
Abstract
PURPOSE The process and outcomes of delivering medical care for chronic low back pain might affect patient satisfaction. We aimed to determine the associations of process and outcomes with patient satisfaction.
METHODS We conducted a cross-sectional study of patient satisfaction among adult participants with chronic low back pain in a national pain research registry using self-reported measures of physician communication, physician empathy, current physician opioid prescribing for low back pain, and outcomes pertaining to pain intensity, physical function, and health-related quality of life. We used simple and multiple linear regression models to measure factors associated with patient satisfaction, including a subgroup of participants having both chronic low back pain and the same treating physician for >5 years.
RESULTS Among 1,352 participants, only physician empathy (standardized β, 0.638; 95% CI, 0.588-0.688; t = 25.14; P < .001) and physician communication (standardized β, 0.182; 95% CI, 0.133-0.232; t = 7.22; P < .001) were associated with patient satisfaction in the multivariable analysis that controlled for potential confounders. Similarly, in the subgroup of 355 participants, physician empathy (standardized β, 0.633; 95% CI, 0.529-0.737; t = 11.95; P < .001) and physician communication (standardized β, 0.208; 95% CI, 0.105-0.311; t = 3.96; P < .001) remained associated with patient satisfaction in the multivariable analysis.
CONCLUSIONS Process measures, notably physician empathy and physician communication, were strongly associated with patient satisfaction with medical care for chronic low back pain. Our findings support the view that patients with chronic pain highly value physicians who are empathic and who make efforts to more clearly communicate treatment plans and expectations.
INTRODUCTION
Donabedian proposed the triad model of quality-of-care assessment on the basis of structure, process, and outcomes more than 3 decades ago.1 The model remains relevant today, with the evolution of health care delivery and the growing problem of chronic pain management. The Institute of Medicine reported that >100 million Americans had chronic pain in the United States in 2010 and that relieving it should be a national priority.2 Clinical practice guidelines were established to help assure the highest quality of care based on current clinical evidence. The Centers for Disease Control and Prevention issued its guideline for prescribing opioids for chronic pain,3 and the American College of Physicians subsequently published a guideline specifically addressing noninvasive treatments for chronic low back pain.4 Federal strategies were also launched to promote the delivery of optimal pain treatment in the United States. The National Pain Strategy involves a comprehensive population health–level approach aimed at decreasing the burden of pain for patients, their families, and society as a whole.5 Correspondingly, the Federal Pain Research Strategy was developed to guide research planning and funding decisions to fill crucial gaps in the federal pain research portfolio.6
Despite these advances over the past decade, much remains unknown regarding how the patient-physician interaction affects the process of delivering medical care for chronic low back pain and, ultimately, patient satisfaction. Physician communication generally has been considered an important element of chronic pain care, owing to its effect on patient engagement7 and collaborative decision making.8 A collaborative approach involving both patient and physician in clinical decisions has been associated with adherence to pain treatment and better outcomes among patients with chronic low back pain.9 Such interpersonal aspects of the patient-physician relationship reflect patient-centered communication that might also facilitate and enhance patient engagement in chronic pain self-management.7 It is striking that there has been much less research on the role of physician empathy in treating patients with chronic pain because these patients are often compromised and feel misunderstood and isolated.10 A study of patients attending a pain clinic found a strong correlation between reported levels of physician empathy and satisfaction with their consultation.11
Studies have often focused on the bivariate relationship between clinical outcomes and patient satisfaction.12-17 The process of treating chronic low back pain has been less studied, despite the broad variety of practitioner-based interventions available to patients.18 Perhaps this is because assessing patient satisfaction with treatment of chronic pain is complex, involving various patient populations and differing levels of satisfaction with the process and outcomes of care.19,20 Some studies of satisfaction with chronic pain care focus on highly selected populations, such as patients with cancer21,22 or substance abuse,23 and are not generalizable to the broader population of patients with chronic pain. The purpose of the present study was to measure the associations among process, outcomes, and patient satisfaction within the structural framework of general medical care for chronic low back pain provided via an ongoing patient-physician relationship.
METHODS
Study Design and Participants
We conducted a cross-sectional study by selecting all eligible participants from the Pain Registry for Epidemiological, Clinical, and Interventional Studies and Innovation (PRECISION) from April 2016 to April 2022. Registry participants were recruited from the contiguous 48 United States and the District of Columbia, primarily using direct-to-patient advertising on social media. Participants were required to be aged 21-79 years at the time of enrollment and to have sufficient English-language proficiency to complete registry case report forms on a digital research platform, either independently or with staff assistance. In addition, participants must have met the criteria for chronic low back pain established by the National Institutes of Health Task Force on Research Standards for Chronic Low Back Pain24 at the time of enrollment. These criteria consisted of having low back pain for at least the past 3-6 months, and with a frequency of at least half of the days in the past 6 months. Participants also must have reported having a physician who regularly treated their low back pain. Pregnant and institutionalized persons were not eligible for this study. The North Texas Institutional Review Board approved this research, and we obtained informed consent from participants before collecting data. Additional registry details are available at ClinicalTrials.gov.25
Measures of Process, Outcomes, and Patient Satisfaction
We used participant-reported data at registry enrollment to assess 3 process measures, 3 outcomes, and patient satisfaction with medical care for chronic low back pain. Process measures included the Communication Behavior Questionnaire (CBQ),26 Consultation and Relational Empathy (CARE) measure,27 and current physician prescribing of opioids for low back pain. The CBQ is a 23-item instrument that assesses physician communication on 4 scales pertaining to patient participation and orientation, effective and open communication, emotionally supportive communication, and communication about personal circumstances (Cronbach α values for these scales are 0.93, 0.90, 0.88, and 0.91, respectively). Scores range from 0 to 100 on each scale. The CARE measure is a 10-item instrument that assesses physician empathy (Cronbach α = 0.93), with scores ranging from 10 to 50. Higher scores on the CBQ and CARE measure represent better patient perceptions of physician communication skills and physician empathy, respectively.
Outcome measures included the numerical rating scale (NRS) for pain intensity, Roland-Morris Disability Questionnaire (RMDQ)28 for physical function, and SPADE cluster (sleep disturbance, pain interference with activities, anxiety, depression, low energy or fatigue) of the Patient-Reported Outcomes Measurement Information System with 29 items (PROMIS-29)29 for health-related quality of life (HRQOL). The NRS measures average pain intensity for the 7 days before registry enrollment, with scores ranging from 0 (no pain) to 10 (worst pain). The RMDQ consists of 24 items that measure physical function in terms of activities that the participant cannot perform because of low back pain, with scores ranging from 0 (no disability) to 24 (greatest disability). The SPADE cluster consists of 20 items that measure various aspects of HRQOL (4 items for each of the 5 scales). All SPADE scale scores, except sleep disturbance, are normed according to the general US population and have a mean of 50 and SD of 10. The sleep disturbance scale is similarly scored; however, it is normed with a calibration sample enriched for chronic illness. The SPADE cluster score is the mean of its 5 component scales. Higher scores for the SPADE cluster represent greater HRQOL deficits.
We measured patient satisfaction with the general satisfaction scale of the Patient Satisfaction Questionnaire Short-Form with 18 items (PSQ-18).30 This scale includes the following 2 items: “I am very satisfied with the medical care I receive” and “I am dissatisfied with some things about the medical care I receive.” Likert scale responses range from strongly agree to strongly disagree, with scale scores ranging from 1 (lowest satisfaction) to 5 (highest satisfaction) after the appropriate data transformations are performed. This simple scale, which has acceptable internal consistency reliability (0.75) and is highly correlated with the general satisfaction scale on the longer 50-item PSQ (r = 0.92), was used to minimize reporting burden for registry participants. It also avoids measuring satisfaction within other domains (eg, accessibility, convenience, and financial aspects of medical care) that are not inherently related to the contemporary patient-physician relationship.
Statistical Analysis
Data are presented as mean (SD) or number (%). We computed an overall score ranging from 0 to 100 for the CBQ using the mean of its 4 scales. We also performed linear transformations of the CARE measure and the PSQ-18 score for patient satisfaction, yielding scores ranging from 0 to 100, to facilitate direct comparisons with the overall CBQ score. We analyzed correlations within the process and outcome measures with the Pearson correlation coefficient. We used simple and multiple linear regression models for patient satisfaction (dependent variable) to compute unadjusted and adjusted (for potential confounders) standardized β coefficients and 95% CIs. The independent variables in these models included participant demographic characteristics (age, gender, and race); burden of medical comorbidities (derived from the sum of participant-reported diagnoses of herniated disc, sciatica, osteoarthritis, osteoporosis, hypertension, heart disease, diabetes mellitus, asthma, and depression); and the above-described process and outcome measures. We computed variance inflation factors (VIFs) for independent variables in the multivariable model to assess multicollinearity. These statistical methods were repeated among participants in a long-term medical care subgroup to explore the effect of having a long-term patient-physician relationship on the study findings. We managed and analyzed data with IBM SPSS Statistics software, version 28 (IBM Corp) and tested hypotheses at the .05 level of statistical significance using 2-sided tests.
RESULTS
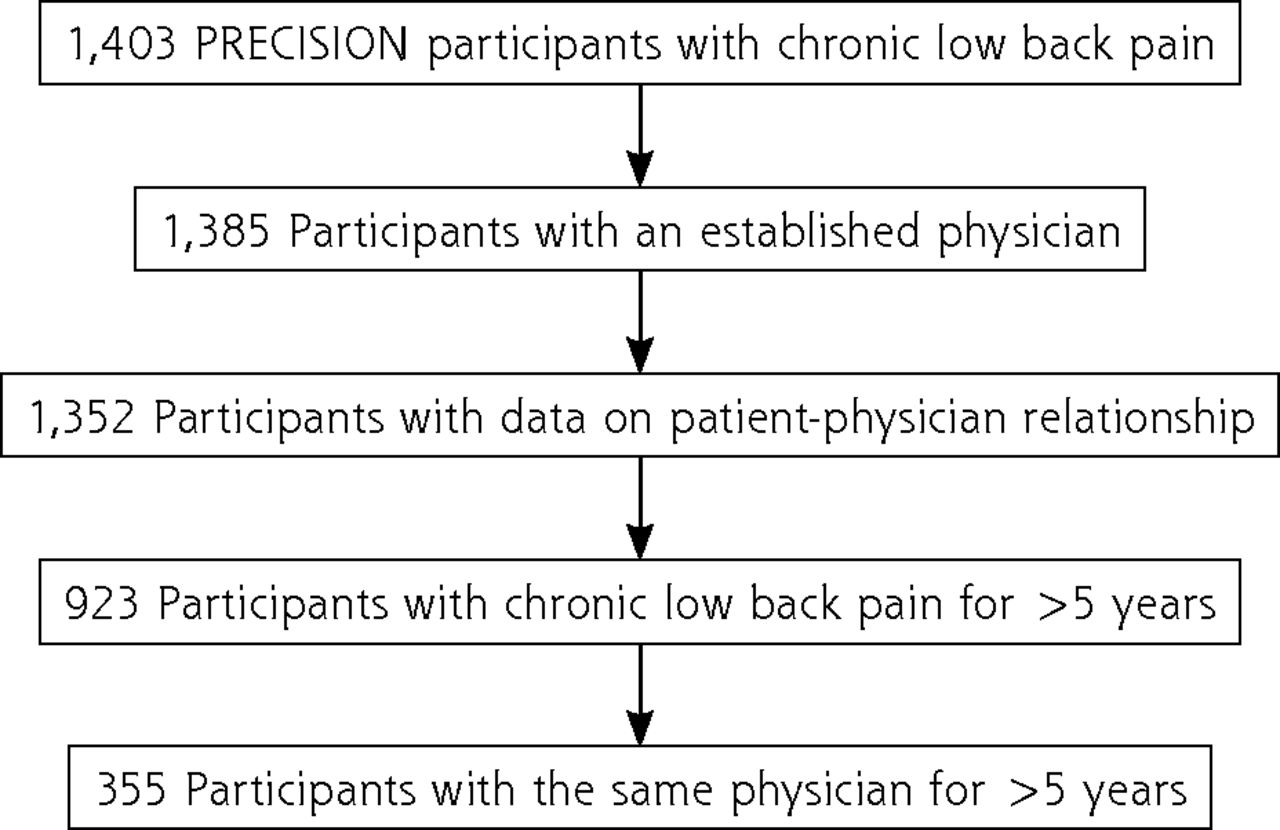
We studied 1,352 participants, including 355 (26.3%) in the long-term medical care subgroup (Figure 1). For the 1,352 participants, the mean (SD) age was 53.3 (13.1) years, 1,009 (74.6%) were female, and 275 (20.3%) represented racial minority groups (Table 1). Depression and sciatica were the most common comorbidities, each reported by half or more of the participants. In the long-term medical care subgroup, the mean age of participants was 56.3 (11.8) years, 255 (71.8%) were female, and 55 (15.5%) represented racial minority groups. More than half of participants in this subgroup reported depression, sciatica, osteoarthritis, and hypertension.
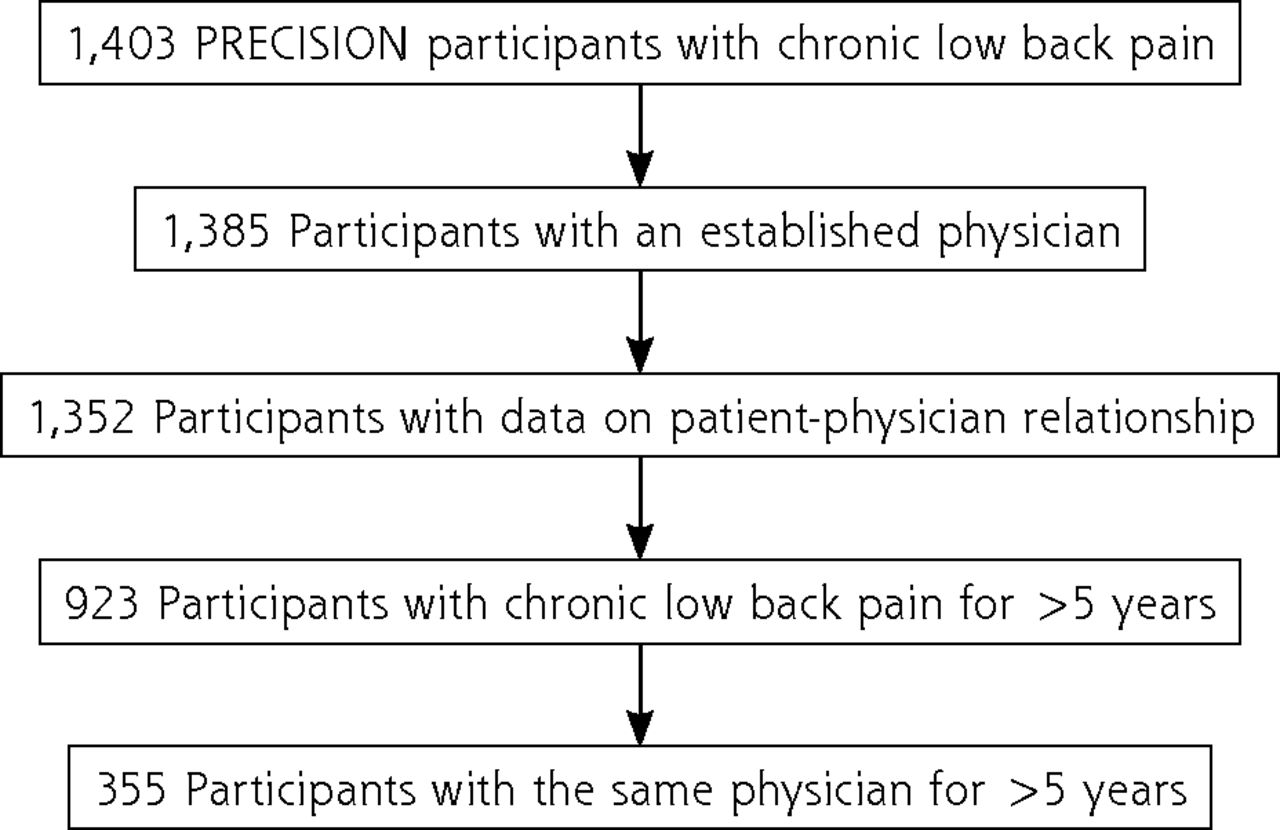
Flow of participants.
PRECISION = Pain Registry for Epidemiological, Clinical, and Interventional Studies and Innovation.
Note: Participants were not required to have a physician who treated their low back pain when the registry was established in 2016, and data on the patient-physician relationship were not routinely collected until later that year.
Participant Characteristics at Registry Enrollment
The mean (SD) physician communication and physician empathy scores were 66.3 (22.4) and 70.9 (29.1), respectively, in the overall sample and 71.1 (22.3) and 74.3 (29.4) in the long-term medical care subgroup (Table 1). A total of 445 (32.9%) participants were currently prescribed opioids for low back pain in the overall sample, compared with 135 (38.0%) in the long-term medical care subgroup. Although participant-reported perceptions of physician communication (r = 0.10; P < .001) and physician empathy (r = 0.06; P = .03) were both correlated with current physician prescribing of opioids, the effect sizes were weak or negligible. There was a much larger effect involving the correlation between physician communication and physician empathy (r = 0.76; P < .001). Similar correlations among the process measures were observed in the long-term medical care subgroup.
The mean (SD) outcome scores in the overall sample were 6.1 (1.8) on the NRS for pain intensity, 14.5 (5.7) on the RMDQ for back-related disability, and 58.0 (6.9) on the SPADE cluster for HRQOL deficits (Table 1). Low back pain intensity was correlated with both back-related disability (r = 0.46; P < .001) and HRQOL deficits (r = 0.36; P < .001); however, back-related disability was more strongly correlated with HRQOL deficits (r = 0.63; P < .001). Almost identical scores and correlations for the outcome measures were observed in the long-term medical care subgroup. The mean (SD) score on the PSQ-18 for patient satisfaction was 62.6 (28.1) in the overall sample and 65.1 (28.5) in the long-term medical care subgroup.
In the univariable analysis, physician empathy, physician communication, and participant age were directly associated with patient satisfaction, whereas HRQOL deficits and back-related disability were inversely associated with patient satisfaction (Table 2). Similar findings were observed in the multivariable analysis, except that back-related disability was no longer associated with patient satisfaction. Physician empathy was most strongly associated with patient satisfaction in the multivariable analysis (standardized β, 0.638; 95% CI, 0.588-0.688; t = 25.14; P < .001), followed by physician communication (standardized β, 0.182; 95% CI, 0.133-0.232; t = 7.22; P < .001). Multicollinearity was not an issue, with all VIFs being <10 (physician empathy = 2.42; physician communication = 2.40).
Factors Associated With Patient Satisfaction With Medical Care for Chronic Low Back Pain (N = 1,352)
In the long-term medical care subgroup, physician empathy and physician communication were again most strongly associated with patient satisfaction in the univariable analysis, although current physician prescribing of opioids for low back pain was also associated with patient satisfaction (Table 3). Health-related quality-of-life deficits and back-related disability were both inversely associated with patient satisfaction. Again, physician empathy (standardized β, 0.633; 95% CI, 0.529-0.737; t = 11.95; P < .001) and physician communication (standardized β, 0.208; 95% CI, 0.105-0.311; t = 3.96; P < .001) remained most strongly associated with patient satisfaction in the multivariable analysis. Being in a racial minority group was also associated with patient satisfaction in the subgroup (standardized β, 0.095; 95% CI, 0.034-0.155; t = 3.09; P = .002). Multicollinearity was not an issue in the subgroup, with all VIFs being <10 (physician empathy = 3.39; physician communication = 3.33).
Factors Associated With Patient Satisfaction With Medical Care for Chronic Low Back Pain in the Long-Term Medical Care Subgroup (n = 355)
DISCUSSION
Participant perceptions of greater physician empathy and better physician communication skills were both strongly associated with patient satisfaction with medical care for chronic low back pain, including in multivariable analyses that controlled for potential confounders and subgroup analyses that involved long-term medical care. The other process measure pertaining to current physician prescribing of opioids for low back pain was associated with patient satisfaction only in the univariable analysis within the long-term medical care subgroup; however, it did not remain a significant factor after controlling for potential confounders in the multivariable analysis. Health-related quality-of-life deficits were consistently associated with decreased patient satisfaction in all analyses; however, the magnitude of effect was substantially lower than observed for physician empathy and physician communication. Thus, within the structural framework of delivering medical care for chronic low back pain, the process of providing that care via empathic physicians and those with superior communication skills clearly stood out as an important factor associated with patient satisfaction.
Research has identified physician communication as an important aspect of medical care for patients with chronic conditions including low back pain. A therapeutic alliance with the patient via communication and collaboration has been associated with improved pain and physical function outcomes such as those studied here.31 Patients also report greater satisfaction with physicians who provide adequate analgesia, as manifested by decreased pain intensity scores32 or the perception of effective medication.33 Conversely, patients report lower satisfaction with treatment that involves discontinuation of opioids.23 Our findings pertaining to physician empathy are intriguing because they do not necessarily involve a therapeutic alliance with the patient based on collaborative communication or the expectation of a therapeutic effect via pharmacotherapy. A study of 140 attendees of a pain clinic that also used the CARE measure found a correlation between physician empathy and patient satisfaction with their consultation.11 However, the present study extends those findings in 2 important ways. First, physician empathy remained the strongest factor associated with patient satisfaction after adjusting for a series of potential confounders including physician communication. Second, rather than examining the immediate effect of physician empathy during a single consultation, we studied ongoing physician empathy reported by participants including those having a long-term patient-physician relationship. Our findings corroborated the enduring effect of physician empathy on patient satisfaction. Thus, physician empathy might play a key role in the delivery of medical care for chronic pain.34 There is emerging evidence for a neural basis for empathy,35 particularly involving activity in the anterior insula and anterior cingulate cortex.36 Clearly, additional research is warranted in this area.
Strengths of the present study include using participants from a national pain research registry to enhance the generalizability of the findings; collecting data with a digital research platform and electronic data capture that precluded missing data; using a variety of validated research instruments for the patient-physician relationship, clinical outcomes, and patient satisfaction; and conducting multivariable analyses to adjust for potential confounders. However, this study was limited by its cross-sectional design. This precluded definitive assessment of a temporal cause-and-effect relation between process and outcome variables and patient satisfaction. For example, it is possible that prior improvements in pain intensity, physical function, or HRQOL might have prompted participants to report more favorable ratings for physician empathy, physician communication, or patient satisfaction at registry enrollment. Nevertheless, when applying the Bradford Hill guides for assessing causation in the absence of experimental evidence, the strength of association is considered of greater importance than temporality.37 We sought to further mitigate the limitation pertaining to a temporal cause-and-effect relation by conducting the subgroup analyses encompassing long-term medical care. Therein, participants also reported strong associations of physician empathy and physician communication with patient satisfaction.
CONCLUSIONS
Physician empathy and physician communication clearly emerged as the factors most strongly associated with patient satisfaction with medical care for chronic low back pain. These process measures, each representing different aspects of the patient-physician relationship, remained associated with patient satisfaction despite adjustment for participant demographic characteristics and comorbid conditions, current physician prescribing of opioids for low back pain, and outcomes including pain intensity, physical function, and HRQOL. Our findings support the view that patients with chronic pain highly value empathic physicians who validate their concerns and often ill-defined symptoms and physicians who make efforts to clearly communicate treatment plans and expectations.
Footnotes
Conflicts of interest: authors report none.
Read or post commentaries in response to this article.
- Received for publication May 25, 2022.
- Revision received November 9, 2022.
- Accepted for publication November 21, 2022.
- © 2023 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.