
Abstract
PURPOSE We assessed low-dose computed tomography (LDCT) screening for lung cancer using a proactive patient education/recruitment program.
METHODS We identified patients aged 55-80 years from a family medicine group. In the retrospective phase (March-August, 2019), patients were categorized as current/former/never smokers, and screening eligibility was determined. Patients who underwent LDCT in the past year, along with outcomes, were documented. In the prospective phase (2020), patients in the same cohort who did not undergo LDCT were proactively contacted by a nurse navigator to discuss eligibility and prescreening. Eligible and willing patients were referred to their primary care physician.
RESULTS In the retrospective phase, of 451 current/former smokers, 184 (40.8%) were eligible for LDCT, 104 (23.1%) were ineligible, and 163 (36.1%) had an incomplete smoking history. Of those eligible, 34 (18.5%) had LDCT ordered. In the prospective phase, 189 (41.9%) were eligible for LDCT (150 [79.4%] of whom had no prior LDCT or diagnostic CT), 106 (23.5%) were ineligible, and 156 (34.6%) had an incomplete smoking history. The nurse navigator identified an additional 56/451 (12.4%) patients as eligible after contacting patients with incomplete smoking history. In total, 206 patients (45.7%) were eligible, an increase of 37.3% compared with the retrospective phase (150). Of these, 122 (59.2%) verbally agreed to screening, 94 (45.6%) met with their physician, and 42 (20.4%) were prescribed LDCT.
CONCLUSIONS A proactive education/recruitment model increased eligible patients for LDCT by 37.3%. Proactive identification/education of patients desiring to pursue LDCT was 59.2%. It is essential to identify strategies that will increase and deliver LDCT screening among eligible and willing patients.
INTRODUCTION
Lung cancer is the leading cause of cancer-related mortality and accounts for an estimated 22% of all cancer deaths.1 In 2011, the National Lung Screening Trial (NLST) showed a crucial 20% decrease in lung cancer mortality with annual low-dose computed tomography (LDCT) screening.2 The NLST prompted the US Preventive Services Task Force (USPSTF) in 2013 to recommend annual lung cancer screening with LDCT for adults aged 55-80 years with a ≥30 pack-year smoking history and being a current smoker/having quit within the past 15 years.3 The Centers for Medicare and Medicaid Services issued a national coverage determination in 2015 that provides Medicare coverage of screening for lung cancer with LDCT.4
Despite Medicare coverage, only 3.9% of eligible individuals reported LDCT screening in 2015 on the basis of National Health Interview Survey data,3 and the American College of Radiology Lung Cancer Screening Registry reported that only 2% of 7.6 million eligible individuals were screened in 2016.5 According to the American Lung Association, only 5.7% of high-risk individuals were screened for lung cancer nationally in 2020, indicating that screening rates remain consistently low.6 In comparison, 76.4% of women aged 50-74 years underwent mammography for breast cancer screening in 2019,7 and 73.5% of women aged 21-65 years underwent cervical cancer screening in 2019.8
Possible reasons for lack of LDCT screening uptake include patient and clinician unfamiliarity with LDCT screening, lack of interest in smoking cessation, the stigma associated with smoking, and perception of a poor quality of life if lung cancer is detected. In addition, inadequate time and inadequate staffing to discuss LDCT screening have been shown to be barriers for primary care physicians (PCPs).9-12 Another distinct aspect of LDCT screening that might affect screening rates is the additional time necessary to discuss the clinical significance of LDCT screening and the required smoking cessation counseling and referral to smoking cessation interventions that are part of shared decision making.
To help physicians identify eligible patients for screening, our program proposes to use a nurse navigator to proactively identify eligible patients for screening from the electronic medical record (EMR) and to contact patients directly to provide preliminary counseling and education on screening and smoking cessation. Patient navigation strategies have been used in cancer care and have been shown to improve screening rates and early diagnosis of disease.13-16 Studies have shown that patient navigation improves screening rates in underserved and vulnerable populations,17 and various navigation metrics have been proposed to assess the quality of navigation in lung cancer screening including screening rate, compliance with follow-up, time to treatment initiation, patient satisfaction, quality of life, biopsy complications, and cultural competency.18
The objective of the present study was to assess LDCT screening rates using a proactive recruitment strategy within a primary care practice, with the aim of identifying and contacting eligible patients and to assist in education and pre-counseling on LDCT screening and smoking cessation.
METHODS
This project was conducted in collaboration with the Department of Family and Community Medicine (DFCM) as well as the Departments of Cardiothoracic Surgery and Pulmonology and was funded by a research grant from the Simmons Cancer Institute at Southern Illinois University School of Medicine. For this pilot study, a group of 4 family medicine physicians working with the DFCM agreed to participate. The DFCM is a federally qualified health center that provides comprehensive primary care services to underserved communities in south-central Illinois. The data were collected from a cohort of patients who attended this facility; most are from rural areas. The project was conducted from March 2019 to August 2020 and was determined to be a nonhuman subjects project by the Springfield Committee for Research Involving Human Subjects. We generated a list of patients aged 55-80 years from the patient pool of the 4 family medicine physicians, and we conducted the study in 2 phases (retrospective and prospective).
For the retrospective phase, we reviewed EMRs from March to August 2019 for all patients aged 55-80 years who saw any of the 4 family medicine physicians, with the purpose of determining their smoking status. Each patient was then categorized to either the current/former smoker or never smoker group. For current/former smokers, smoking history was determined via chart review, and screening eligibility was determined per the 2013 USPSTF guidelines (current/former smokers who quit ≤15 years ago, ≥30 pack-year smoking history should receive screening computed tomography [CT]). The EMR was then reviewed for all patients eligible for LDCT screening to determine how many underwent LDCT in the past year (1 year before the data collection period) and the outcome of the screening.
The same group of current/former smokers was also used for the prospective phase. The nurse navigator identified patients who were eligible for screening in 2020 and determined how many had already undergone LDCT. The nurse navigator ensured that there was no overlap in the years of screening between the retrospective and prospective phases. If a patient had not undergone LDCT, the nurse navigator contacted them by telephone to provide information about LDCT screening, discuss the importance of lung cancer screening, and to provide preliminary education on shared decision making and smoking cessation counseling. If a patient was inaccessible during the first attempt at contact, the navigator attempted to contact the patient up to 3 more times, and if still inaccessible, they were marked as non-reachable. All eligible patients who were willing to undergo LDCT screening were referred to the office of their respective PCP for a formal shared decision-making clinic visit. The office followed up with eligible patients, and the physician discussed LDCT screening, including the risks and benefits, and prescribed LDCT if the patient was agreeable. The clinic followed up with eligible patients who completed LDCT screening to discuss the next course of action. If a patient declined LDCT screening, the reason was documented.
In addition to screening-eligible patients, the nurse navigator contacted patients who had incomplete smoking history (pack-years) information in the EMR to determine if they qualified for LDCT screening. Any patient who was found to be eligible for LDCT screening after contact with the nurse navigator was counseled in the same manner as other screening-eligible patients. If a patient was agreeable to LDCT screening, the physician’s office followed up in the same manner as described above.
RESULTS
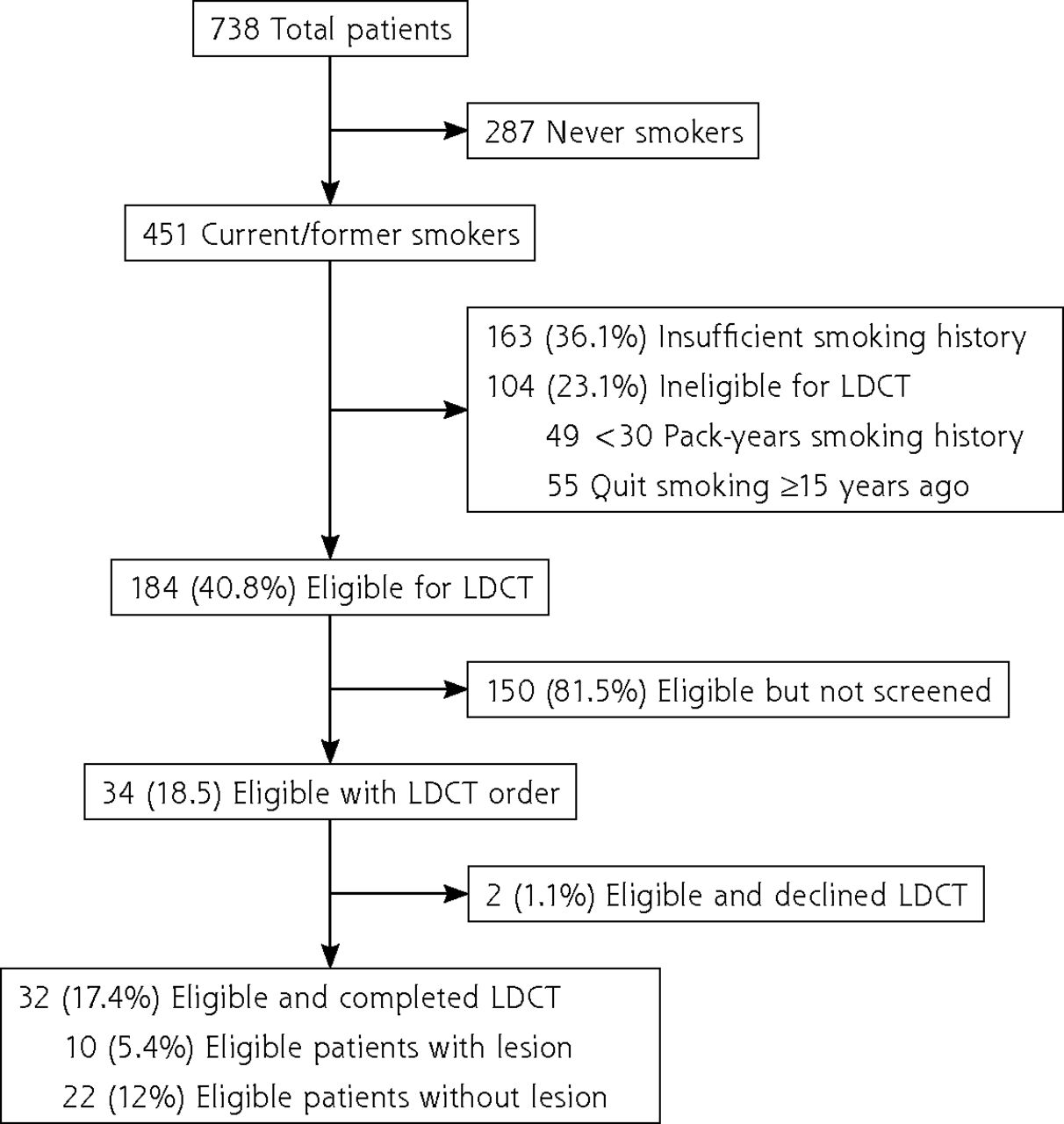
A total of 738 patients aged 55-80 years were identified from the patient pool of the participating family medicine physicians. For the retrospective phase, 451 (61.1%) patients were current/former smokers, and 287 (38.9%) were never smokers and thus not eligible for LDCT screening (Figure 1). The median age of the current/former smokers was 61 years (interquartile range [IQR] 58-66 years), 54.4% were female, 75% were White, 24% were Black, and 1.2% were categorized as other. Almost 99% were non-Hispanic or Latine. Approximately 34% were employed; however, employment status was unavailable for most (60.7%).

Retrospective assessment of patients for LDCT screening.
LDCT = low-dose computed tomography.
Of the 451 current/former smokers, 163 (36.1%) did not have enough information in the EMR to calculate pack-years to determine LDCT eligibility, 104 (23.1%) were not eligible for LDCT screening on the basis of number of pack-years, and the remaining 184 (40.8%) were eligible for LDCT screening. Of the 184 eligible patients, 34 (18.5%) had LDCT ordered, 32 (17.4%) completed LDCT, and 10 (5.4%) had a lesion identified. The remaining 150 eligible patients did not undergo LDCT screening.
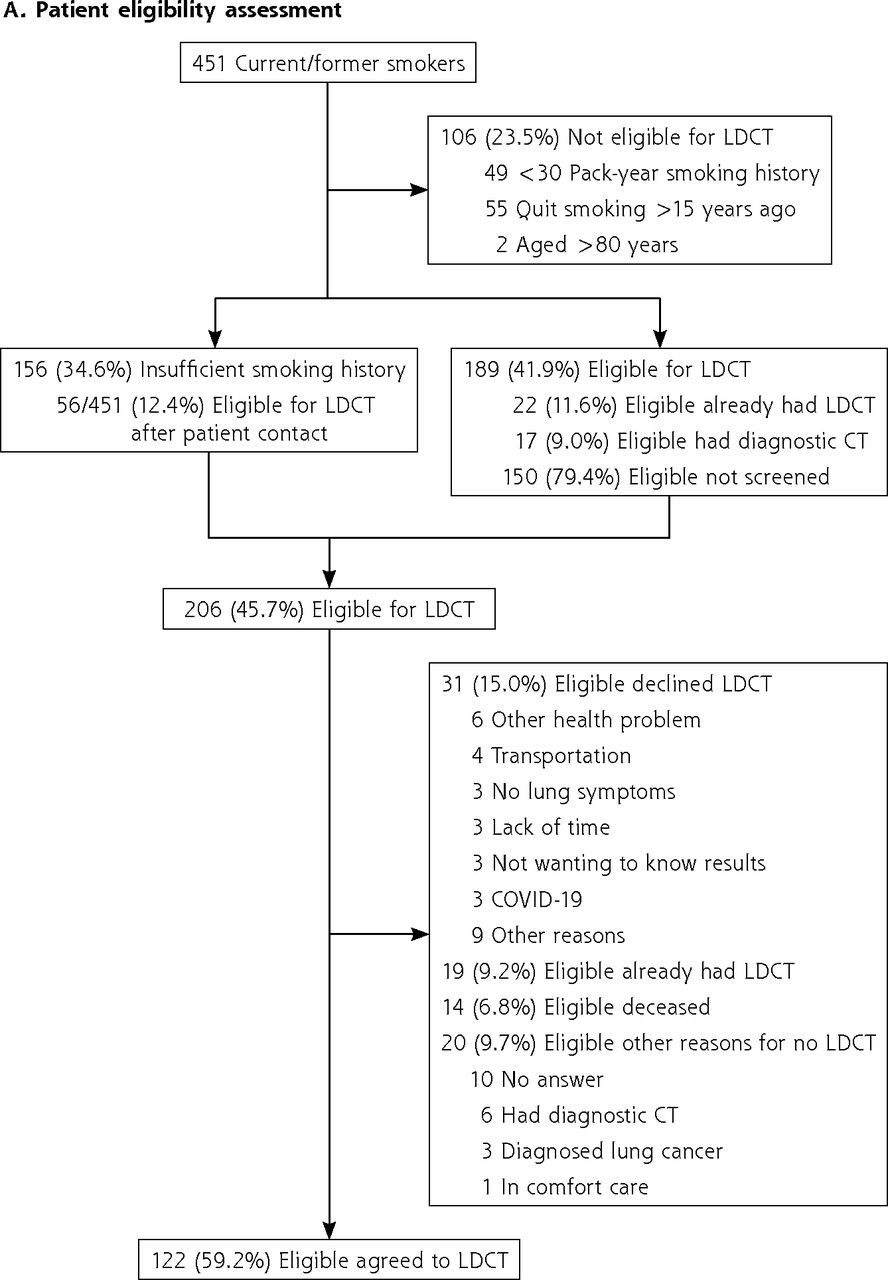
For the prospective phase (in 2020), of the 451 current/former smokers, 189 (41.9%) were eligible for screening (Figure 2A). Compared with the retrospective phase, an additional 5 patients were eligible for screening on the basis of number of pack-years. Of the remaining patients, 106 (23.5%) were ineligible for screening (55 quit smoking >15 years ago, 49 had a <30 pack-year smoking history, 2 were aged >80 years). Of the 189 eligible patients, 22 (11.6%) had completed LDCT in the past year elsewhere, and 17 (9.0%) had a diagnostic chest CT in the past year, leaving 150 (79.4%) eligible for screening.
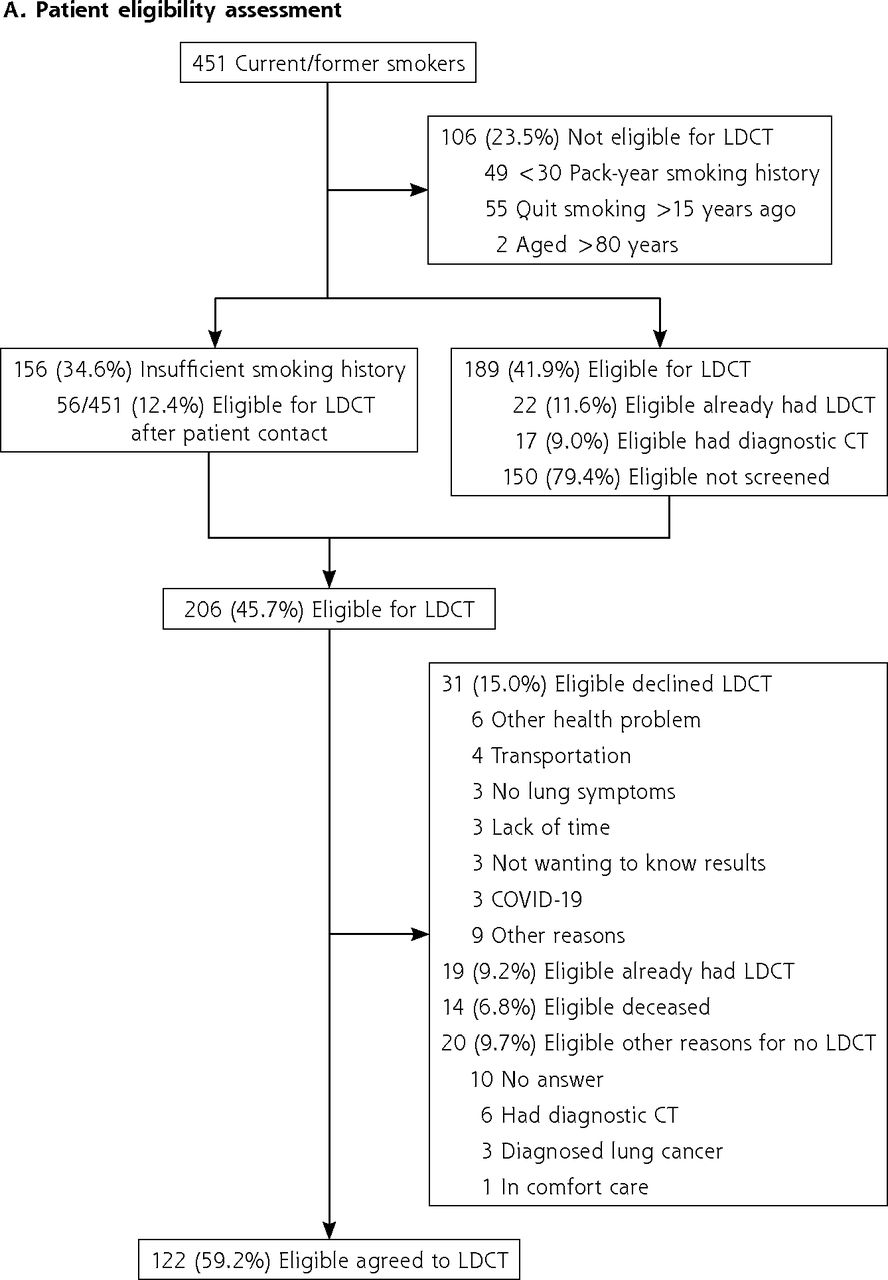

Prospective proactive patient identification/education guided by nurse navigator for LDCT screening.
COVID-19 = coronavirus disease 2019; CT = computed tomography; LDCT = low-dose computed tomography; PCP = primary care physician.
The remaining 156 (34.6%) patients did not have sufficient information in the EMR to calculate pack-years to determine LDCT eligibility (Figure 2A). Compared to the retrospective phase (n = 163), 7 patients had undergone LDCT elsewhere, and this information was documented in the medical records. All 156 patients were called by the nurse navigator to determine smoking history and screening eligibility. The nurse navigator identified an additional 56 (12.4% of 451) eligible patients. Overall, 206 (150 + 56) of 451 patients (45.7%) were eligible for screening in the prospective phase. Compared with the retrospective phase (150), an additional 37.3% patients were identified to be eligible for LDCT with the help of the proactive recruitment initiative.
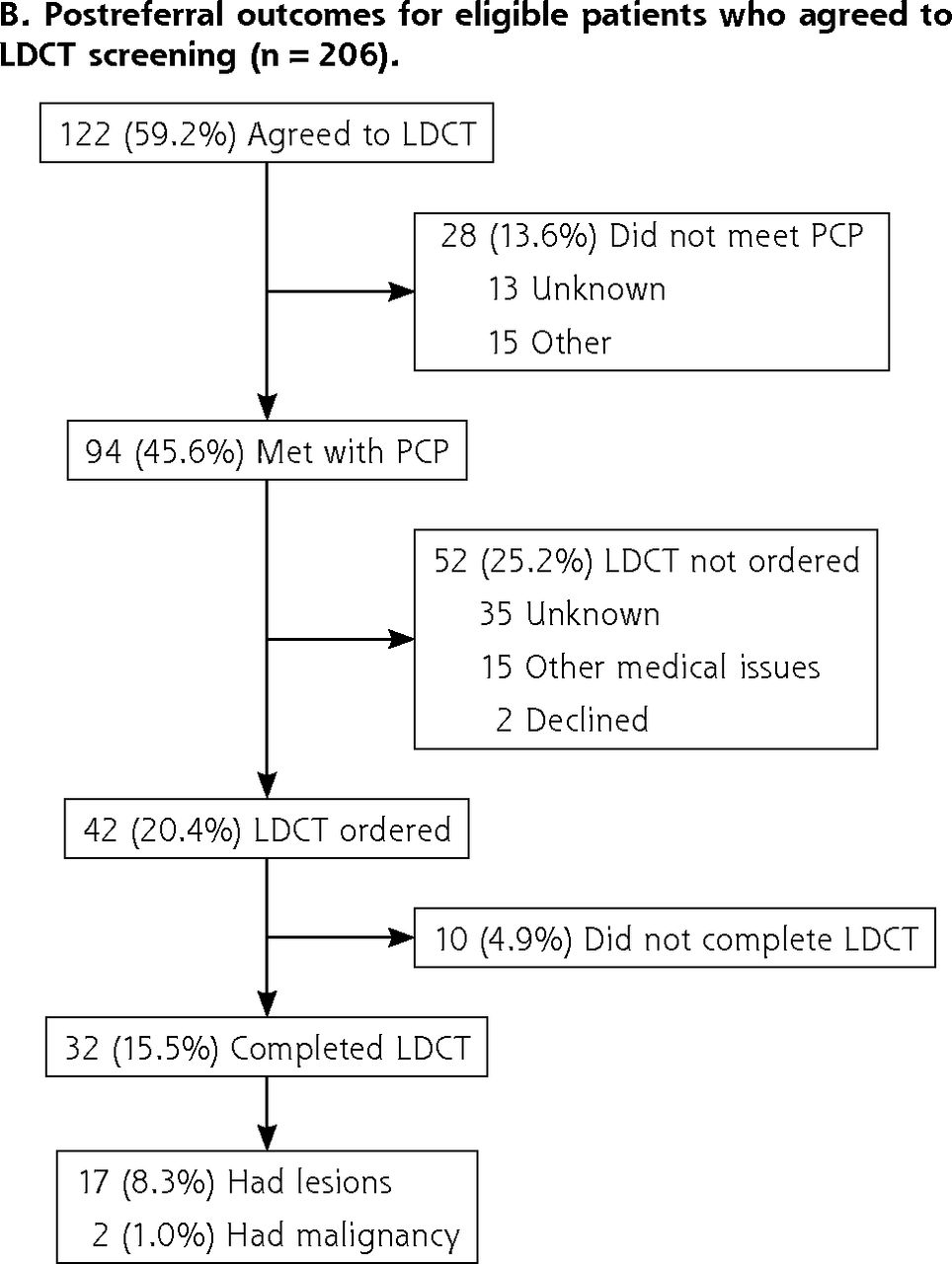
The nurse navigator called all 206 eligible patients to identify how many were agreeable to screening, and 122 (59.2%) verbally agreed, whereas 31 (15.0%) declined LDCT screening (Figure 2A). The most common reasons for declining LDCT included other health problems taking precedence (6), lack of transportation (4), and lack of interest given no obvious lung complaints (3). There were additional outcomes resulting from the nurse navigator contacting all 206 eligible patients. These included the identification of 19 patients (9.2%) who had undergone LDCT with another clinician at the time of the telephone call, which was not documented in the medical records, 14 (6.8%) who were deceased, 10 (4.9%) who were unreachable, and 3 (1.5%) who already had a confirmed diagnosis of lung cancer.
Regarding the overall 206 eligible patients, 94 (45.6%) met with their PCP, 42 (20.4%) were prescribed LDCT, 32 (15.5%) completed LDCT, and 10 (4.9%) did not complete LDCT (Figure 2B). A nodule was identified in 17 (8.3%) patients, and 2 (1.0%) received a confirmed diagnosis of squamous cell carcinoma. The radiologist recommended follow-up CT for the other 15 patients at different time intervals over the next year. The reasons for not placing an order included 35 for an unknown reason and 15 for other medical issues taking precedence; 2 patients declined.
Based on new USPSTF criteria, which were released in 2021 (recommending LDCT screening for adults aged 50-80 years who have a 20 pack-year smoking history and currently smoke or quit within the past 15 years), we identified an additional 17 patients eligible for LDCT, which is an 8.2% increase in eligible candidates compared with the old criteria.
DISCUSSION
With the help of our nurse navigator–driven recruitment strategy, an additional 37.3% of the initial cohort of patients were identified to be eligible for LDCT screening. A total of 59.2% of eligible patients agreed to come to the clinic visit for shared decision making, and 45.6% met with their physician. Comparing assessments without and with the nurse navigator–driven recruitment strategy, the percentage of LDCTs ordered was 18.5% and 20.4%, respectively, the percentage of LDCTs completed was 17.4% and 15.5%, and the percentage of lesions identified requiring follow-up investigation was 5.4% and 8.3%. The nurse navigator was able to identify a greater proportion of eligible individuals for LDCT at the prescreening level. Though the nurse navigator was not directly involved in scheduling the clinic visit or prescribing LDCT, there was a 70% increase in the number of lesions identified in the prospective phase.
In this study, the percentage of patients requiring follow-up evaluation increased from 5.4% to 8.3% with the nurse navigator. In the NLST study, the percentage was 12.8%. Our recruitment initiative used a nurse navigator only for prescreening and identification of eligible patients and was able to identify an additional 12.4% of the 451 patients. Other studies using the Lung CT Screening Reporting and Data System (Lung-RADS) criteria and engaging a navigator for the entire screening process showed that 20% of patients required follow-up for lesions,17-19 but those studies were performed with a more targeted vulnerable population (Veterans Health Administration study and smokers in community health centers) compared to the NLST study and the present study. Engaging the nurse navigator for the entire screening process, from patient identification to follow-up appointments, might improve the number of patients requiring follow-up for lesions in our setting. The present study was conducted in a federally qualified health center that serves most of the rural population in south-central Illinois. The proportion of current/former smokers was 61% in this cohort compared with 14.5% in the whole of Illinois in 2019.20 The results of our study reiterate the need for identifying strategies to decrease smoking burden and providing lung cancer screening in rural regions with a high prevalence of cigarette smoking.
Several barriers have been reported in the literature that influence LDCT uptake by eligible patients. These include transportation, cost, existing comorbidities, caregiver availability, and fear of the results.10 Physician-perceived barriers include uncertainty regarding the benefit of LDCT screening, false-positive results, insurance coverage, cost-effectiveness, unfamiliarity with LDCT screening, and inadequate physician time and staffing to discuss screening.9,21,22 In our cohort and on the basis of patient response, the most common barriers to screening were other health conditions taking precedence over screening, lack of transportation, and lack of interest in screening given no current lung symptoms. With the help of the prescreening consultation with the nurse navigator, nearly 60% of eligible patients verbally agreed to LDCT screening, of whom 45.6% actually met with their PCP to discuss screening. This might suggest that there is a willingness to undergo LDCT screening, and more individuals might comply with screening, provided that barriers associated with clinic visits and shared decision making are addressed.
The prospective phase of the present study was conducted during the coronavirus disease 2019 (COVID-19) pandemic, which might have been an additional contributor to decreased LDCT prescriptions provided by physicians and other health problems taking precedence over LDCT screening. During the COVID-19 pandemic, there was a significant increase in the use of telehealth for patient care. Telehealth has helped patients by resolving issues such as transportation barriers, time away from work, and the necessity of a caregiver to travel along, and more importantly has helped expand health care to rural, underserved regions. Telemedicine (video and/or telephone assisted) along with the help of the type of program described here can proactively identify eligible and willing patients, provide smoking cessation counseling, and help in shared decision making, ultimately increasing the use of LDCT screening. Another potential barrier is the lack of smoking details in the EMRs required to calculate pack-years and assess screening eligibility. In our cohort, 36.1% did not have adequately documented smoking history in the medical records system to determine LDCT screening eligibility. Additional training and better documentation of smoking history in the EMR system and sharing screening records across EMR platforms could decrease health service redundancies and inefficiencies as well as decrease the burden on health care clinicians.
Program sustainability using nurse navigators is an important issue, especially with no standard payment structures for additional navigators.23 Several studies of breast cancer and colorectal cancer have shown that the use of patient navigators is cost-effective, with increased uptake of cancer screening, adherence to yearly screening, and timely diagnosis, treatment, and follow-up.24 There are very few studies assessing the cost-effectiveness of the use of navigators for lung cancer screening, and the results are inconclusive.25,26 A single study of Medicare capitated payment beneficiaries showed cost-effectiveness of a patient navigator model; however, additional evaluation is needed to determine if navigator programs are cost-effective in lung cancer screening in other clinical settings.27 Although we used a nurse navigator only for identifying eligible patients and for prescreening, we did find a marked increase in the number of patients willing to undergo screening, with minimal funding. Our results suggest that lung cancer screening programs with a proactive recruitment strategy and telehealth can increase the number of LDCT screenings among high-risk eligible individuals.
Future lung cancer screening initiatives with this nurse navigator recruitment strategy will be beneficial in identifying eligible patients, providing counseling and shared decision making, scheduling CT screens, reviewing results with patients, and making appropriate referrals for management of any identified pulmonary disease and for follow-up screening. Future studies evaluating the sustainability and cost-effectiveness of such programs are essential.
Footnotes
Conflicts of interest: authors report none.
Read or post commentaries in response to this article.
Funding support: This study was funded by a research grant from the Simmons Cancer Institute, Southern Illinois University School of Medicine.
Previous presentation: 2021 American Cancer Society Virtual Clinical Congress; October 2021; virtual.
- Received for publication January 28, 2022.
- Revision received October 31, 2022.
- Accepted for publication November 21, 2022.
- © 2023 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.