
Article Figures & Data
Figures
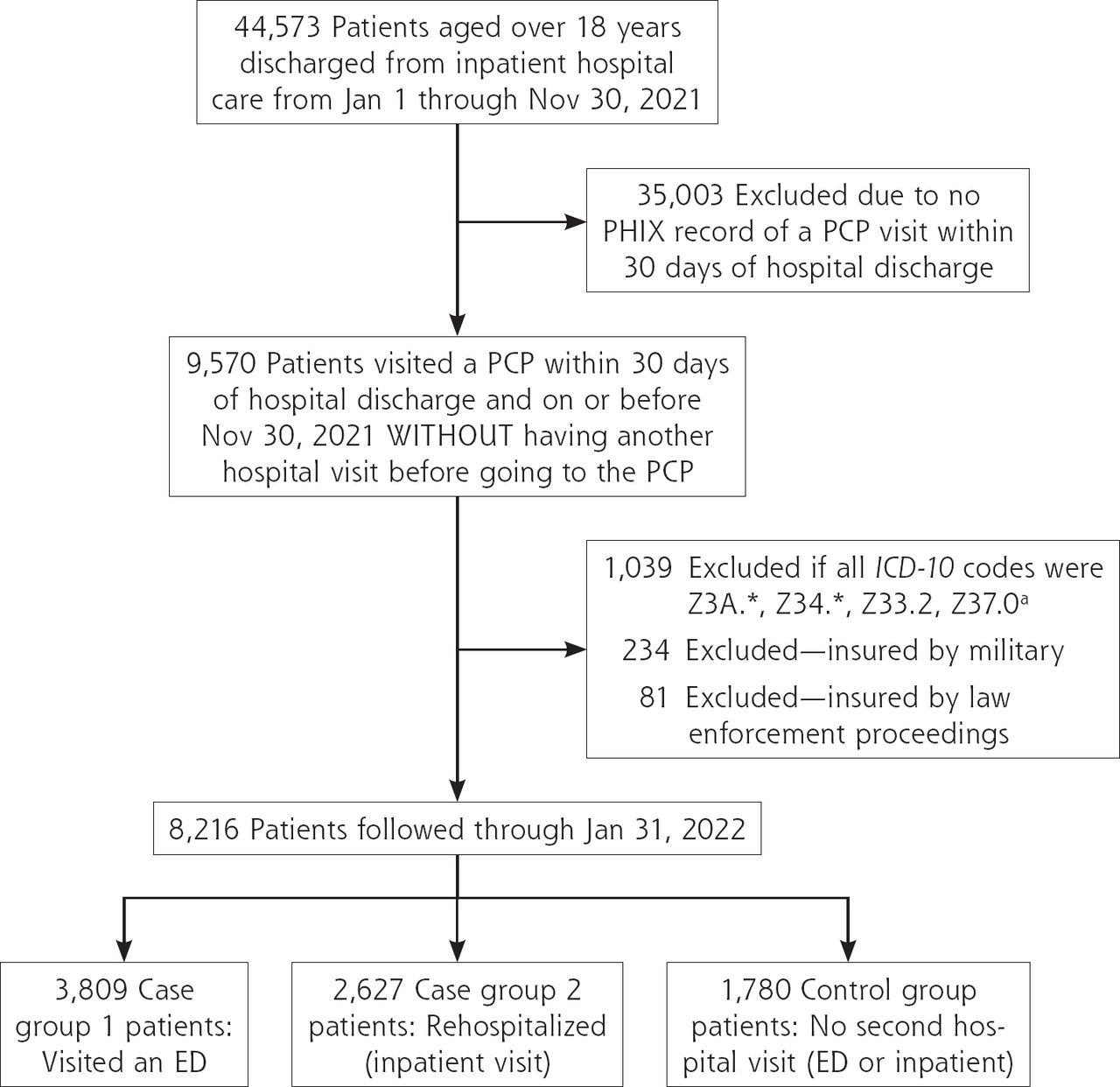
- Figure 1.
Flowchart of cohort and group selection.
ED = emergency department; ICD-10 = International Statistical Classification of Diseases, 10th Revision; PCP = primary care physician; PHIX = Paso del Norte Health Information Exchange.
a These codes were excluded because they indicate normal pregnancy or elective termination of pregnancy. For example, patients with false labor were labeled as inpatient in the system. They were expected to return as inpatient for delivery, and thus were excluded.
b Patients brought to the hospital through the prison system, border control, or other law enforcement agencies could not be reliably followed-up. Also, patients with military insurance are referred out from military hospitals for specific purposes, making them non-representative of the larger population.
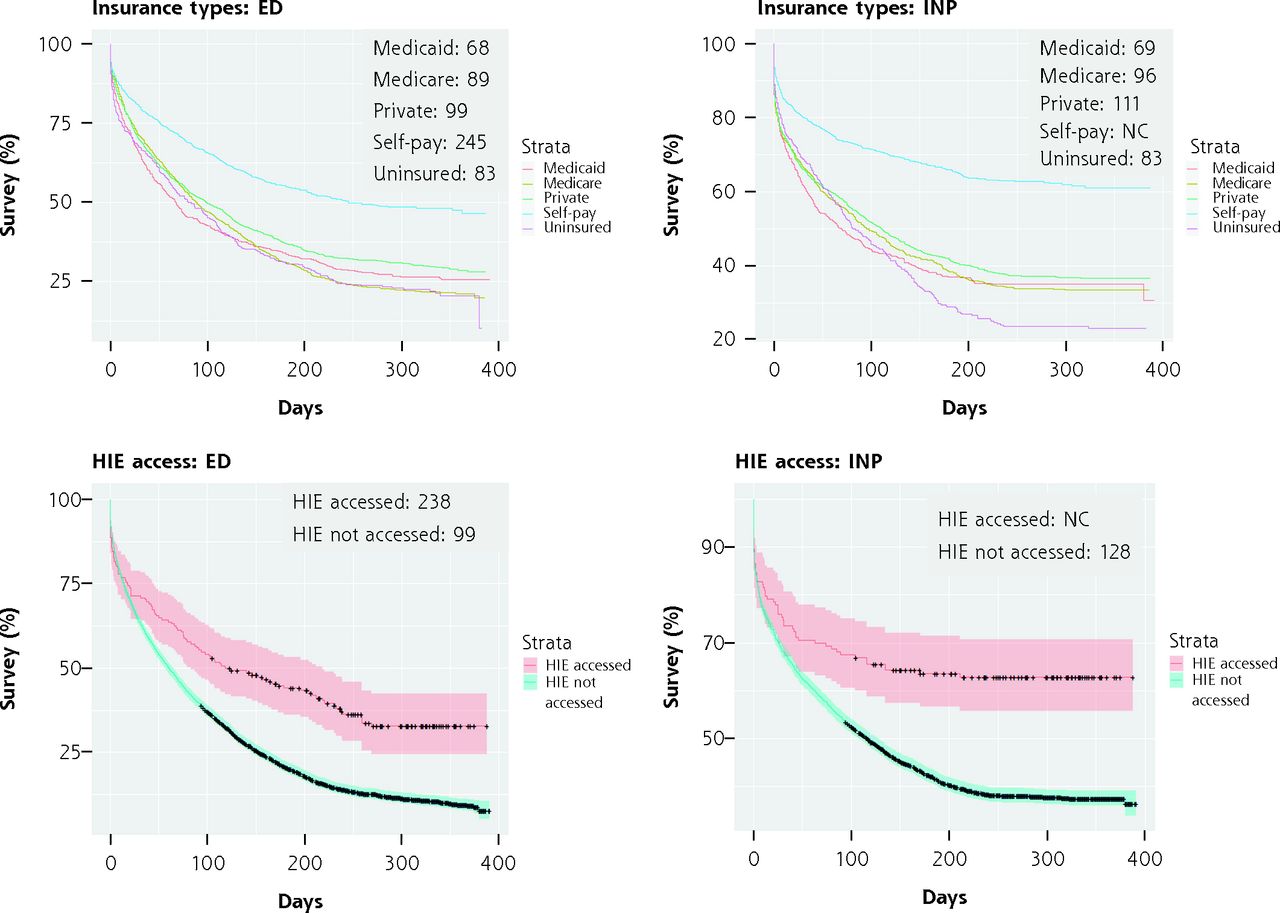
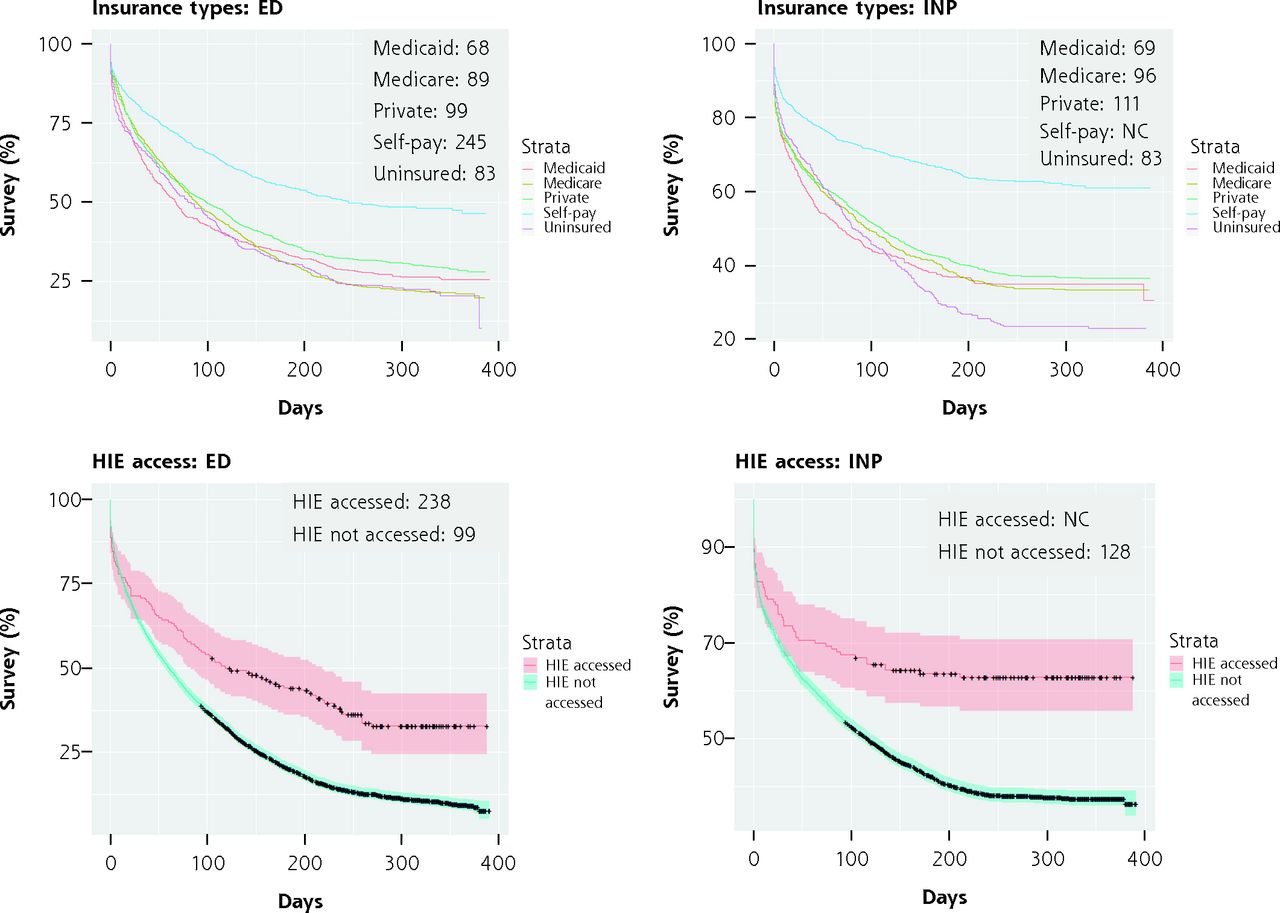
- Figure 2.
Survival curves for key characteristics by case group (ED or inpatient visit).
ED = emergency department; F = female; HIE = health information exchange; INP = inpatient; = male; NonHisp = Non-Hispanic; PHIX = Paso del Norte Health Information Exchange.
Note: Censoring events are shown as crosses and CIs are included except for insurance categories, for ease of viewing. Time (x axis) is in days. Median number of days to second hospital visit for each group are shown in the upper right corner of the plot. If the number of persons re-entering the ED or INP never drops below 50%, the median cannot be calculated.
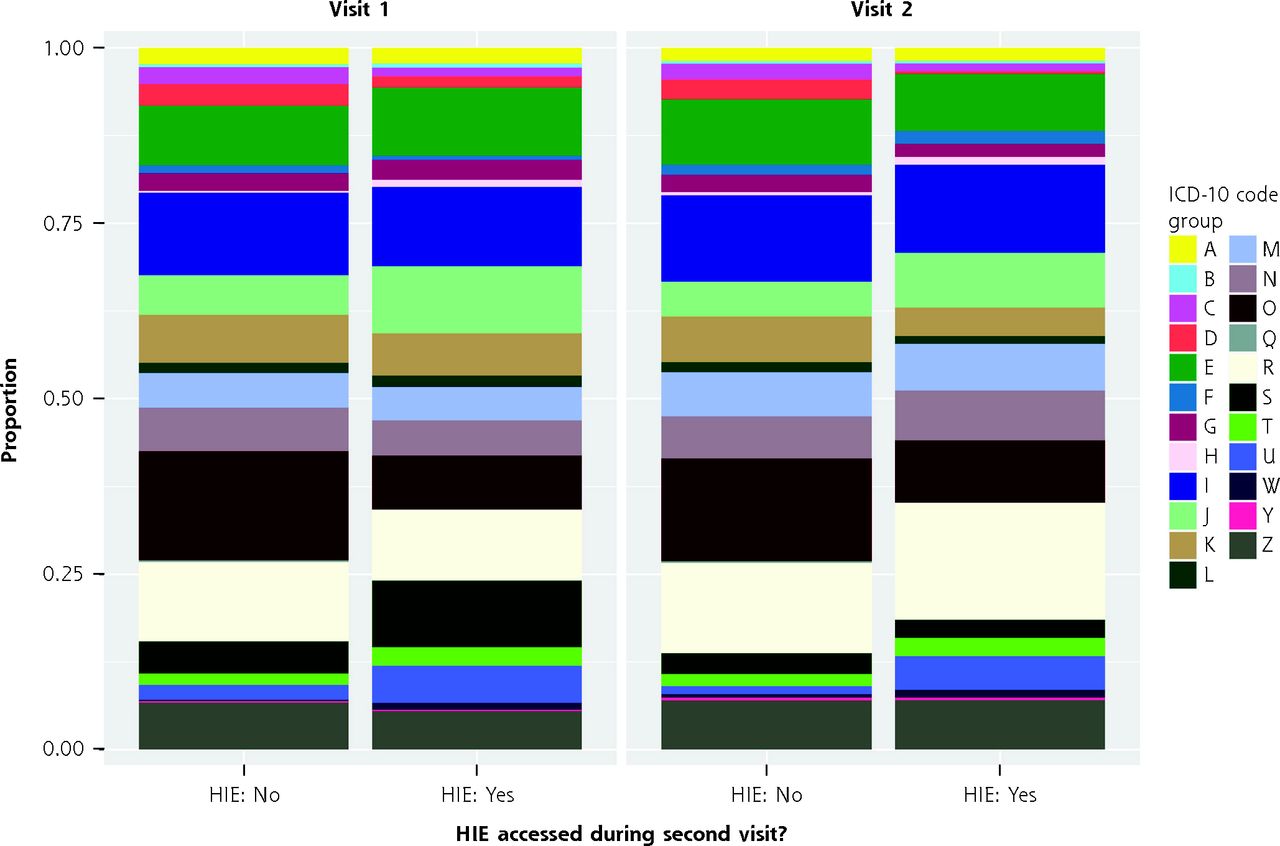
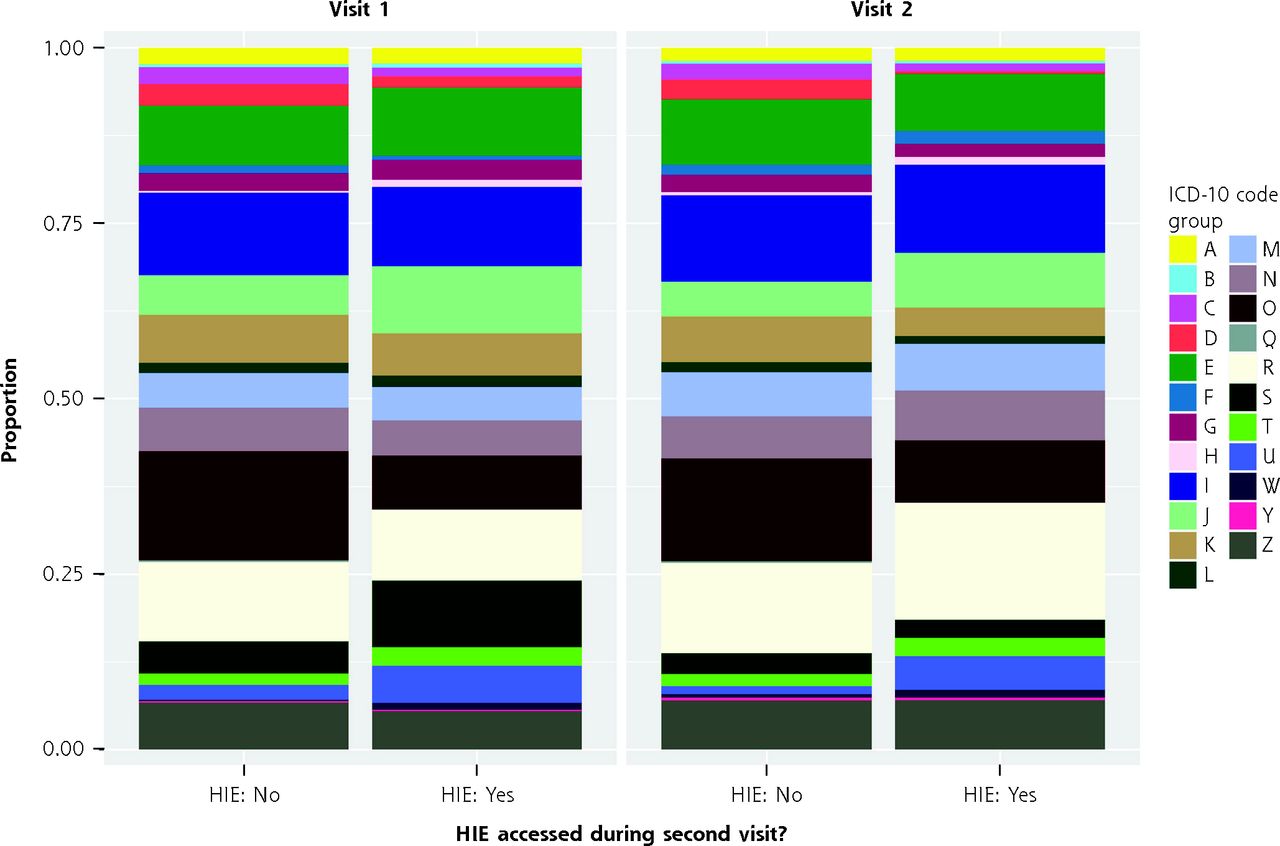
- Figure 3.
Proportion of ICD-10 code groups reported during hospital visits and physician use of HIE.
ED = emergency department; HIE = health information exchange; ICD-10 = International Statistical Classification of Diseases, 10th Revision.
Note: Graphic represents the proportion of ICD-10 code groups reported during hospital visits, divided by the first inpatient visit and the second visit (ED or inpatient combined, cases only), and whether the HIE was accessed between the first and second visit by a primary care physician. A similar chart for all variables in the model is included in Supplemental Figure 3.


Tables
Characteristic HIE Lookup
(n = 270)No HIE Lookup
(n = 7,946)P
ValueGender, No. (%) .09 Female 151 (56) 4,860 (61) Male 119 (44) 3,085 (39) NA 0 (0) 1 (0) Age, y, No. (%) .60 18-49 115 (43) 3,245 (41) ≥50 155 (57) 4,701 (59) Ethnicity, No. (%) <.001a Hispanic 153 (57) 5,611 (71) Non-Hispanic 54 (20) 1,083 (14) NA 63 (23) 1,252 (16) Insurance status, No. (%) .57 Medicaid 33 (12) 1,049 (13) Medicare 63 (23) 1,929 (24) Private 75 (28) 2,368 (30) Self-pay 52 (19) 1,236 (16) Uninsured 24 (9) 705 (9) NA 23 (9) 659 (8) Patient days, median, (IQR) 108 (11-256) 66 (11-169) <.001a HIE = health information exchange; IQR = interquartile range; NA = not available.
↵a Significance level 0.001
Characteristic Case Group 1:
ED Visit
(n = 3,809)Case Group 2:
Inpatient Visit
(n = 2,627)Controls: No
Second Hospital
Visit (n = 1,780)P Value Gender, No. (%) <.001b Female 2,441 (64) 1,661 (63) 909 (51) Male 1,367 (36) 966 (37) 871 (49) NA 1 (0) 0 (0) 0 (0) Age, y, No. (%) <.001b 18-49 1,411 (37) 1,111 (42) 838 (47) ≥50 2,398 (63) 1,516 (58) 942 (53) NA 0 (0) 0 (0) 0 (0) Ethnicity, No. (%) .003a Hispanic 2,498 (66) 2,005 (76) 1,261 (71) Non-Hispanic 465 (12) 370 (14) 302 (17) NA 846 (22) 252 (10) 217 (12) Insurance status, No. (%) <.001b Medicaid 509 (13) 368 (14) 205 (12) Medicare 1,038 (27) 616 (23) 338 (19) Private 1,095 (29) 831 (32) 517 (29) Self-pay 484 (13) 293 (11) 511 (29) Uninsured 323 (8) 302 (11) 104 (6) NA 360 (9) 217 (8) 105 (6) HIE accessed, No. (%) <.001b Yes 107 (3) 60 (2) 103 (6) No 3,702 (97) 2,567 (98) 1,677 (94) Patient days, median (IQR) 43 (10-108) 26 (2-88) 290 (207-343) <.001b ED = emergency department; HIE = health information exchange; IQR = interquartile range; NA = not available.
Note: Outcome groups were based on whether a patient visited an ED or was rehospitalized (inpatient visit) for the same or similar symptoms as indicated by the ICD-10 codes from first hospital discharge.
↵a Significance level 0.01
↵b Significance level 0.001
Characteristic Case Group 1: ED Visit (n = 3,809) Case Group 2: Inpatient Visit (n = 2,627) Coefficient HR (LCI, UCI) P Value Coefficient HR (LCI, UCI) P Value Gender Female Reference Reference Reference Reference Reference Reference Male −0.26 0.77 (0.71, 0.84) <.001c −0.28 0.75 (0.69, 0.82) <.001c Age, y 18-49 Reference Reference Reference Reference Reference Reference ≥50 0.17 1.18 (1.08, 1.3) <.001c 0.13 1.13 (1.02, 1.26) .02a Ethnicity Hispanic Reference Reference Reference Reference Reference Reference Non-Hispanic −0.20 0.82 (0.73, 0.91) <.001c −0.17 0.84 (0.75, 0.95) .004b Insurance type Medicaid Reference Reference Reference Reference Reference Reference Medicare −0.13 0.88 (0.76, 1.02) .08 −0.10 0.91 (0.77, 1.07) .24 Private −0.22 0.81 (0.71, 0.91) <.001c −0.17 0.84 (0.74, 0.96) .01a Self-pay −0.71 0.49 (0.43, 0.57) <.001c −0.94 0.39 (0.33, 0.46) <.001c Uninsured 0.00 1 (0.85, 1.17) 1.00 0.04 1.04 (0.88, 1.23) .65 HIE accessed No Reference Reference Reference Reference Reference Reference Yes −0.53 0.59 (0.46, 0.76) <.001c −0.59 0.56 (0.42, 0.74) <.001c ED = emergency department; HIE = health information exchange; HR = hazard ratio; LCI = lower confidence interval; UCI = upper confidence interval.
Note: The dependent variables are being rehospitalized (inpatient visit) or having an ED visit after the post-inpatient primary care physician visit. Independent variables are whether the HIE was accessed, insurance category, age, ethnicity, and gender.
↵a Significance level 0.05
↵b Significance level 0.01
↵c Significance level 0.001
SUPPLEMENTAL MATERIALS IN PDF FILE BELOW
- Sloan.pdf -
PDF file
- Sloan.pdf -
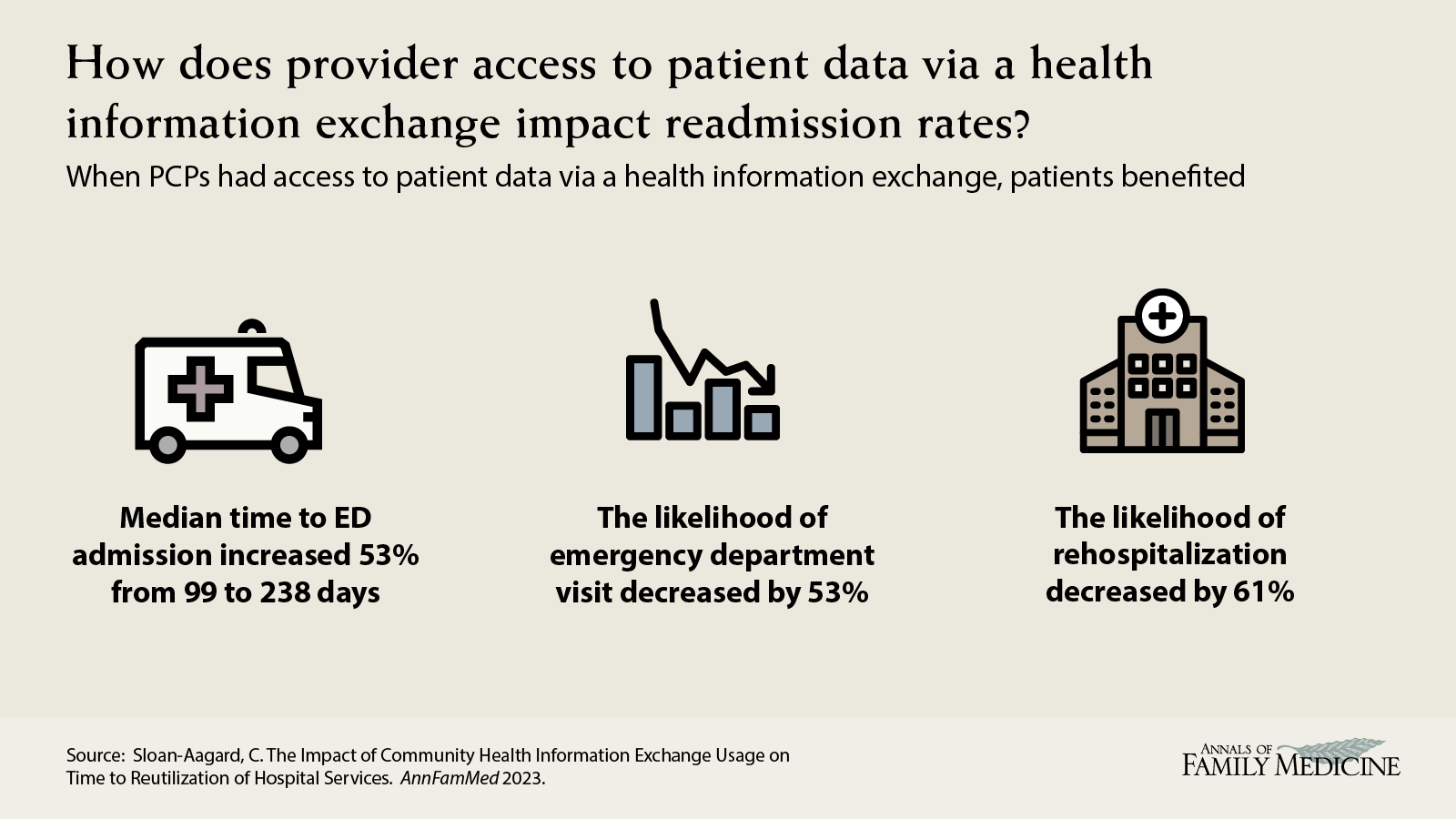
VISUAL ABSTRACT IN PNG FILE BELOW
- 21.1_Sloan-Aargard_visualabstract_v06.png -
PNG file
- 21.1_Sloan-Aargard_visualabstract_v06.png -
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.