
Abstract
PURPOSE Few studies have determined whether clinician usage of a community health information exchange (HIE) directly improves patient care transitions. We hypothesized that lookup in the HIE by primary care physicians of patients recently released from the hospital would increase the time until hospital reuse.
METHODS We identified a retrospective cohort of 8,216 hospital inpatients aged over 18 years that were discharged from January 1, 2021 through November 30, 2021 using the Paso del Norte Health Information Exchange, in El Paso County, Texas. All patients had a primary care physician visit within 30 days after hospital discharge, and we identified patients that were looked up in the HIE close to that visit. Of the cohort, 2,627 were rehospitalized and 3,809 visited an emergency department (ED) during the follow-up window. The remaining 1,780 patients were controls. We conducted survival analysis, censoring at the second ED or inpatient visit or end of the study window (January 31, 2022). The model was adjusted by ethnicity, gender, insurance, and age.
RESULTS Lookup in the HIE was significantly associated with reducing the likelihood of visiting the ED by 53% and being rehospitalized by 61%. Lookup in the HIE was associated with an increased median time to use of the ED after inpatient discharge from 99 to 238 patient days. Ethnicity, insurance, gender, and age were also significant predictors of hospital reuse.
CONCLUSIONS Increased utilization of community HIEs by primary care physicians on behalf of their recently discharged patients may dramatically increase the time until inpatient or ED reuse.
INTRODUCTION
The health care system in the United States is markedly fragmented, with patients moving through levels and types of care that benefit when seamless transfers of information from one clinic to the next is possible.1 Despite the promise of electronic health records (EHRs) to enhance coordination and efficiency of care, proprietary EHR systems and a host of other issues make record sharing difficult. Stepping into the gap are a growing number of secure health information exchanges (HIEs), which seek to merge EHRs from different systems into a single organized electronic database that can be looked up by clinicians at the point of care.2 According to data from the American Hospital Association, HIE use among hospitals in the United States has gradually increased from about 30% in 2012 to 55% in 2015 and 65% in 2019.3-5
Health information exchanges include a convener entity and its participating health provider organizations.5,6 Most HIEs are based within clinical care or insurance provider systems (enterprise HIEs), integrated into vendor-mediated EHRs, or bring together systems within geographic regions (community HIEs).7,8 Among these varying structures, some of the most promising benefits to health outcomes are reported from community HIEs.9 Community HIEs, however, also face larger barriers to development and adoption because they must integrate data from the largest variety of systems.10
In this study, we focused on one of the most common and fraught types of care transitioning that can be mediated by a community HIE, from inpatient hospitalization to primary care physicians.11 Primary care physicians need to be aware of medications, procedures, and hospital instructions for a patient. Inpatient hospitalization is indicative of more severe symptoms and complex treatment needs. Frequent readmission of patients shortly after discharge is commonplace,12-14 as is utilization of emergency departments (EDs).15 While a primary care physician review of hospital records is only 1 time point in what may be a complex transition, it may be pivotal. We hypothesized that when primary care physicians use a community-level HIE for treating their recently discharged patients, it increases the time until hospital reutilization.
METHODS
Data Source
The non-profit Paso del Norte Health Information Exchange (PHIX) became operational in 2016. The PHIX is located at a secure facility which receives discrete data from EHRs from the 11 hospitals and 28 participating primary care clinics across 6 different organizations in El Paso County, Texas. Within the 11 hospitals, there are multiple EHR platforms currently in use, including markedly different implementations of the same platform. The records are received by PHIX electronically in real time and immediately merged into a confidential community medical record for individual patients which can only be viewed by a credentialed clinician responsible for treating that patient. Since 2016, only 695 patients (approximately 0.05%) have decided to not have their data sent to PHIX.
Inclusion and Exclusion Criteria
We identified a retrospective cohort of patients in the PHIX who were released from hospital inpatient care from January 1, 2021 through November 30, 2021. Patients were included in the data set if they had a recorded index visit with their primary care clinician within 30 days after hospital release and did not have another hospital inpatient or ED visit before that index visit (Supplemental Figure 1). If a patient had a second hospital inpatient or ED visit after their index visit and before January 31, 2022 (end of the study window), the dates of those visits were recorded, along with the top 3 International Statistical Classification of Diseases, 10th Revision (ICD-10) billing codes used to identify the hospital diagnoses. All patients had to be aged over 18 years at the time of their first hospital discharge. The study was deemed exempt (under category 4) by the Institutional Review Board at Brigham Young University.
Data Set Preparation
The primary exposure variable of interest was whether a primary care physician looked up a patient’s record in the HIE during the index visit. If a patient lookup occurred within 2 days prior or 2 days after the index primary care physician visit, they were designated as having been looked up by the physician. Most lookups occurred on the same day (Supplemental Figure 2). We allowed for the lookup to occur after the visit because primary care physicians may look up a patient after being informed of the hospital discharge during the visit.
The primary outcome of interest was whether a patient was readmitted to the hospital or visited the ED after visiting their primary care physician. Patients who met inclusion criteria were divided into 3 outcome groups: (1) patients whose 1st hospital visit after the index visit was to an ED and they were not admitted as an inpatient (case group 1); (2) patients whose 1st hospital visit after the index visit was an ED visit that led to admission as a hospital inpatient (case group 2); and (3) patients with no subsequent ED or hospital inpatient visits after their index visit (control group). Note that it is standard practice for non–maternal care inpatients to be admitted through the ED.
We did not attempt to further identify whether patients’ first and second encounters with the hospital system were for the same or associated reasons, because it is difficult to make that designation using ICD-10 codes at discharge. For example, if the patient’s initial hospitalization had a code for sepsis, and then they present at the ED with abdominal pain, it is very difficult to know if the abdominal pain was related to the sepsis inpatient visit. However, we did use the ICD-10 codes to eliminate patients who were recorded as inpatient because they were at the hospital for standard care related to normal pregnancy. Patients who present at the hospital, for example, for false labor, are marked inpatient in El Paso hospital systems.
Patients could only be in the data set once. We aggregated individual insurance providers into larger categories as shown in Supplemental Table 1. Ethnicity variables were also collapsed to either Hispanic/Latine or non-Hispanic/Latine and age variables were collapsed to being aged less than 50 or 50 years and older.
Statistical Analysis
We calculated the frequency and percentage of patients in demographic groups stratified by whether they were looked up in the HIE by the primary care physician. We also stratified the demographic variables and whether patients were looked up in the HIE by their primary care physician by case-control status and conducted appropriate tests to determine statistical significance (χ2, t-tests, and Kruskal-Wallis).
We used survival analysis to determine the time between hospital visits for persons of different age groups, genders, ethnicities, insurance types, and HIE lookup status with the survival package found in R version 4.1.1 (the R Foundation). A Cox proportional hazards model was generated to determine the statistical significance of each exposure variable to the outcome of interest. Finally, we determined the proportion of visits by group (divided by first and, when applicable, second visit, for cases) by ICD-10 code groups to help determine whether types of hospitalizations were more likely to occur among patients who were looked up in the HIE.
RESULTS
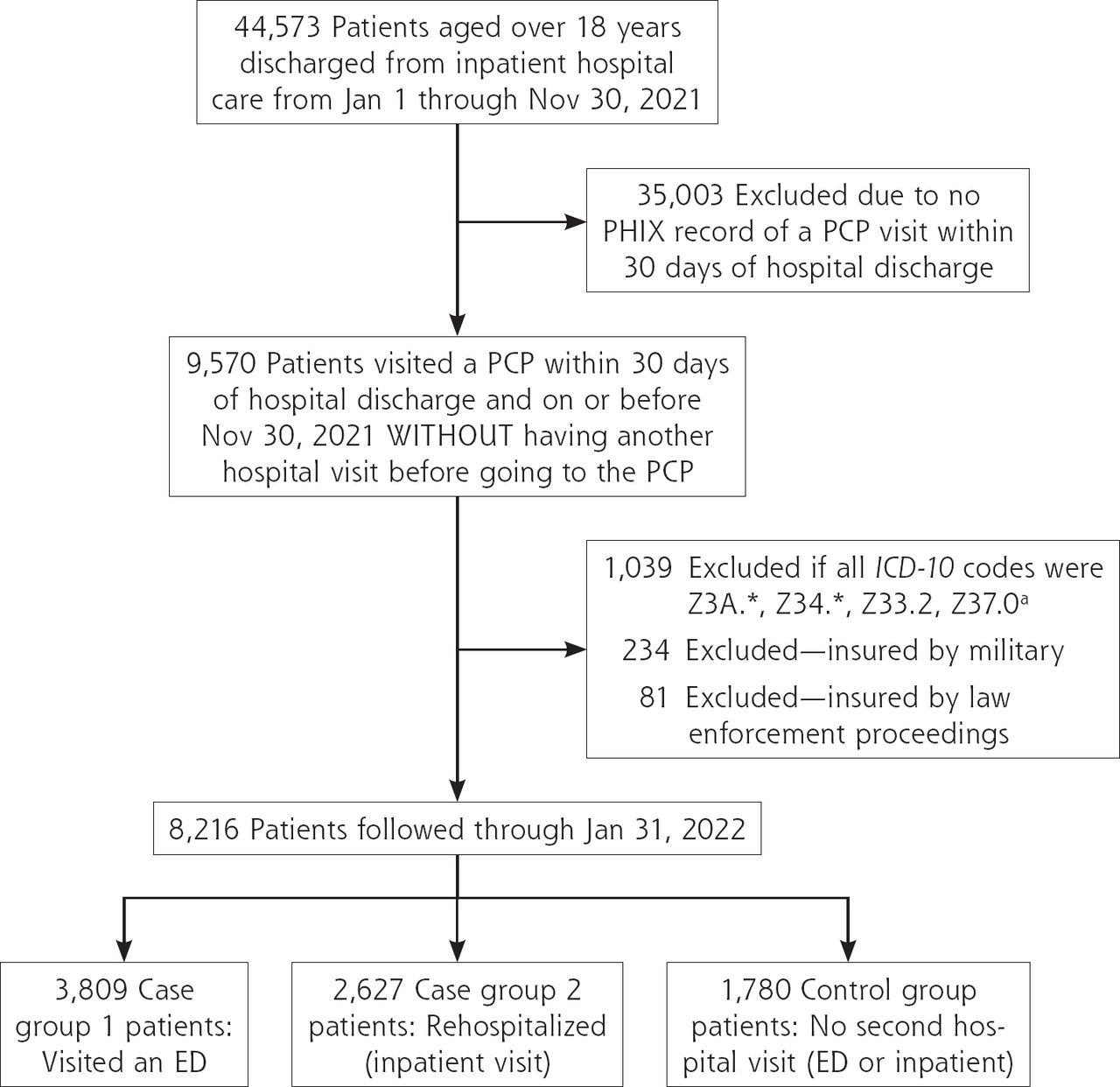
There were 44,573 patients identified in the PHIX system who were aged over 18 years and were discharged from inpatient hospital care from January 1, 2021 through November 30, 2021. The effect of each type of exclusion criteria on final cohort size are shown in (Figure 1). The resulting 8,216 patients were divided into 2 comparison groups and 1 control group for analysis (described in the methods). Primary care physicians looked up 270 (3.29%) of patients in the HIE within 2 days before or after the index visit. Table 1 provides comparisons of demographics between those with an HIE lookup and those without.

Flowchart of cohort and group selection.
ED = emergency department; ICD-10 = International Statistical Classification of Diseases, 10th Revision; PCP = primary care physician; PHIX = Paso del Norte Health Information Exchange.
a These codes were excluded because they indicate normal pregnancy or elective termination of pregnancy. For example, patients with false labor were labeled as inpatient in the system. They were expected to return as inpatient for delivery, and thus were excluded.
b Patients brought to the hospital through the prison system, border control, or other law enforcement agencies could not be reliably followed-up. Also, patients with military insurance are referred out from military hospitals for specific purposes, making them non-representative of the larger population.
Cohort Characteristics by HIE Lookup at Post-Discharge Appointment (N = 8,216)
Differences between the 2 case groups and the control group were statistically significant for all demographic characteristics tested (Table 2). We calculated unadjusted odds ratios for each case group compared with controls whether there was an HIE lookup associated with the index visit (Supplemental Table 2).
Cohort Characteristics by Outcome Group (N = 8,216)
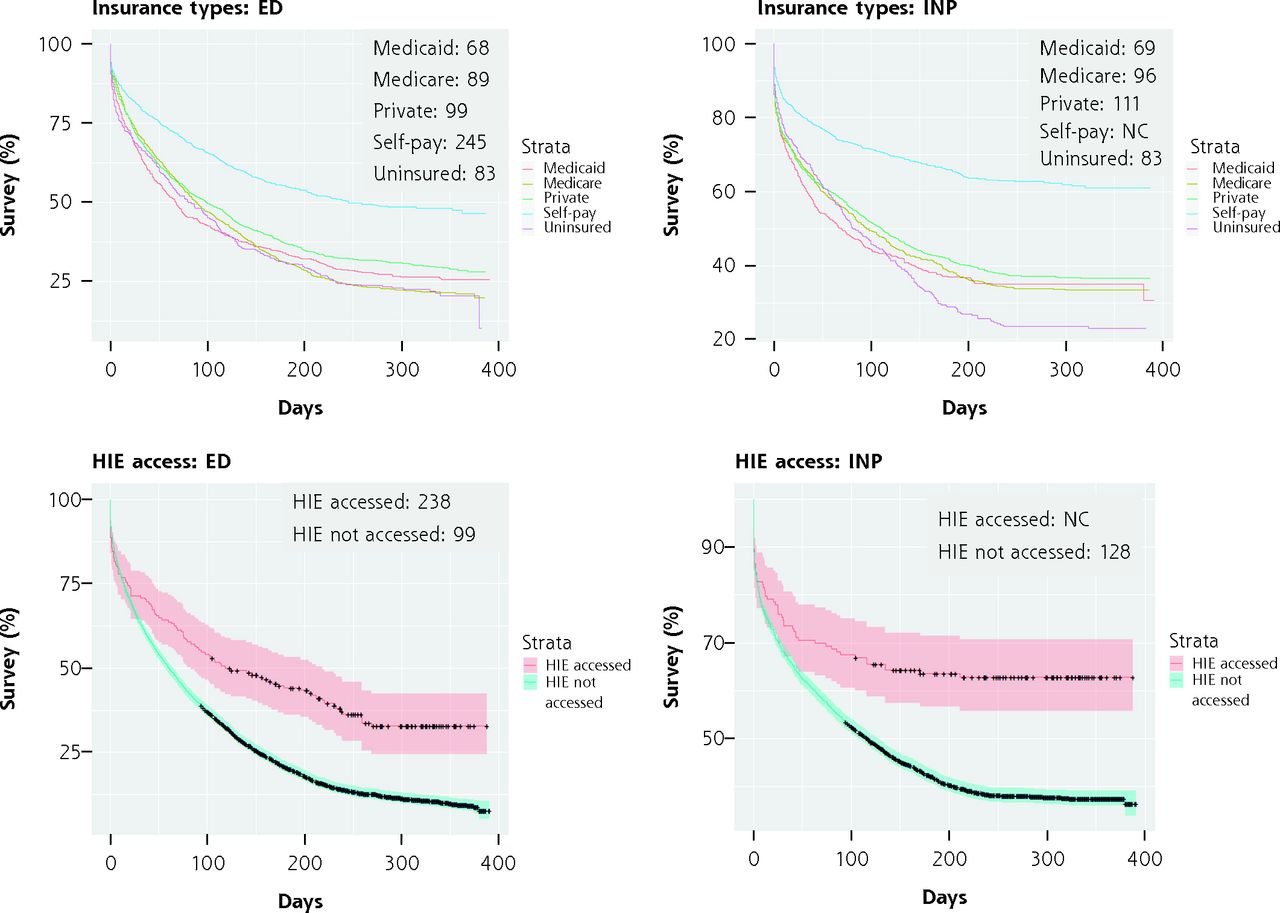
Survival curves showing time until second hospital use by HIE lookup status as well as gender, age category (aged 18-49, and 50 or more years), ethnicity, and insurance categories are shown in Figure 2. After investigating multiple age category breakdowns, the simple 18-49 and 50 or more years seemed to best demonstrate differences. Shorter times for both ED and rehospitalization groups were seen for females, Hispanics, and persons for whom the HIE was not accessed by their primary care physician. The median time to second hospital use is shown as text in the upper right corner of each plot.

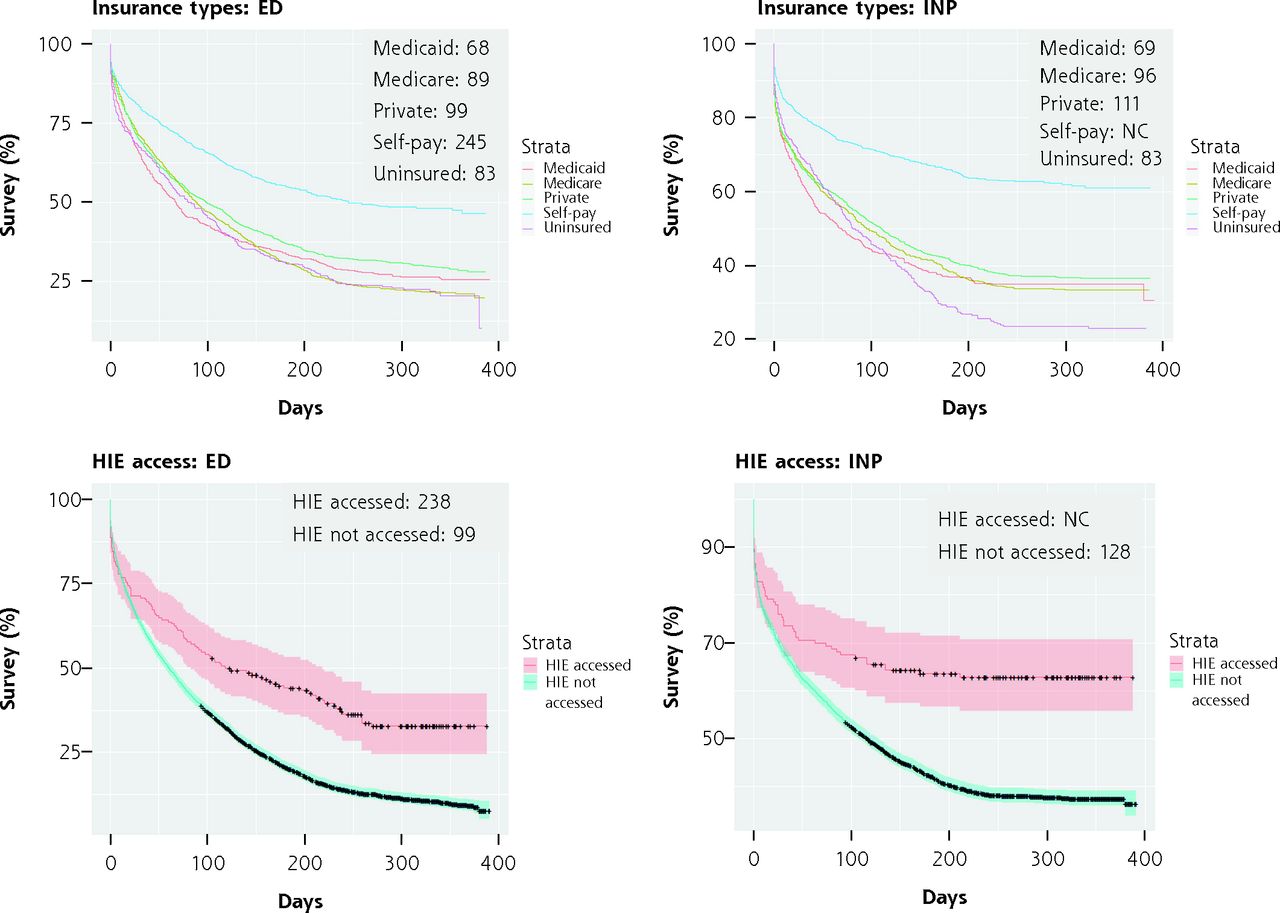
Survival curves for key characteristics by case group (ED or inpatient visit).
ED = emergency department; F = female; HIE = health information exchange; INP = inpatient; = male; NonHisp = Non-Hispanic; PHIX = Paso del Norte Health Information Exchange.
Note: Censoring events are shown as crosses and CIs are included except for insurance categories, for ease of viewing. Time (x axis) is in days. Median number of days to second hospital visit for each group are shown in the upper right corner of the plot. If the number of persons re-entering the ED or INP never drops below 50%, the median cannot be calculated.
Cox proportional hazards models for both ED and rehospitalization case groups are shown in Table 3. Reference groups were female gender, age 18 to 49, Hispanic ethnicity, Medicaid insurance category, and not having the HIE accessed by the primary care physician.
Cox Proportional Hazards Results by Case Group
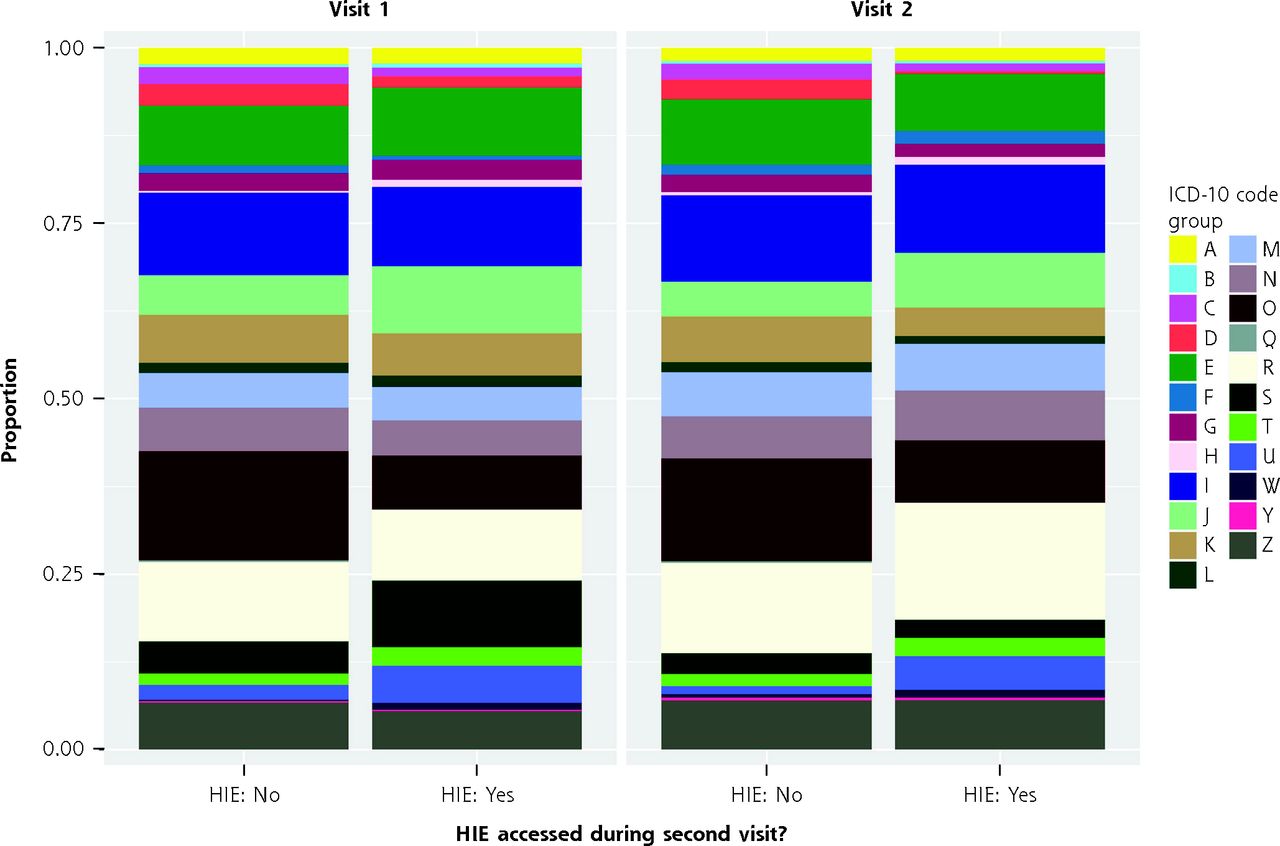
The proportion of ICD-10 code groups reported during hospital visits 1 and 2, divided by whether the HIE was accessed by a primary care physician between those 2 visits is shown in Figure 3. They are further delineated for all variables in the Cox proportional hazards model in Supplemental Figure 3. Some persons had only 1 ICD-10 code, while others had multiple. Therefore, this should not be interpreted as a proportion of the persons who had certain ICD-10 code groups associated with their hospital discharge. A proportions statistical test identified a statistically significant difference between the proportions of different ICD-10 codes for whom the HIE was accessed and for those for whom the HIE was not accessed. This was primarily driven by the proportions of persons with ICD-10 code group “O” (associated with maternal care) being looked up in the HIE by a primary care physician less often.
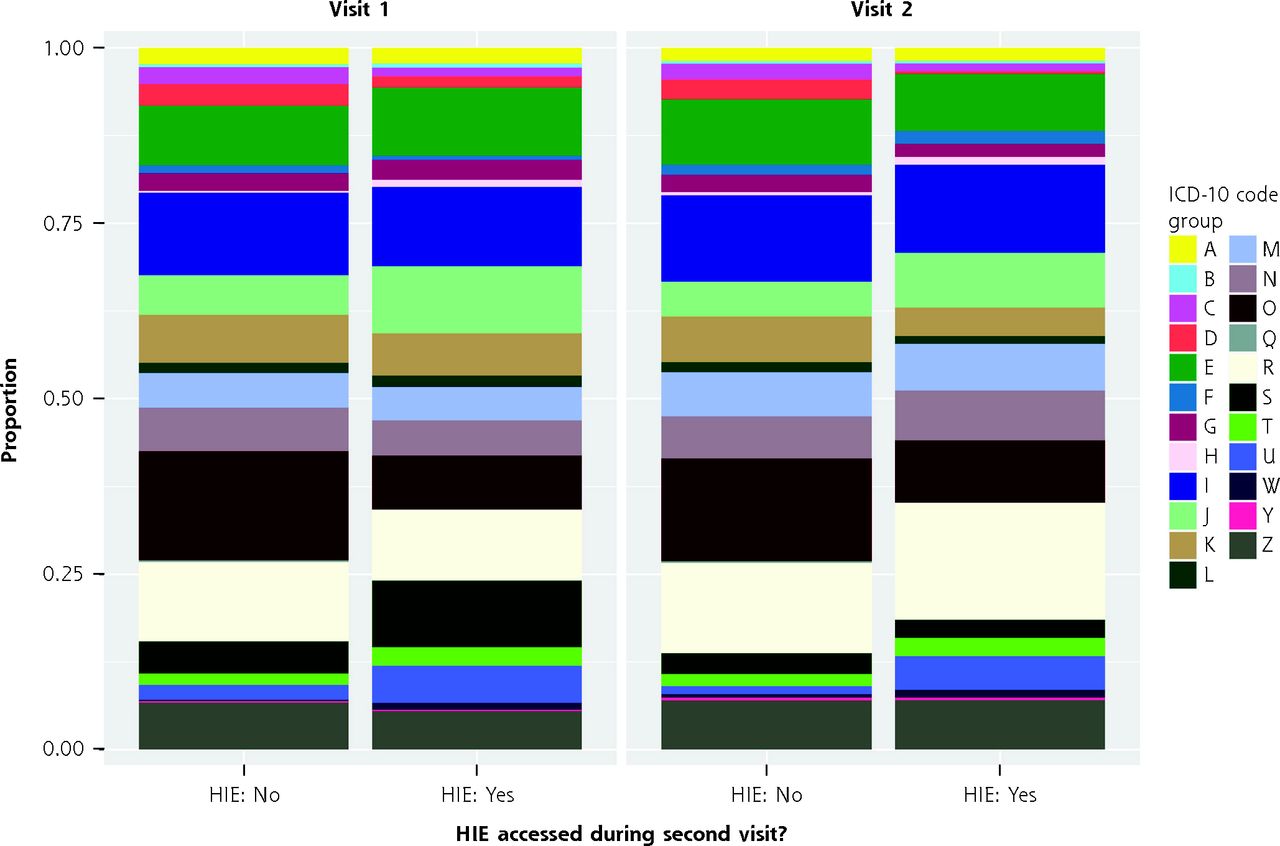
Proportion of ICD-10 code groups reported during hospital visits and physician use of HIE.
ED = emergency department; HIE = health information exchange; ICD-10 = International Statistical Classification of Diseases, 10th Revision.
Note: Graphic represents the proportion of ICD-10 code groups reported during hospital visits, divided by the first inpatient visit and the second visit (ED or inpatient combined, cases only), and whether the HIE was accessed between the first and second visit by a primary care physician. A similar chart for all variables in the model is included in Supplemental Figure 3.
DISCUSSION
This study gives important insight to the direct benefit HIE use can have on patient outcomes. When primary care physicians looked up patients in PHIX, patients were 50% less likely to reutilize the hospital in the follow-up window. And if the hospital was reutilized, the median length of time to the subsequent hospital visit more than doubled. These findings are remarkable, and match those found in a similar study in Rochester, New York,14 that found a lower adjusted odds ratio of hospital readmission of 57% if patients were looked up in an HIE within 30 days after hospital discharge. Despite some differences in study design, population, and system organization, our finding of a 50% decrease in readmission is similar. Together, these studies provide evidence of generalizability and deserve follow-up by other community HIEs, including those serving rural or otherwise underserved populations.16
We found about 3% of patients who saw their primary care clinician within 30 days after discharge were looked up in PHIX. This means under-utilization of PHIX by El Paso primary care physicians is a hurdle for improving outcomes via the HIE. Low engagement with HIEs by US clinicians is a chronic problem despite widespread adoption of EHRs.17 Some physicians use the HIE as standard practice, which likely accounts for most lookups, while others never use it.
There are many possible explanations for under-utilization of PHIX and other HIEs. A primary reason is that the structure provides passive communication between providers. Patients may not disclose a recent hospital visit to their primary care physician when asked or their primary care physician may fail to ask. A solution PHIX is pursuing is more active communication by means of an alert system to notify primary care physicians when a patient is admitted to the hospital. Increasing engagement with HIEs may also be aided through task-sharing with other clinical or administrative staff (eg, medical assistants, nurses, etc.).
A second finding from cohort analysis was that only a small portion (16%) of persons in El Paso who were discharged from hospital inpatient visits had a follow-up appointment with their primary care physician within 30 days. This is an undercount because not all primary care physicians in El Paso are part of the PHIX system. This is one of the weaknesses of the study and placed some limits on cohort size. We suspect, that despite incomplete data capture, there is a need for increased efforts to be sure patients visit their primary care physicians promptly for follow-ups.
Other findings that deserve investigation are the patterns of increased length of time between hospital uses by persons who self-pay. Although self-pay is defined differently within different hospital systems across the country,12,13,18-20 in El Paso it is an indicator used specifically by certain hospital providers for persons who are lower income and lack insurance. Persons in our study categorized as uninsured, however, had a median 83 days before hospital reuse, while it was 245 days for persons categorized as self-pay. The reason for the difference is unclear and worthy of further study.
Women may reutilize the hospital more for necessary non-standard maternal care, indicated by the high number of ICD-10 codes of type “O” looked up less often in the HIE. There is potentially great benefit for maternal care in increasing HIE usage in obstetrics and gynecology. Men took longer before reutilizing the hospital, as did persons of any gender who self-identified as non-Hispanic. There may be interactions between culture and gender that merit further study. For example, other studies suggest Hispanic/Latine men are less likely to seek medical care.21 This aligns with our finding that men took longer before reutilizing the hospital, but not findings among non-Hispanics. Age showed a stronger association with ED use than inpatient readmission; both were significant in the model. A reason for the difference may be increased use of rehabilitation, assisted living, nursing home, and other systems that assist in transitioning care for older adults.
This study was specifically designed to answer the question “Is there evidence of an association between HIE lookup and increased time to next hospital use?” which presents several limitations. First, while we had strong reason to believe that primary care physicians were looking up hospital records when they visited their patient’s profiles (it being their most recent health care interaction), we cannot be sure of this. We further cannot tell how in-depth the physician’s review of the records were, or exactly what changes to care were subsequently made. This must be the province of further studies using different methods, such as chart review.
The strengths of this study lie in the completeness of PHIX data and our ability to analyze the length of time to hospital reuse across a large population. We examined the data broadly to determine if any population-level associations could be identified, or if, in the many crossroads that occur during patient care, the influence of lookup of a patient in an HIE was simply lost. We are encouraged by our findings to further study why there is potentially a link between this one moment in a physician’s office and a longer time to hospital reuse.
CONCLUSIONS
Much more research into the health benefits of HIEs and the communication about the benefits to primary care physicians and patients is needed for HIEs to become established components of the US health care system. So far, it seems that community HIEs such as PHIX are successful in receiving data, integrating it, and making it available to primary care physicians. When used, the information can be remarkably beneficial to increasing the time to future hospital use. Increased support of community HIEs by clinicians is needed and could be accomplished with HIE usage becoming part of standard care. More research into potential HIE-related improvements in health care is central to improving such adoption.
Footnotes
Conflicts of interest: E. H. and J. N. are employees of PHIX. J. C. is an unpaid volunteer. C. S-A. is a paid contractor doing research with PHIX. J. G. and S. C. have no conflicts of interest to disclose.
Funding support: Funding for this research was provided by the Paso del Norte Health Information Exchange.
- Received for publication April 27, 2022.
- Revision received August 23, 2022.
- Accepted for publication September 12, 2022.
- © 2023 Annals of Family Medicine, Inc.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.