage of adults having a wellness visit changed to 31% of White, 27.9% of Black (P = .018), and 27.3% of Hispanic adults (P = .007). Diabetes screening was higher among Hispanic adults compared with White adults, but rates increased over time for both subgroups. In year 1, 19.5% of White and 21.1% of Hispanic adults received diabetes screening (P = 0.189); this increased to 23.8% of White and 32.6% of Hispanic adults in year 4 (P <.001). Bone density screening was low for all subpopulations.

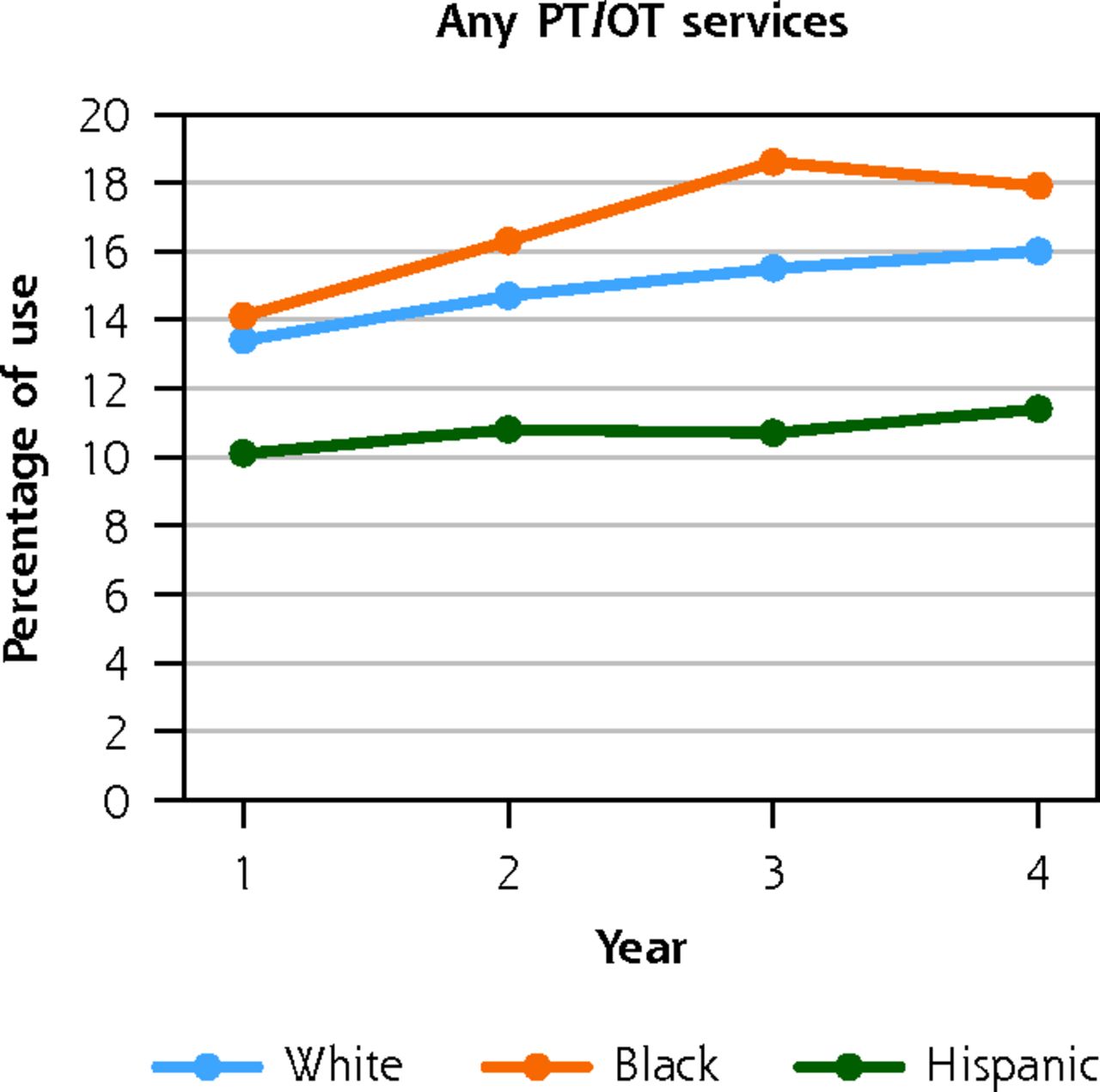
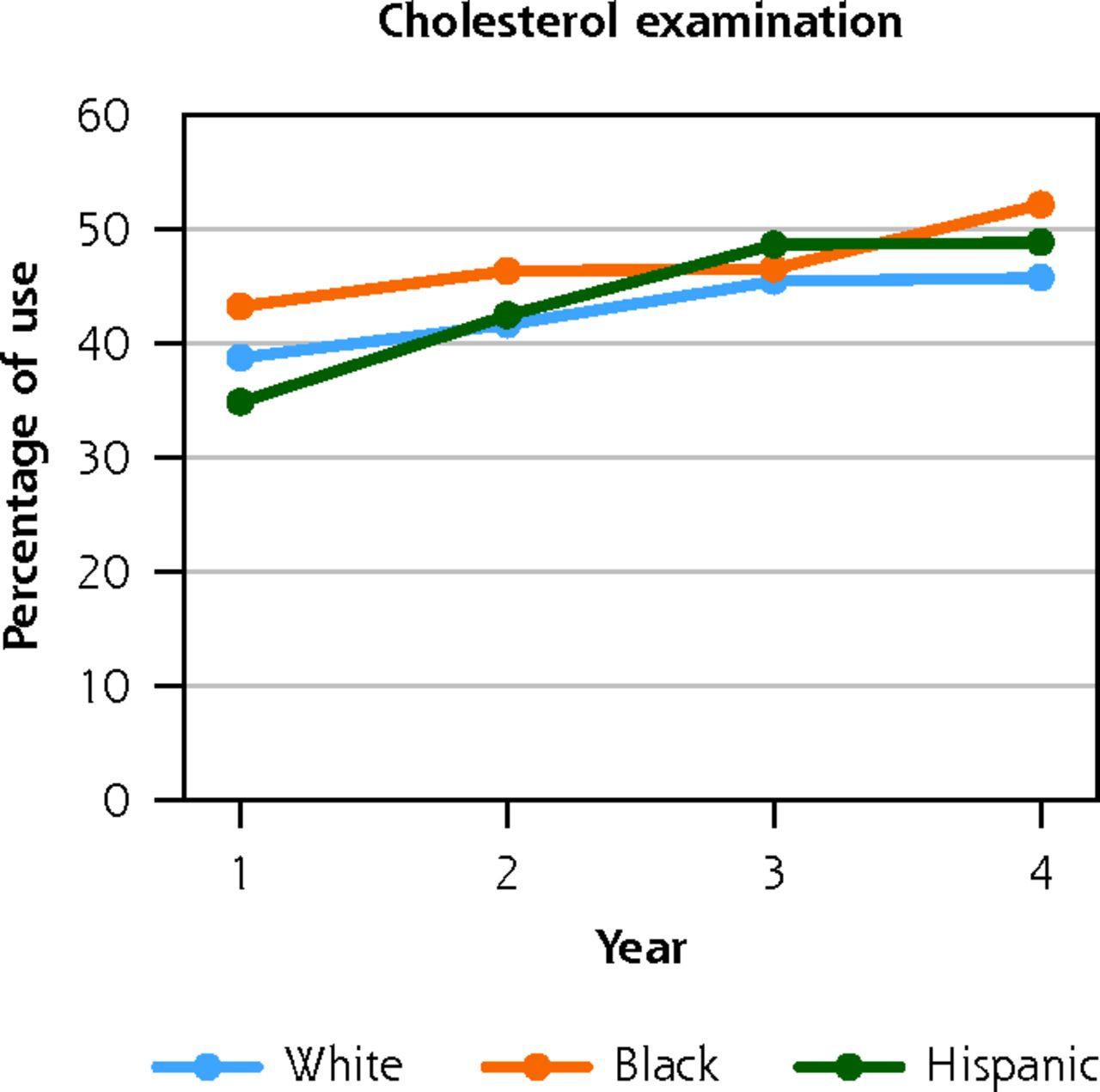


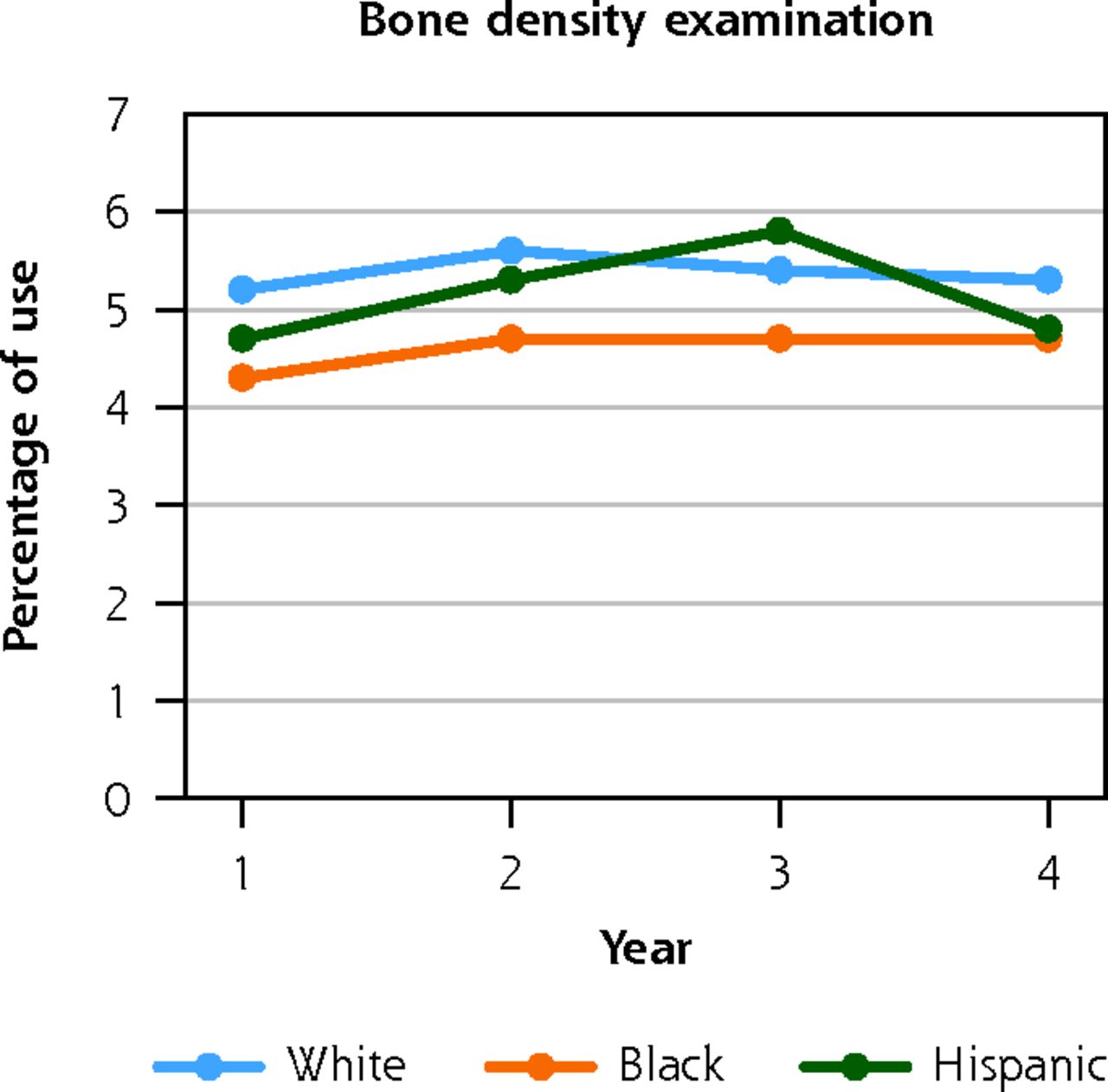
Unadjusted use of preventive services among privately insured White, Black, and Hispanic adults with cerebral palsy or spina bifida.
PT = physical therapy; OT = occupational therapy.
Note: data source is the 2007-2017 Clinformatics Data Mart (OptumInsight).
Table 3 reveals the adjusted predicted rate of preventive service use and corresponding odds ratios for Hispanic and Black adults compared with their matched White counterparts. About 30% of White compared with 23% of Hispanic adults had an annual wellness visit. Hispanic adults had lower odds of having a wellness visit (OR = 0.71, 95% CI, 0.53-0.96). However, 20% of Hispanic vs 14% of White adults had diabetes screening (OR = 1.47, 95% CI, 1.13-1.93).
Adjusted Predicted Racial/Ethnic Disparities in Use of Preventative Services Among White, Black, and Hispanic Adults With Cerebral Palsy/Spina Bifida
Approximately, 30% of White vs 18% of Black adults (OR = 0.50, 95% CI, 0.24-1.00) had an annual wellness visit. Additionally, 2% of White vs 1% of Black adults had any bone density screening (OR = 0.54, 95% CI, 0.31-0.95). Regression results are presented in Supplemental Tables 8-19.
DISCUSSION
In this study, we used commercial insurance claims data to evaluate racial/ethnic inequities in the use of preventive services among privately insured adults with CP/SB. Our findings revealed that both Black and Hispanic adults had substantially lower odds of having an annual wellness visit, compared with White adults. Furthermore, compared with White adults, Black adults had lower odds of having bone density screening. We did not find racial/ethnic inequities in use of other preventive services, specifically office visits, cholesterol assessment, physical/occupational therapy, and diabetes screening. Finally, although use of most preventive services slowly increased over time, the rate of use, in general, was low among privately isured adults with CP/SB.
In concordance with prior research,38 our findings revealed inequities in use of some preventive care—such as wellness visits and bone density screening. Wellness visits were introduced in 2011 as part of the Patient Protection and Affordable Care Act (ACA). Although there is no out-of-pocket cost associated with wellness visits, racial/ethnic inequities in utilization persist.33,38,39 Inequities in access to care have mainly been attributed to existing gaps in health insurance coverage and socioeconomic status.38–41 All individuals in our study had stable private insurance coverage and we matched White adults and minorities by their health needs (age, sex, and comorbidity conditions). Our findings, however, revealed wide gaps in both income and education among our privately insured cohorts of adults with CP/SB, with White adults having substantially higher educational attainment and annual income levels.
While we did not find any inequities in any office visit, cholesterol screening, physical/occupational therapy, and diabetes screening, Hispanic adults had higher odds of diabetes screening compared with White adults, which might be explained by a higher prevalence of cardiometabolic conditions among this subpopulation. Insurance coverage is one of the major facilitators of access to care,28,29 and having uninterrupted access to health insurance has been associated with reducing racial/ethnic inequities.30 For example, since Medicare coverage of colonoscopy in July 2001, disparity in colon cancer screening between White and Black adults has been reduced.42 Furthermore, a longitudinal study evaluating the timing of disability onset, comparing White and Black adults, found that supplemental private health insurance was protective against disability onset, even after controlling for socioeconomic differences.43 Having private insurance has been associated with fewer functional limitations over time and lower odds of limitation onset.44 Access to health insurance enables a more equitable use of health care services.31,32
Our results indicated that use of preventive services increased over time across all subgroups. As age increases, there is a corresponding increased burden of chronic illnesses and need for preventive services. Furthermore, since the enactment of the ACA in 2010, due to direct and indirect effects of cost sharing, there has been an upward trend of preventive care use among the general population.39 The ACA was associated with reducing inequities in access to care and in preventive care.45 Moreover, research shows an association between the ACA and increase in use of preventive services by privately insured Hispanic and Black patients.46
Nevertheless, the overall utilization of preventive health care services among adults with CP/SB remains low. This finding is supported by prior studies showing lower rates of preventive service utilization among individuals with disabilities compared with the general population.47–50 For example, research has shown that women with physical disabilities are less likely to receive a pap smear or mammogram.51,52 Additionally, the rates of bone density screening are particularly concerning, given the fact that individuals with CP/SB are at a higher risk for osteoporosis and fractures than the general population.6–8
When inequities are identified, action must be taken to make care more equitable. One major barrier to improved access to care is the physical structure and set up of primary care offices. For instance, a study of primary care offices in California revealed that an accessible weight scale was available in just 3.6% of offices, and bathrooms and exam spaces posed access barriers. Reducing physical barriers to care is particularly important.53 Use of telehealth may make care more accessible, especially when physical barriers persist.54,55 Furthermore, it is imperative to educate clinicians on appropriate care for adults with a pediatric-onset disability. A survey of family/internal medicine residents found that few clinicians had received disability-specific training during medical school or residency.56 Similarly, health systems must recognize that minority individuals with physical disabilities are less likely to utilize preventive care. Initiatives to address physical and logistical barriers to care must prioritize minority populations. While this study included privately insured adults with disability, these interventions would likely benefit all adults with disabilities.
Several limitations are noteworthy. This study was not representative of the overall population of adults with CP/SB. It included only privately insured adults, with better access to economic resources and stable health coverage over time. Due to physical limitations, lack of accommodations, and lack of accessible transportation, individuals with CP/SB are disproportionately unemployed or underemployed and many utilize public insurance.57,58 Due to this limitation, there is an inherent selection bias in our population. Most patients with disability have public insurance coverage, and we anticipate much larger inequities in the use of preventive services between those covered by public vs private insurance. Furthermore, our data did not have an ethnoracial representation of the US population. Future research should focus on using representative data. Additionally, using claims data, we were unable to capture the personal or cultural preferences of our subpopulation cohorts, their lifestyle choices, and environmental barriers. Finally, it is possible that patients with disabilities had other insurances. Thus, some of the services were not recorded in the Optum claims data.
CONCLUSION
Although insurance and social status have strong impacts on health care inequities between White patients and minorities, this study accounted for those factors and focused on detection of inequities for Black and Hispanic adults with pediatric-onset disabilities. Black and Hispanic adults had substantially lower odds of having a wellness visit compared with White adults. Furthermore, Black adults had lower odds of having bone density screening. Preventive service utilization increased for all subpopulations over the 4-year follow-up period. Despite this increase, overall rates of service utilization remained low. Improved physical accessibility of health care settings, greater adoption of telehealth, and increased clinician education regarding the health care needs of individuals with disabilities could lessen these inequities in the future. It is imperative that health care systems target interventions to clinical settings that serve minority patients, where they could have the greatest impact.
Footnotes
Conflicts of interest: authors report none.
Funding support: The National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR #90RTHF0001-01-00).
- Received for publication July 22, 2021.
- Revision received April 27, 2022.
- Accepted for publication May 4, 2022.
- © 2022 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}