
Abstract
PURPOSE Health Teams Advancing Patient Experience: Strengthening Quality (Health TAPESTRY) is a complex primary care program aimed at assisting older adults to stay healthier for longer. This study evaluated the feasibility of implementation across multiple sites, and the reproducibility of the effects found in the previous randomized controlled trial.
METHODS This was a pragmatic, unblinded, 6-month parallel group randomized controlled trial. Participants were randomized (intervention or control) using a computer-generated system. Eligible patients, aged 70 years and older, were rostered to 1 of 6 participating interprofessional primary care practices (urban and rural). In total, 599 (301 intervention, 298 control) patients were recruited from March 2018 through August 2019. Intervention participants received a home visit from volunteers to collect information on physical and mental health, and social context. An interprofessional care team created and implemented a plan of care. The primary outcomes were physical activity and number of hospitalizations.
RESULTS Based on the Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) framework, Health TAPESTRY had widespread reach and adoption. In the intention-to-treat analysis (257 intervention, 255 control), there were no statistically significant between-group differences for hospitalizations (incidence rate ratio = 0.79; 95% CI, 0.48-1.30; P = .35) or total physical activity (mean difference = −0.26; 95% CI, −1.18 to 0.67; P = .58). There were 37 non-study related serious adverse events (19 intervention, 18 control).
CONCLUSIONS We found Health TAPESTRY was successfully implemented for patients in diverse primary care practices; however, implementation did not reproduce the effect on hospitalizations and physical activity found in the initial randomized controlled trial.
INTRODUCTION
As the proportion of older adults increases, health care systems try to meet their complex needs more efficiently and effectively. Strengthening primary care is a system-level strategy to address this. Strong primary care systems report lower hospitalization rates, system costs, and other benefits.1-4 Primary care can improve patient and service use outcomes by managing diseases and advocating for coordinated, longitudinal, person-focused, and comprehensive care.1-3,5-10
Health Teams Advancing Patient Experience: Strengthening Quality (Health TAPESTRY) is a complex primary care–based program focused on improving the health and health care of older adults. Health TAPESTRY aligns with best-practice research and the principles of primary care through the integration of 4 areas: (1) trained volunteers conduct home visits to gather health and social information from patients enrolled in Health TAPESTRY; (2) interprofessional primary health care teams provide health care to patients and work with them to meet their health goals; (3) technology collects and shares information; and (4) community engagement and connections create links between clients and community resources. Our initial randomized controlled trial (RCT) showed positive results in secondary outcomes. At 6 months, people who received Health TAPESTRY walked more (mean difference [MD] = 1.13; 95% CI, 0.31-1.95); had fewer hospitalizations (incidence rate ratio [IRR] = 0.37; 95% CI, 0.18-0.77); and saw their primary care team more (MD = 1.52; 95% CI, 0.84-2.19).11 Our qualitative work suggested mechanisms of Health TAPESTRY, including that the interprofessional care team improved care coordination, gained a better understanding of colleagues’ roles, and developed a sense of which team members to involve in care plans.12 The results informed key strategies for effective implementation, guiding this study.12
In the spread and scale of programs, it is critical to understand factors related to successful implementation, and the reproducibility of effectiveness when implemented and adapted in real-world contexts.13,14 This study aimed to (1) test the feasibility of, and understand the factors contributing to, implementation of the Health TAPESTRY program in 6 primary care practices; (2) test reproducibility of the effect of Health TAPESTRY on hospitalizations and physical activity, compared with usual care found in our initial study; and (3) perform an economic analysis to determine value and costs of implementing Health TAPESTRY.11 The Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework assists in developing, implementing, and evaluating programs; we used this framework for our objectives and outcomes.13 We used Normalization Process Theory (NPT) to further understand the adoption and maintenance of Health TAPESTRY.14
METHODS
Study Design
We conducted a pragmatic 1:1 parallel group randomized controlled trial. The control group received a delayed intervention at 6 months. We simultaneously assessed the implementation and reproducibility of effectiveness in a real-world setting in a Type II hybrid trial.15 Table 1 outlines the differences in implementation between the initial and the current trials. This study was designed to allow for replication of the initial implementation while also allowing implementation to occur as if Health TAPESTRY was being directly translated from research into practice. We recruited 6 primary care sites across Ontario, Canada to achieve the sample size and heterogeneous implementation contexts. Sites were recruited from existing community and primary care contacts and knowledge translation initiatives. At each site, all clinicians, staff, and patients were able to participate. All practices implemented Health TAPESTRY for over 12 months due to rolling recruitment. This study received ethics approval from the Hamilton Integrated Research Ethics Board (#3967). The full trial protocol is published elsewhere.16
Comparison of Interpretation and Implementation of Initial and Current Trials
Participants
Eligible participants were aged 70 years or older and rostered to participating family physicians (patients permanently assigned to a physician practice). Participants were excluded if they resided in a long-term care facility, were unavailable for follow-up, participated in the original Health TAPESTRY implementation, or had other factors that prevented them from completing surveys (eg, severe dementia). The practices identified eligible participants using their preferred methods. All sites were given guidance on suitable patients and questions to consider for recruitment. These included patients with frequent use of the health care system, and those being overlooked or otherwise likely to benefit from an intensive team-based intervention. The patients invited were at the clinic’s discretion. Patients were invited by telephone, mail, or e-mail according to site preference. All participants provided informed written consent. Recruitment occurred from March 15, 2018 through August 31, 2019.
Randomization and Masking
A volunteer coordinator at each site randomly assigned patients into intervention or control groups using a central computerized randomization sequence (block size of 2, 4, and 6 in a ratio of 1:1). Health care team members, volunteers, and researchers were not blinded to randomization.16
Procedures
At each site, Health TAPESTRY was implemented as a collaboration between the primary care practice and a volunteer organization. Two volunteer organizations recruited, trained, and managed all Health TAPESTRY volunteers.17 One was the Canadian Red Cross, a national humanitarian charitable organization, and the other was Windsor-Essex Compassion Care Community, a coalition of community health agencies. During the baseline visit, patients met with 2 volunteers in their home to complete surveys and a goal-setting activity. We mostly used previously validated survey instruments plus a small number of custom questions.16 Volunteers entered responses into a web-based application (TAP-App), using a tablet computer.18 A summary of survey responses (TAP-Report; Supplemental Appendix 1) was securely sent to an interprofessional team of primary care team members (TAP-Huddle) at the patient’s clinic. Personnel at each site received training on possible actions to address information from the TAP-Reports.
Each TAP-Huddle was required to have at least 3 different health care team members linked to the clinic; however, the type of professionals involved was the clinic’s choice (Supplemental Table 2) and volunteer coordinators could attend TAP-Huddles.
The TAP-Huddle created and implemented a plan of care for each patient. The TAP-Huddle involved the volunteers at a follow-up visit at the patient’s home after 6 months to complete the surveys again. Volunteers had a list of community resources that they could share with patients and they could assist patients in joining community programs (Supplemental Appendix 2).
The control group received an initial visit by volunteers, who administered the same surveys as the intervention group, however, no report was created and the TAP-Huddle did not discuss the patients. The patients received usual care until the 6-month data collection, after which they were offered the intervention.
Outcomes
We collected data using structured surveys, electronic medical records, and program records. All data were stored at the lead implementation site. The study outcomes were developed to map on to the RE-AIM framework.13
Reach
Reach examines the extent to which the program reaches the target population, specifically the proportion of eligible people who start the program, the representativeness of the sample compared with the Canadian population, and the frequency of volunteer visits.
Effectiveness
Effectiveness looks at the impact of an intervention on outcomes. Co-primary outcomes to assess reproducibility of the initial RCT results8 were total metabolic equivalent of task (MET) minutes of physical activity per week19 and number of hospitalizations. Secondary effectiveness outcomes were hours sitting per day, minutes walking,19 moderate-vigorous physical activity,19 patient enablement,10 quality of life,20 treatment burden,21 disease burden,22 and the number of emergency or urgent care visits, falls, medications, and primary care visits.
Adverse events included serious adverse events using accepted definitions, assessment of the extent to which expectations were not met (disappointment), and labeling effects (labeling health conditions as a result of Health TAPESTRY screening). Baseline health care utilization was defined as the 6 months before patient’s study start date.
Adoption
Adoption evaluates the proportion and representativeness of primary care sites that participated, proportion of recruiting health care clinicians, number of volunteers involved, and adoption processes using the Normalization Measurement Development (NoMAD) instrument.14 Any primary care staff member involved with Health TAPESTRY was invited to complete the NoMAD 6 times over 12 months. We scored the NoMAD using the NPT domain subscales: coherence, collective action, cognitive participation, and reflexive monitoring.
Implementation
Implementation measures included the number of TAP-Reports, clinical actions, each primary care practices’ fidelity to the program (Supplemental Table 3), and high-level barriers and facilitators to implementation. The barriers and facilitators are based on feedback from stakeholders (patients, volunteers, volunteer coordinators, clinicians, and clinical managers) in interviews/focus groups and an open-ended survey (described in the protocol).16
Maintenance
Assessment of maintenance of the intervention was based on the 12-month score on the NoMAD item “Do you feel Health TAPESTRY is part of your normal part of work?” (10-point scale: 1 = not at all to 10 = completely) averaged per site,14 the proportion of patients and health care team members who recommend the program, and sites continuing with Health TAPESTRY.
Sample Size
To determine differences in the co-primary outcomes at 6 months between groups, we aimed to recruit 584 participants. This sample size was based on the effect size of the co-primary outcomes of the initial trial,11 while assuming a power of 0.80, type I error probability of 0.05, and attrition rate of 20% (see protocol for details).16
Data Analysis
Baseline characteristics are reported by group using mean (SD), median (first quartile, third quartile), or count and proportion (number, percentage) depending on variable type. We took an intention-to-treat approach to the effectiveness outcomes at 6 months, using multiple imputation through chained equations to impute missing data.23 All randomized individuals were included in the intention-to-treat analysis even if they did not receive follow-up. We analyzed the continuous outcomes, including the co-primary outcome physical activity, using multiple linear regression. We report the pooled effect estimate in terms of mean difference along with 95% CIs. We analyzed the count outcomes, including the co-primary outcome number of hospitalizations, using negative binomial regression. The pooled effect estimates in terms of incidence rate ratio along with 95% CIs are reported. The criterion for statistical significance was set a priori at α = 0.05.
All analyses were adjusted for the site and baseline values when determining effectiveness. Sensitivity analyses were conducted through per-protocol approach for primary and secondary outcomes. In addition, post-hoc logistic regressions adjusting for site and baseline values were conducted to evaluate the association of Health TAPESTRY with: (1) any hospitalizations; (2) any hospitalization or emergency department visits; (3) the proportion of patients achieving at least 20% increase in MET minutes; and (4) the proportion of patients achieving any increase in MET minutes from baseline to 6 months. To identify factors that might impact on our primary outcomes, we included age, sex, and the Charlson Comorbidity Index as additional covariates in our analysis of hospitalizations and MET minutes. All other outcomes are reported descriptively. Analyses were performed using R version 4.0.3 (R Foundation for Statistical Computing). Qualitative data analysis is described elsewhere.16
Economic Evaluation
A 6-month trial-based economic evaluation was conducted from a public payer perspective to compare Health TAPESTRY and usual care in terms of costs and quality-adjusted life years. The detailed methods for this economic evaluation have been described in the study protocol.16 Briefly, 6-month health care resource utilization consumed in each group were costed using public data sources (Supplemental Table 4 for a list of unit costs), while costs related to the implementation of Health TAPESTRY (ie, personnel, office supplies and equipment, tablets, and volunteer onboarding) were determined using trial data.
Quality-adjusted life years were calculated based on baseline and 6-month EQ-5D-5L (EuroQol Group) utility measurements using an area under the curve approach. EQ-5D-5L addresses mobility, self-care, usual activities, pain or discomfort, and anxiety or depression. Bootstrap techniques24 were used to deal with sampling uncertainty and the uncertainty was presented using cost-effectiveness acceptability curves.25
RESULTS
Reach
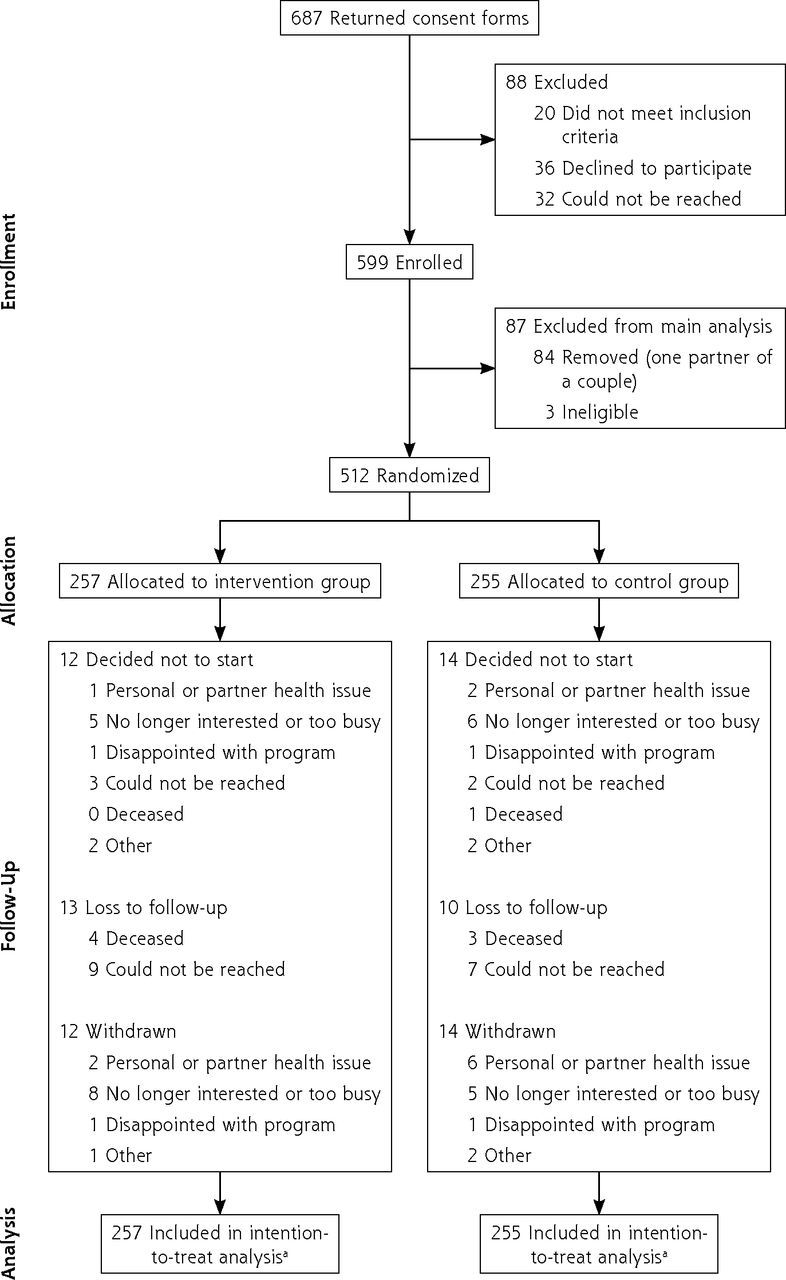
Approximately 3,711 potential participants were invited by mail (Figure 1), 687 (19%) returned a signed consent form, and 599 were enrolled (16%). Recruitment strategies varied across sites, as did enrollment (range across sites was 10% to 57%). One partner per couple was removed; therefore 512 people were randomized (257 intervention, 255 control).
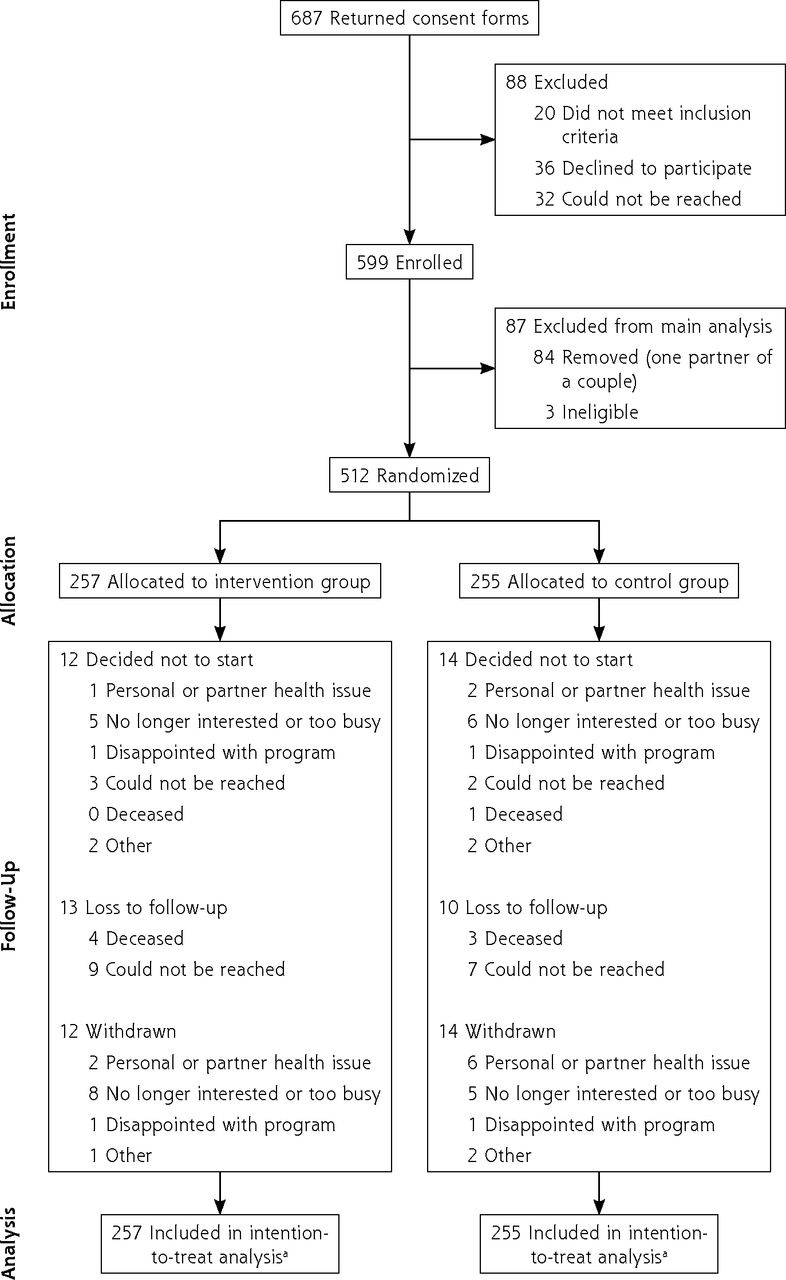
CONSORT flow diagram of participants.
CONSORT = consolidated standards of reporting trials.
a All randomized individuals were included in the intention-to-treat analysis even if they did not receive follow-up.
The intervention and control groups were similar (Table 2) and while comparable to the Canadian population for socioeconomic status,26 Black, Indigenous, and other people of color were under represented. The most frequent key information that appeared on the TAP-Report for the intervention group related to limitations of walking and stair climbing, nutrition, and interest in discussing advance care planning (Supplemental Table 1).
Baseline Characteristics of Participants by Group
Volunteers conducted 283 initial study visits and 57 follow-up visits with the intervention group, mainly as requests to facilitate connections to community programs (42% of visits).
Effectiveness
There was no statistically significant difference between groups for the co-primary outcomes. Among the secondary outcomes (Table 3), the intervention group had significantly more primary care visits (including interprofessional team members) than the control group at 6 months (mean = 4.51 vs 3.63, P <.005, IRR = 1.18; 95% CI, 1.01-1.37). The removal of outliers in physical activity outcomes did not impact the results (eg, moderate-vigorous physical activity with outliers removed MD = −0.14; 95% CI, −0.68 to 0.41). Both intervention and control participants reported a decrease in physical activity (all domains) at 6 months compared with baseline; however, the median minutes of activity were not considered suboptimal (ie, less than 150 minutes/week). The decrease was less in the intervention group but difference was not significant.
Patient-Reported and Health Care Utilization Outcomes Related to Effectiveness
Most participants indicated Health TAPESTRY met or exceeded their expectations, and only a small portion of participants became aware of health issues otherwise unknown to them (Supplemental Table 5). None of the serious adverse events were adjudicated to be linked to the intervention; no patterns were observed (Supplemental Table 5).
Sensitivity Analyses
We conducted several post-hoc sensitivity analyses to better understand the findings within the implementation lens. Neither our per-protocol analysis of the primary and secondary outcomes or our post-hoc analyses using logistic regressions changed the findings. While age and sex were not significant predictors of hospitalization or MET minutes, the Charlson Comorbidity Index score was found to be a significant predictor of hospitalizations (IRR = 1.21; P = .01). We examined the data for the co-primary outcomes at the lead implementation site (same as the site for the original RCT) and enrolled almost 40% of the study participants. While the effect on hospitalizations, emergency visits, and quality of life favored the intervention group (Table 4), it was not statistically significant. The trial was not powered to detect differences at individual sites and there was no suggestion of an effect at other sites.
Sensitivity Analysis (Efficacy): Co-Primary Outcomes at the Lead Implementation Site
Adoption
Six of 11 Family Health Teams (FHTs) approached about the study participated (55% adoption) (Supplemental Appendix 3). The FHTs differed in many aspects including number of sites, interprofessional health care team members, and in-clinic programs (Table 5, Supplemental Table 2).
Descriptions of the 6 Participating FHTs and Key Outcomes Across Ontario
In total, 61 physicians (of initial 100 eligible) had at least 1 patient participate. There were 4 to 37 physicians per FHT, a 61% adoption rate. The size and composition of TAP-Huddles (3-8 team members) differed between sites (Supplemental Table 2). Physicians, occupational therapists, nurses, social workers, and dietitians commonly participated in TAP-Huddles.
Overall, 301 people were recruited to be Health TAPESTRY volunteers (aged 18-78 years). Through 49 training sessions, 217 volunteers were trained and became active; 68 volunteers withdrew or were lost to follow-up. A fuller description of the volunteers is available elsewhere.27
In total, 56 people from all sites (6 physicians, 40 health care team members, 10 other) completed the NoMAD at least once. The average scores for 3 of the 4 subscales (Coherence, Collective Action, and Reflexive Monitoring) improved over time (Supplemental Table 6). The average score for Cognitive Participation remained the same; however, the scores for this subscale were consistently higher than the other subscales.
Implementation
All FHTs achieved high fidelity to the protocol with scores of 29-31 (maximum = 33). One major adaptation occurred partway through the program due to volunteer recruitment challenges: sites could send a volunteer coordinator (a paid position) with a volunteer or allow only 1 person (volunteer or coordinator) to complete a study visit, instead of sending 2 volunteers.
The intervention group had follow-up contact by health care team members through telephone calls (22%) or clinic visits and assessments (20%). Of all contacts, 29% included a recommendation to the patient (eg, clinic-based program). Other than the TAP-Huddle who created a plan of care, follow-up was completed most often by a registered nurse (22%), occupational therapist (9%), or physician (9%) (Supplemental Table 7).
From our qualitative data, key barriers to implementation included: a struggle to recruit patients who in clinicians’ opinions would most benefit from the intervention, volunteers and patients finding surveys repetitive or confusing, technology glitches, specific gaps in volunteer training or knowledge (eg, community resources), and patients not understanding the program or its purpose. Key facilitators included: the opportunity to have time set aside to take a collaborative approach during TAP-Huddles, volunteers being able to work with a partner on visits, volunteers feeling well-trained overall (despite some specific gaps), having the volunteer coordinator at TAP-Huddles, and the use of patient recruitment strategies such as patient-facing materials that clearly explain the program.
Maintenance
After 12 months of implementation, the scores from the NoMAD indicated that Health TAPESTRY was well normalized for the FHT members (Supplemental Table 6). However, when participants were explicitly asked about how “normal” Health TAPESTRY feels, 4 of the TAP-Huddles agreed that it was a normal part of their work, whereas 3 TAP-Huddles were unsure.
Of the health care team members surveyed (n = 60), 53% indicated they would recommend Health TAPESTRY to others and 32% were unsure. Of the 23 patients who provided responses, 100% indicated they would recommend the program. Most patients who were asked the question did not respond. When the FHT leadership were asked if they wanted to continue with Health TAPESTRY, 5 of the 6 FHTs indicated yes with the assumption of continued support from the volunteer organizations, as the FHTs would not be able to manage volunteer coordination.
Economic Evaluation
With an intervention cost of $562 per patient (Supplemental Table 8), Health TAPESTRY compared with the control group resulted in $380 of additional costs and generated 0.0025 more quality-adjusted life years, yielding an incremental cost per quality-adjusted life years gained of $152,558. Supplemental Table 9 and Supplemental Figure 1 present the cost-effectiveness results and acceptability curve.
DISCUSSION
Health TAPESTRY was successfully implemented, with high fidelity to the model, for all patients across 6 heterogenous family practice settings in Ontario, Canada. There was a high level of normalization of Health TAPESTRY into routine workflow at 1 year. The flexibility in implementation to fit local context (eg, recruitment, TAP-Huddle make-up) contributed to this. However, the effect on hospitalizations and physical activity compared with usual care was not reproduced, and we found no significant between-group differences at 6 months for the co-primary or secondary outcomes. Compared with the control group, Health TAPESTRY resulted in an incremental cost per quality-adjusted life years gained of approximately $153,000.
In assessing implementation across the key pillars that primary care uses to improve health outcomes for the population (access, comprehensiveness, integration, person focus),1,2 we found beneficial effects. In both the original and current trial, we found evidence of greater access to comprehensive primary care, with significantly more primary care visits in the intervention group over 6 months, and better comprehensiveness: the visits triggered involvement of a broad range of health care team members.11 In other research on the same implementation, we found that team members expanded their understanding of system navigation,28 potentially impacting integration.
We speculate there are several reasons for the lack of reproducibility and outline a few here. We took a pragmatic approach to implementation to reflect what happens in the real world: a randomized trial occurs in a tightly controlled way, then if successful, is implemented flexibly according to local context, and it is assumed that RCT effectiveness is reproduced. The original study was at 1 academic FHT,11 whereas the current implementation occurred at 6 FHTs.11 In this implementation, at the same site as the original RCT only, post hoc analysis suggested that the effect on hospitalizations, emergency visits, and quality of life again favored the intervention group, but this did not translate broadly. Despite high fidelity, local contextual differences such as health care team characteristics, clinic workflow, and levels of vertical health care system integration likely drove the varying effectiveness of Health TAPESTRY. Further, the context-specific flexibility illustrates a common phenomenon of dilution of effect when research results are translated into practice.29 This does not invalidate the initial results, but illustrates the pragmatic tension between proving efficacy in a controlled context, and achieving scale-up as part of routine care, which maps onto the fundamental intention; to help people in the real world. Further exploration of site differences is elsewhere.30 This raises questions for future work about the key elements of successful implementation and scale up of a complex intervention that has initial efficacy data, but a primary care context that requires flexible implementation.
The patient populations in each study differed and this may have influenced results. For example, the proportion of patients with diabetes and with suboptimal physical activity were both less than that in the original trial population, which may have limited the size of the group to whom further actions were recommended and potential for impact on patient outcomes. Further, though the program was able to be successfully implemented and integrated into routine primary care workflow in the clinics for all patients, the proportion of patients who responded to the invitation was 19%. This finding highlights another point of tension in implementation trials. Recruiting to randomized trials in primary care is notoriously difficult with many failing to reach their recruitment targets. While our recruitment rate compares favorably to recruitment rates in primary care RCTs and the target was met, the research framework makes it impossible to assess true reach.31,32 We know patients may not want to engage in randomized trials in primary care because of the burden of research assessments or randomization. There is no way to estimate whether this reach would improve if implementation was outside a research framework without an observational study. The 19% response rate would represent suboptimal reach if it did not improve response to invitation outside a research framework. This is an area to explore in future primary care research and is an important consideration for implementation trials.
Our mixed results pose other questions around the practicality and utility of trials reproducing efficacy of any intervention in a wider pragmatic implementation trial within the primary care landscape, particularly those outcomes with complex causation such as hospitalizations or health behaviors. How should these different elements of program implementation be balanced? On one hand, there is an essential requirement for ongoing evaluation when implementing research into practice, especially in the heterogenous context of primary care, to ensure health care resources and effort are used most effectively. On the other, if the efficacy of an intervention is established in a controlled context with specific outcomes chosen because they are amenable to measurement, the value in understanding how to implement an intervention in primary care may be more rooted in the effects of the underpinning processes (eg, interprofessional teamwork and collaboration) that strengthen the core dimensions by which primary care achieves better population outcomes.
This study has several strengths. Basing our evaluation in the RE-AIM framework and NPT provided critical information (beyond effectiveness) that specifically assessed implementation to shape the scale and spread of Health TAPESTRY. The trial of implementation across several settings was a key strength, testing the ability to successfully scale up into routine care. Regarding limitations, like the population in the first trial, the participants were arguably healthier than the source population, which could mean that our study did not recruit the population that would have most benefited from or been interested in Health TAPESTRY. Future trials could consider recruiting from more defined patient populations such as those new to a practice, from groups more likely to experience health inequity, or recently discharged from the hospital. Further, different study designs would give a better assessment of the concept of reach. A larger sample size or longer follow-up period may have detected significant effects which future trials could investigate. Regarding outcomes given by team members (eg, NoMAD) and patients, there was a chance of response bias. Lastly, since our outcomes were guided by the aim to reproduce the results of the first implementation, this study likely missed outcomes related to other mechanisms by which Health TAPESTRY improved patient outcomes. For example, incorporating outcomes relating to the delivery of care such as the Patient Assessment of Chronic Illness Care could be beneficial33 for future trials.
CONCLUSIONS
Our findings show the critical importance of pragmatic trials of implementation with less-controlled conditions. While our findings show that for patients, successful implementation and normalization into routine clinical workflow of a complex intervention such as Health TAPESTRY is feasible across varied primary care settings, we did not reproduce the effectiveness of the original implementation. This reinforces the importance of assessing implementation into routine practice, as well as raising questions about approaches and limitations to this kind of research in primary care settings, such as estimating true reach in a design that, while necessarily robust for research outcomes, is at the same time a disincentive to patient engagement. This program helped foster greater patient access to comprehensive primary care, so understanding how Health TAPESTRY and similar programs could impact people who access primary care less often, who are less healthy, or are not connected with primary care warrants future work. See Supplemental Appendix 4 for other articles related to this RCT and outcomes.
Acknowledgments
The authors thank the health care team members and staff from the 6 Health TAPESTRY implementation sites for their hard work and commitment to Health TAPESTRY: Dufferin Area Family Health Team, Harrow Health Centre, McMaster Family Health Team, Niagara North Family Health Team, Superior Family Health Team, and Windsor Family Health Team. Yana Almeida, Lisa Banning, Tanya Elliott, Alexander Macmillan, Marianne Skerl, and Chantel Sylvain from the Canadian Red Cross; Deborah Sattler from Windsor Essex Compassion Care Community; the volunteer coordinators Mackenzie Berthiaume, Cherie Gagnon, Jaclyn McKenna, Danielle Mischkot, Nelson Ruiz-Blanco, Louisa van Lith, and Samantha Woodcroft; and staff at McMaster University: Stephanie Di Pelino, Steven Dragos, Jay Gallagher, Jennifer Lawson, Lynda Nash, and Fiona Parascandalo. The authors would also like to thank all the volunteers for their exceptional work delivering the program.
Footnotes
Conflicts of interest: authors report none.
Read or post commentaries in response to this article.
Funding support: This work was supported by the Ontario Ministry of Health and Long-Term Care and by David Braley. The funders of this study had no role in the design; data collection, analysis, or interpretation; or writing of the report. Authors had full access to the data in the study and the corresponding author had the final responsibility for the decision to submit this manuscript for publication.
Trial registration: The trial (NCT03397836) is registered as complete at https://clinicaltrials.gov/ct2/show/NCT03397836
Supplemental materials
- Received for publication February 22, 2022.
- Revision received November 11, 2022.
- Accepted for publication November 21, 2022.
- © 2023 Annals of Family Medicine, Inc.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.