
Abstract
PURPOSE During a pandemic, when there are many barriers to providing preventive care, chronic disease management, and early response to acute common diseases for primary care providers, it is unclear whether primary care attributes contribute to reducing hospitalization. We aimed to examine the association between core primary care attributes and total hospitalizations during the COVID-19 pandemic.
METHODS We conducted a nationwide prospective cohort study during the pandemic using a representative sample of the Japanese adult population aged 40 to 75 years. Primary care attributes (first contact, longitudinality, coordination, comprehensiveness, and community orientation) were assessed using the Japanese version of Primary Care Assessment Tool (JPCAT). The primary outcome measure was any incidence of hospitalization during a 12-month period from May 2021 through April 2022.
RESULTS Data from 1,161 participants were analyzed (92% follow-up rate). After adjustment for possible confounders, overall primary care attributes (assessed by the JPCAT total score) were associated in a dose-dependent manner with a decrease in hospitalizations (odds ratio [OR] = 0.37, 95% CI, 0.16-0.83 for the highest score quartile, compared with no usual source of care). All associations between each domain score of the JPCAT and hospitalization were statistically significant when comparing the highest quartile with no usual source of care.
CONCLUSIONS Our study revealed that the provision of primary care, particularly high-quality primary care, was associated with decreased total hospitalization, even during a pandemic when there are many barriers to providing usual medical care. These findings support policies that seek to strengthen primary care systems during and after the COVID-19 pandemic.
INTRODUCTION
Prevention of hospitalization, which is associated with mortality, complications, and increased health care costs, is an important role of primary care. Studies before the coronavirus disease 2019 (COVID-19) pandemic have examined associations between essential attributes of high-quality primary care and fewer hospitalizations. For example, systematic reviews reported that greater continuity with a primary care physician can reduce total hospitalizations.1,2 Other studies demonstrated that, greater access to and more comprehensive primary care are associated with fewer hospitalizations.3,4
The COVID-19 pandemic dealt serious blows to the primary care system globally. During the pandemic, in addition to usual medical care, primary care providers allocated resources to aid in the triage of patients and treatment and vaccination for COVID-19. Moreover, studies conducted in the United States and Japan have consistently reported that the number of outpatient visits decreased while telemedicine visits increased during the pandemic.5-7 As a result, a decline in utilization of preventive services, reduction in diagnoses of chronic diseases, and worsening control of chronic diseases have been reported.8-10
In Japan, as in other countries, primary care clinicians performed the initial assessment of and vaccination against COVID-19 alongside usual medical care during the pandemic.11 Primary care services in Japan are provided in both community clinics and outpatient departments of small- and medium-sized hospitals. Care is provided by teams consisting of physicians trained in an internal medicine-based residency program, nurses, medical assistants, and other health care professionals.12 The Japan Primary Care Association has certified family physicians since 201013 and the Japanese Medical Specialty Board started a new certification program for primary care specialists in 2018.14 Formal training of physicians specializing in primary care has just begun in Japan; thus, variations in the quality of primary care is expected.
Our team consists of faculty and alumni from the Division of Clinical Epidemiology of The Jikei University School of Medicine which has conducted primary care research about quality assessment, multimorbidity, home medical care, patient complexity, etc.
During a pandemic, when there are many barriers to providing preventive care, chronic disease management, and early response to common acute diseases, it is unclear whether primary care attributes contributed to reducing hospitalization for COVID-19 and other causes. Therefore, in this study, we aimed to examine the association between core primary care attributes and total hospitalizations during the COVID-19 pandemic using a representative sample of the Japanese adult population.
METHODS
Design, Setting, and Participants
We conducted a nationwide prospective cohort study in Japan, titled the National Usual Source of Care Survey, from May 2021 through April 2022 (follow-up period of 12 months), during the fourth to sixth waves of COVID-19. The sixth wave, that began in January 2022 with the Omicron vaient, was the largest ever in Japan, with more than 90,000 new cases of COVID-19 occurring daily.15 In this study, a nationally representative panel, administered by the Nippon Research Center, was used to select potential participants. This panel comprised approximately 70,000 residents who were selected from the Japanese adult population using a multistage sampling method.16 From the panel, prospective participants aged 40 to 75 years were selected through stratified random sampling by age, sex, and residential area. In the baseline survey, we evaluated the usual source of care and the primary care attributes, health conditions, health-related quality of life, and sociodemographic characteristics of the study participants. A follow-up survey was conducted 12 months after the completion of the baseline survey to assess health care utilization, including hospitalization. Data collection for the initial and follow-up surveys was mail based. The respondents received a 500 yen gift certificate for each survey. The institutional review board of the Jikei University School of Medicine approved this study (approval number 32-416[10505]).
Measures
Primary Care Attributes
In the baseline survey, we used the Japanese version of Primary Care Assessment Tool (JPCAT) to assess primary care attributes through patient experience.17,18 The JPCAT is based on the Primary Care Assessment Tool, a well-established and internationally recognized scale for measuring primary care attributes.19,20 Previous studies have shown the JPCAT has good reliability and validity.17,18 It comprises 6 multi-item domains addressing the following primary care attributes: first contact, longitudinality, coordination, comprehensiveness (services available), comprehensiveness (services provided), and community orientation. In this study, we used the 13-item short version of the scale.18
First, the following item of the Primary Care Assessment Tool was used to identify an individual’s usual source of care: “Is there a doctor that you usually go to if you are sick or need advice about your health?” A participant was considered to have a usual source of care if he or she was able to identify a physician who practiced outside university hospitals. Second, for participants who had a usual source of care, we assessed the primary care attributes with the JPCAT. The JPCAT’s scoring system uses a 5-point Likert scale (1 = strongly disagree, 2 = somewhat disagree, 3 = not sure, 4 = somewhat agree, and 5 = strongly agree). Each response is converted into an item score from 0 to 4. The calculated means of the item scores in the same domain are multiplied by 25 to yield domain scores ranging from 0 to 100 points. The JPCAT total score is the mean of the 6 domain scores and reflects an overall measure of primary care attributes, with higher scores indicating better quality.
Hospitalization
The primary outcome measure in this study was the incidence of hospitalization during 12 months of the COVID-19 pandemic study period. Hospitalization was determined by the response to the follow-up survey item, “In the past 12 months, have you been hospitalized?” The participants were asked to answer on a binary scale (yes vs no). If participants answered yes to the primary question, they were asked to answer the following item on hospitalization: “In the past 12 months, have you been hospitalized because of infection with the novel coronavirus?” Participants were asked to respond yes or no.
Statistical Analysis
Descriptive statistics for continuous data were reported as means and standard deviations. Categorical data were reported as frequencies and percentages.
To examine whether the JPCAT total score was associated with hospitalization, we used multivariable logistic regression analysis. In addition, we performed ancillary analyses of the outcomes in relation to each JPCAT domain score. We categorized the JPCAT total score and domain scores into quartiles. The following potential confounders were selected based on the previous studies4,21,22 which investigated the association between primary care attributes and hospitalization: age (continuous), sex, educational level (less than a bachelor’s degree vs bachelor’s degree or more), number of chronic conditions (continuous), and health-related quality of life (continuous) assessed by the 5-level version of the Euro-Qol 5-dimensional questionnaire (EQ-5D-5L).23
We used a validated list of 20 chronic conditions that was created based on previous multimorbidity literature24 and relevance to the primary care population: hypertension, depression/anxiety, chronic musculoskeletal conditions causing pain or limitation, arthritis/rheumatoid arthritis, osteoporosis, chronic respiratory disease (asthma, chronic obstructive pulmonary disease, or chronic bronchitis), cardiovascular disease, heart failure, stroke/transient ischemic attack, stomach problem, colon problem, chronic hepatitis, diabetes, thyroid disorder, any cancer in the previous 5 years, kidney disease/failure, chronic urinary problem, dementia/Alzheimer’s disease, hyperlipidemia, and obesity. All confounders were evaluated at baseline using a self-administered questionnaire.
According to the sample size formula used in a previous study, events per variable values of 10 or more were necessary for logistic regression analysis.25 The incidence of hospitalizations in the Japanese adult population was assessed to be 1% per month according to a previous study.7 Thus, we estimated a minimum sample size of 750 because the maximum number of variables in this study was 9. However, a larger sample size was selected to accommodate the needs of other studies incorporated into the National Usual Source of Care Survey.
For each analysis, we used a 2-sided significance level of P <.05, without adjustment for multiple comparisons.26 Missing data on independent variables were handled by applying multiple imputations with 20 imputations using a fully conditional specification. Statistical analyses were conducted using R, version 4.2.1 (the R Foundation).
RESULTS
Participant Characteristics
From the national representative panel, 1,382 participants aged 40 to 75 years were selected through stratified random sampling, and 1,262 completed the baseline assessment. Among them, 1,161 (92%) participants completed the follow-up (Figure 1). Table 1 shows the baseline characteristics of the study population. We noted a trend suggesting that participants who were lost to follow-up were younger and had a usual source of care less frequently than those who completed the follow-up assessment. Among the participants who completed the follow-up, 87 (7.5%) were hospitalized during the 12 months. Among the participants who were hospitalized, 5 (5.7%) reported hospitalization due to COVID-19. Compared with participants without hospitalization, those with hospitalization were older, more often male, had more chronic conditions, had lower EQ-5D-5L scores, and had a usual source of care less frequently. Among participants who had a usual source of care, the mean JPCAT total score and all domain scores were lower in participants with hospitalization, compared with those not hospitalized.

Participant flowchart.
Participant Characteristics at Baseline
Primary Care Attributes and Hospitalization
Figure 2 shows the results of the multivariable logistic regression analysis used to investigate the association between the overall measure of primary care attributes (assessed by the JPCAT total score) and hospitalization. After adjusting for possible confounders, the JPCAT total score showed a dose-dependent association with a decrease in hospitalizations (adjusted odds ratio [aOR] = 0.37; 95% CI, 0.16-0.83) for the JPCAT highest quartile, compared with no usual source of care.
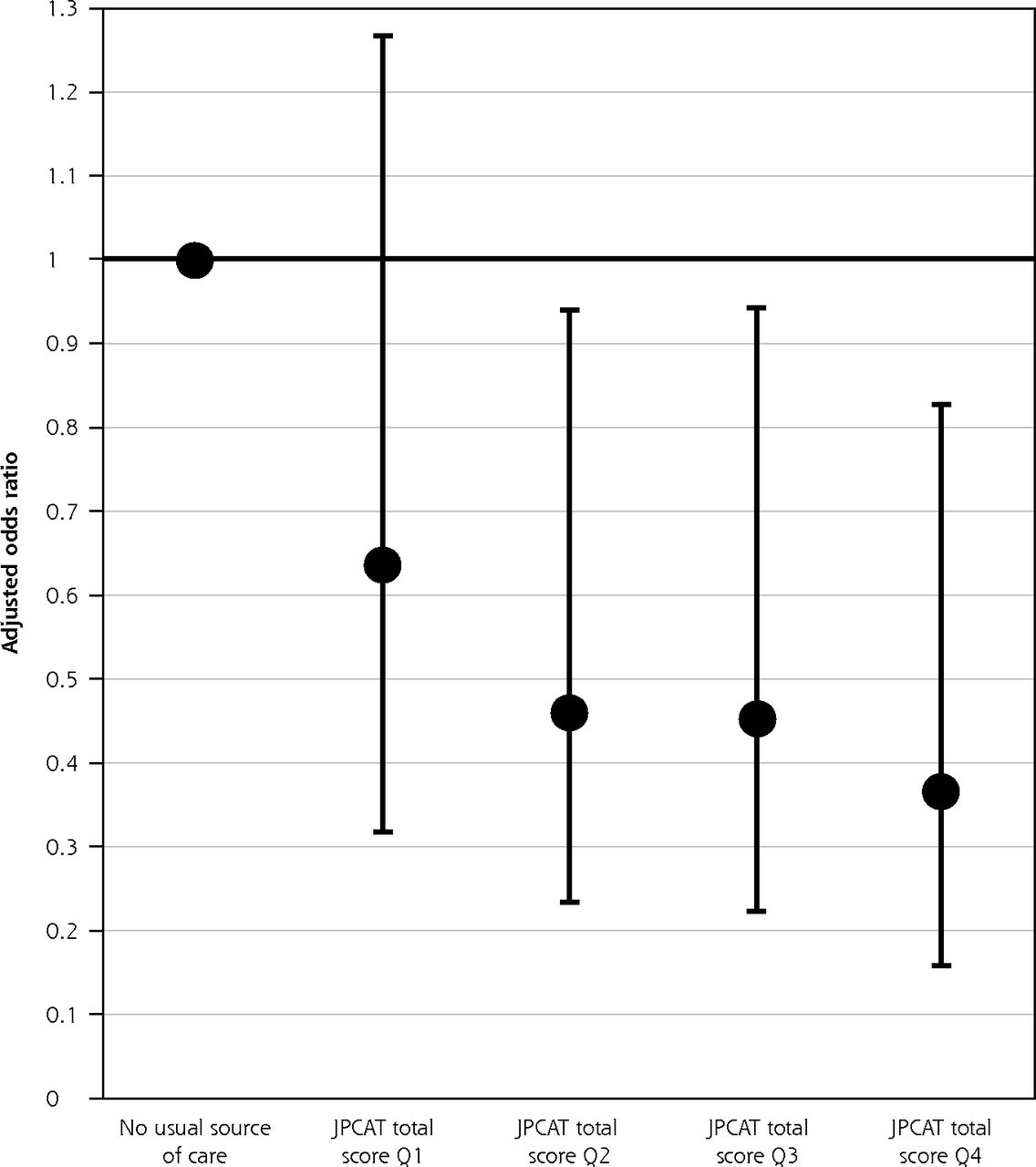
Association between the overall measure of primary care attributes and hospitalization.
EQ-5D-5L = 5-level version of the EuroQol 5-dimensional questionnaire; JPCAT = Japanese version of Primary Care Assessment Tool; Q = quartile.
Notes: Association assessed by the JPCAT total score. Adjusted for age, sex, educational level, number of chronic conditions, and EQ-5D-5L. Error bars indicate 95% CIs. JPCAT total score quartiles: Q1, 0.0-35.4; Q2, 35.4-47.9; Q3, 47.9-60.4; Q4, 60.4-100.0.
Table 2 shows the results of the multivariable logistic regression analyses modeling the associations of the JPCAT domain scores with hospitalization. Although the dose-response relationships were not clear, all associations between each domain score of the JPCAT and hospitalization were statistically significant when comparing the highest quartile with no usual source of care.
Hospitalization by JPCAT Domain Scoresa (N = 1,161)
DISCUSSION
Our nationwide prospective cohort study of the Japanese adult population found that the overall primary care attributes assessed by the JPCAT were associated with decreased hospitalization during the COVID-19 pandemic. The presence of a dose-response relationship indicated that the associations were causal. Moreover, all domains of the JPCAT, which represent first contact, longitudinality, coordination, comprehensiveness, and community orientation, were associated with fewer hospitalizations. These findings indicate that the provision of high-quality primary care contributed to decreased total hospitalization, even during a pandemic when there are many barriers to providing usual medical care. Preventing hospitalizations during a pandemic not only avoids deterioration in the health status of the population and reduces health care costs but also reduces inpatient hospital care overload.
The results of this study are consistent with findings before the COVID-19 pandemic, showing that each primary care attribute, such as accessibility, continuity, coordination, and comprehensiveness, is associated with a reduction in hospitalizations.1-4,27 Specifically, there is strong evidence that continuity of care can reduce hospitalizations. For example, a recent registry-based observational study in Norway reported that continuity of care by a general practitioner was associated with reduced acute hospital admission in a dose-dependent manner.21 Furthermore, this study showed an association between community orientation of primary care and hospitalization, which was previously unclear. Community orientation can improve the recognition, prevention, and management of diseases through the knowledge of all community members, not simply those who visit primary care practices.28 Especially during a pandemic, the integration of public health practice with the delivery of primary care services may be a more important process. As one of the mechanisms underlying our findings, a recent nationwide study reported that overall primary care attributes were associated with increased receipt of preventive care, such as screening, immunization, and counseling, during the COVID-19 pandemic.29 Further research is needed to investigate other mechanisms related to the management of chronic diseases, mental health, and social health disparities.
Our findings support policies that seek to strengthen the primary care systems in each country during and after the COVID-19 pandemic. For instance, a new consensus report by the National Academies of Sciences, Engineering, and Medicine emphasized that the United States should prioritize the implementation of high-quality primary care by the government and private sector.30 In Japan, the Ministry of Health, Labour and Welfare has recommended that all individuals should have a usual source of care, called a kakaritsukei in Japanese, and identified strengthening primary care functions as an important policy issue.31 Based on lessons learned during the pandemic, policy makers and health care system leaders in Japan and other countries should ensure that high-quality primary care is available to every individual.
To the best of our knowledge, this is the first study to report the impact of primary care attributes on hospitalization during a pandemic. A key strength of our study is the use of longitudinal data from a nationwide study with a sample representative of the Japanese adult population, which allows for generalization of our results to the wider population. Another strength of this study was the high follow-up rate. Furthermore, the assessment tool used, the JPCAT, is a validated and internationally established tool for evaluating primary care attributes.
However, our study had several potential limitations. First, we did not have outcome data on participants who had relocated, lost their ability to respond to the survey, or died during the follow-up period. The participants who were lost to follow-up were younger than those who completed it and may have experienced fewer hospitalizations. They also reported lower JPCAT scores in the baseline survey; thus, this may have led to an overestimation of the relationship between primary care attributes and hospitalization. Second, while we used a structured questionnaire for the data collection, self-reported data for identifying hospitalization and chronic conditions may have introduced a misclassification bias. Third, the sample of participants did not include patients with diseases such as advanced dementia. Finally, we investigated hospitalization over a short period of 12 months, but the association between primary care attributes and hospitalization over a longer period remains unknown.
In conclusion, this study revealed that the provision of primary care, particularly high-quality primary care, was associated with decreased total hospitalization, even during a pandemic when there are many barriers to providing usual medical care. These findings support policies seeking to strengthen primary care systems during and after a pandemic.
Footnotes
Conflicts of interest: Aoki and Matsushima received lecture fees and lecture travel fees from the Centre for Family Medicine Development of Japanese Health and Welfare Co-operative Federation. They are advisers of the Centre for Family Medicine Development practice-based research network. Matsushima’s son-in-law worked at IQVIA Services Japan K.K. which is a contract research organization and a contract sales organization. Matsushima’s son-in-law works at Syneos Health Clinical K.K. which is a contract research organization and a contract sales organization.
Funding support: This work was supported by JSPS KAKENHI Grant Number JP20K18849 and Pfizer Health Research Foundation Grant Number 21-E-01.
- Received for publication July 26, 2022.
- Revision received September 25, 2022.
- Accepted for publication September 30, 2022.
- © 2023 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Association between person-centred care quality and advance care planning participation in haemodialysis
- Association Between Person-Centered Care Quality and Advance Care Planning Participation in Patients Undergoing Hemodialysis: A Multicenter Cross-Sectional Study
- COVID-19 and Primary Care: Taking Stock