
Abstract
Few have studied the COVID-19 pandemic’s impact on tobacco use status assessment and cessation counseling. Electronic health record data from 217 primary care clinics were examined from January 1, 2019 to July 31, 2021. Data included telehealth and in-person visits for 759,138 adult patients (aged ≥18 years). Monthly rates of tobacco assessment per 1,000 patients were calculated. From March 2020 to May 2020, tobacco assessment monthly rates declined by 50% and increased from June 2020 to May 2021 but remained 33.5% lower than pre-pandemic levels. Rates of tobacco cessation assistance changed less, but remain low. These findings are significant given the relevance of tobacco use to increased severity of COVID-19.
INTRODUCTION
The COVID-19 pandemic dramatically altered patterns of primary health care–seeking and delivery. This was reflected in a dramatic increase in telehealth visits (ie, video and telephone visits)1,2 and a shift from comprehensive to acute care and immunization efforts. Many patients delayed seeking care for routine prevention and disease management due to limited in-person appointments and fear of traveling to/attending in-person visits. Since the start of the pandemic, several studies have shown a decline in receipt of preventive care3-6 and chronic disease management.7 Little is known about the impact of the pandemic on addressing tobacco use. Given the relevance of tobacco use for severe symptoms of COVID-19,8,9 it is important to understand the pandemic’s impact on tobacco assessment and cessation assistance.
Use of tobacco remains the leading cause of preventable morbidity and mortality in the United States10 and disproportionately affects socioeconomically disadvantaged persons.11,12 Thus, reducing the harms from tobacco use is particularly important in the context of community health centers (CHCs) which provide primary care services for a large proportion of socioeconomically disadvantaged patients. The purpose of this study is to describe the COVID-19 pandemic’s impact on the assessment of and cessation assistance for tobacco use among patients receiving care at CHCs.
METHODS
Electronic health record (EHR) data from CHCs from the OCHIN Network were extracted from January 1, 2019 to July 31, 2021. OCHIN, Inc is a nonprofit health technology network that provides a single instance of Epic to its member CHCs, which vary in size, location, staff roles, clinical workflows, and patient populations. OCHIN patients are socioeconomically vulnerable (>70% from households <200% of the federal poverty level). Eligible clinics were primary care or public health departments that provided patient care during the study period. A total of 217 clinics within 79 health centers across 13 states, representing 7,225,354 encounters by 759,138 patients, had useable tobacco-related data during the study period. Tobacco assessment and counseling were documented in the EHR with checkboxes indicating complete/not complete. Data were collected from telehealth and in-person primary care visits for adult patients (aged ≥18 years). Patients were included if they had ≥1 preventive care visit or ≥2 office or telehealth visits with a clinician between February 1, 2018 to June 30, 2021. Monthly rates of tobacco assessment per 1,000 patients were calculated. Rates of provision of tobacco cessation counseling and cessation medications (nicotine replacement therapy, bupropion, and varenicline) per 1,000 patients that use tobacco were calculated. Telehealth visits were health care visits conducted by telephone or video. Rates of these indicators are reported by month for the study period and graphically displayed. The Oregon Health & Science University (OHSU) Institutional Review Board approved this study.
RESULTS
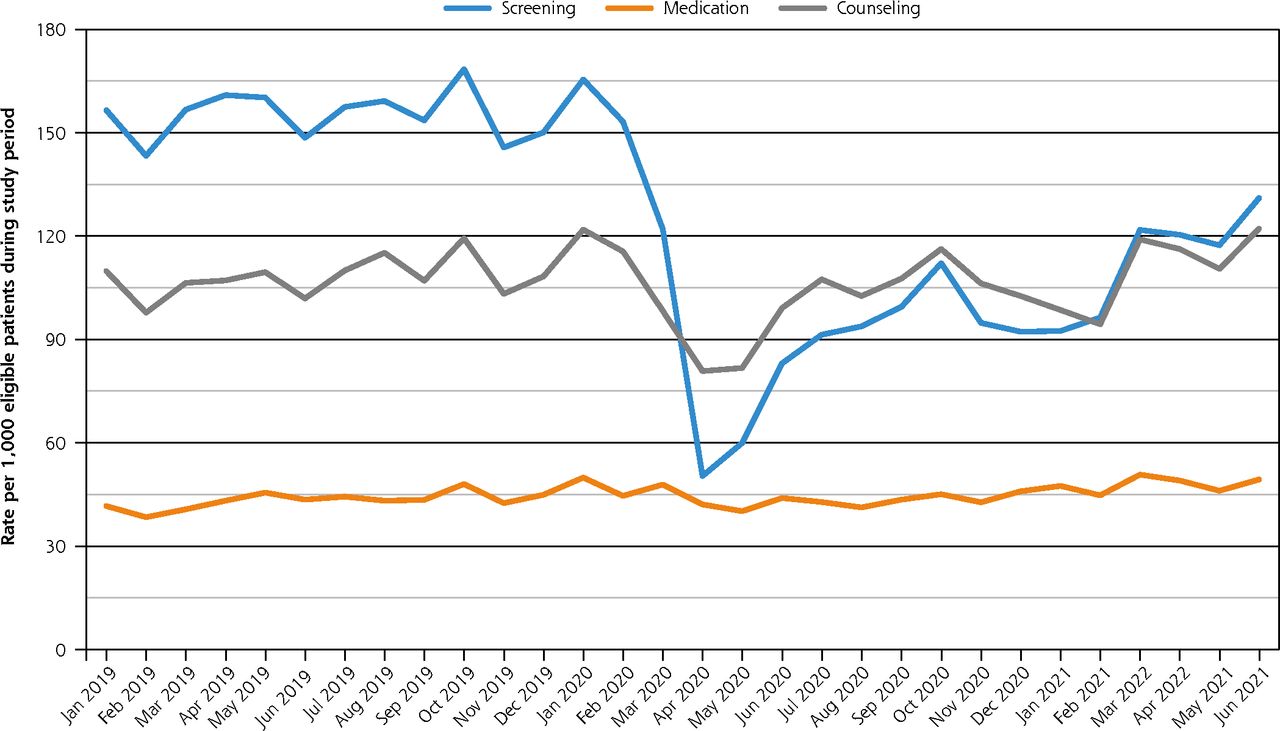
Figure 1 shows that from January 2019 to February 2020, monthly rates of tobacco assessment per 1,000 patients was 155.7. From March 2020 to May 2020, rates of tobacco assessment declined to 77.7 per 1,000 patients, a 50% reduction. From June 2020 to May 2021, rates of tobacco assessment increased but remained 33.5% lower than pre-pandemic levels.
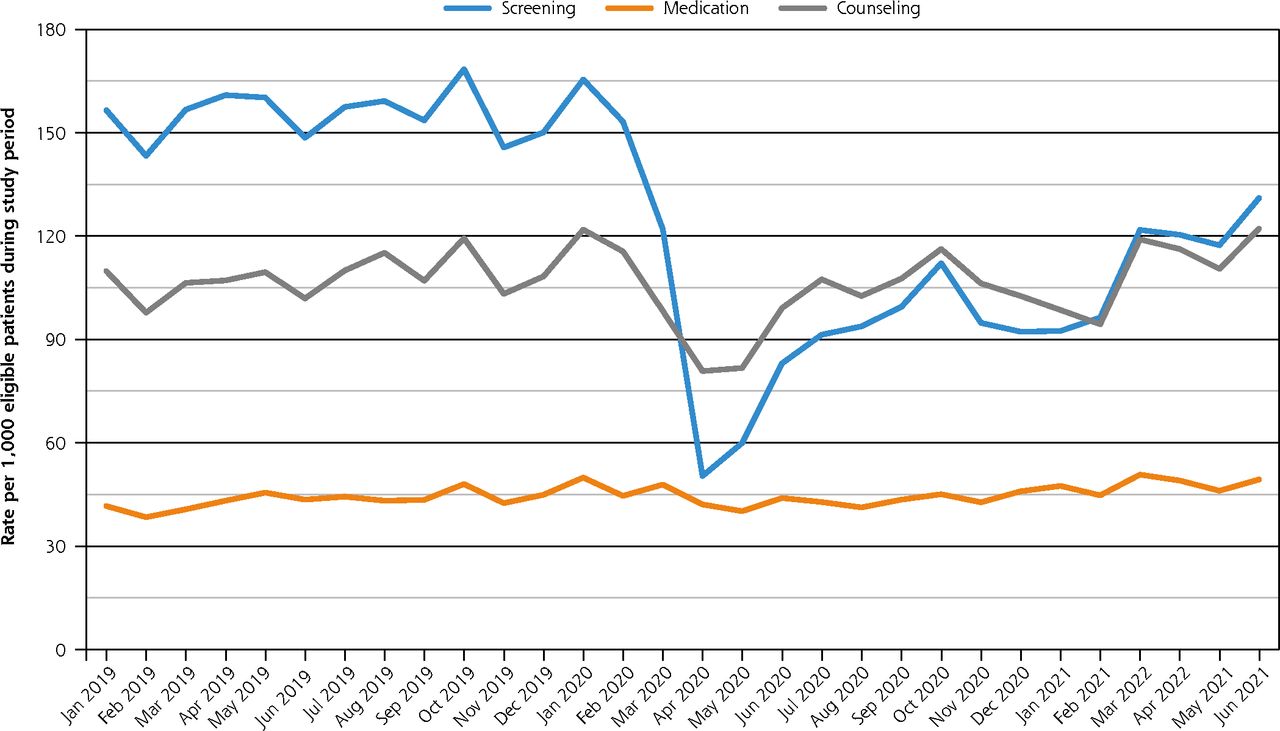
Tobacco screening, counseling, and provision of tobacco cessation medications.
Provision of tobacco cessation counseling decreased from 109.5 from January 2019 to February 2020, to 87.1 per 1,000 tobacco users from March 2020 to May 2020, a 20.4% decline. From June 2020 to May 2021, rates of tobacco cessation counseling increased to 107.9 (2.5% lower than prepandemic levels). Provision of tobacco cessation medications was low, 43.9 per 1,000 tobacco users from January 2019 to February 2020, and declined slightly across the time periods.
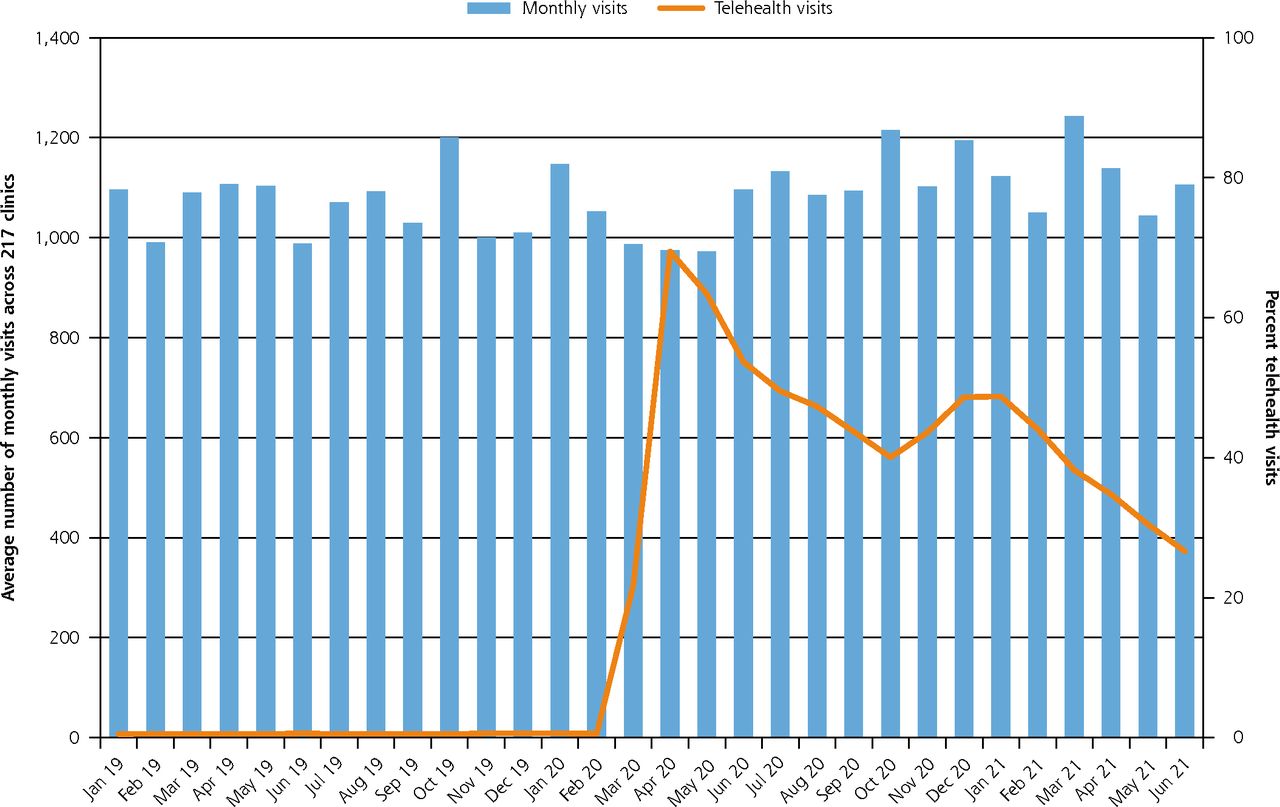
Among the 217 clinics, the average monthly number of adult patients seen was 830. Figure 2 shows that the average monthly visit across clinics remained fairly steady; however, telehealth visits increased from a monthly average of 4.6 visits before the onset of the pandemic to 436.0 average monthly visits. The proportion of visits conducted as a telehealth visit peaked at 69.5% in April 2020 and declined gradually to 27% in June 2021.

Number of visits by month and percent of telehealth visits.
DISCUSSION
The decline in rate of tobacco assessment during the first wave of the COVID-19 pandemic was substantial and rates did not return to prepandemic levels. These findings are significant given the relevance of smoking to increased severity of COVID-19 and the emerging evidence that tobacco cessation13 and abstinence rates have declined during this pandemic period.14 Further, the observed pattern of tobacco care delivery in CHCs is different from screening for colon, cervical, and breast cancer—which declined at the beginning of the pandemic but rebounded to prepandemic levels.4,5 Unlike other cancer screenings, tobacco assessment and cessation assistance do not require face-to-face interaction with health providers and can be conducted during telehealth visits. So why did tobacco assessment and assistance drop and not rebound to prepandemic levels?
It is possible that routines for tobacco assessment were disrupted with the change to telehealth and never reestablished as clinics shifted back to office visits. Tobacco assessment before the pandemic was likely conducted by medical assistants during the rooming process involving vital signs and tobacco use history.15 It is likely that telehealth visits changed this workflow such that gathering vital signs—typically done by the person who “roomed the patient”—was omitted as a step before initiating the interaction between the patient and clinician. Use of telehealth to collect information about tobacco history and provide tobacco treatment can be effective16,17; however, lack of standard workflow on when and who should assess tobacco history during telehealth visits in CHCs could have impeded tobacco assessment performance. Tobacco cessation assistance (counseling and medications) substantially outperforms other preventive services like cervical and breast cancer screening and provision of statins in the number needed to treat to prevent 1 death.18,19 Given the health impact of tobacco use, all primary care settings should have a process in place to routinely assess tobacco status and to provide assistance for quitting. Careful examination of procedural changes that promote or impede assessment of tobacco, including adaptation to support tobacco assessment via telehealth, is needed to guide resilient procedures that can weather operational changes.
Limitations
The data for this study are aggregate rates and cannot examine rates of tobacco assessment and assistance by telehealth visits vs office visits. Understanding this association is important to uncover operational issues to tobacco cessation support that could be addressed. Further, we cannot examine patient level characteristics to evaluate if the decline in tobacco cessation support affected some subgroups more than others. Finally, these data are from CHCs in 13 states and may not be generalizable to other settings.
CONCLUSIONS
The decline in rate of tobacco assessment during the onset of the COVID-19 pandemic was substantial and rates have not returned to pre-pandemic levels. Careful examination of procedural changes to adapt to various media of care delivery is needed to support CHCs preventive care delivery efforts and their patients.
Acknowledgments
This work was conducted with the Accelerating Data Value Across a National Community Health CenterNetwork (ADVANCE) Clinical Research Network (CRN). ADVANCE is led by OCHIN in partnership with Health Choice Network, Fenway Health, Oregon Health & Science University, and the Robert Graham Center HealthLandscape. ADVANCE is funded through the Patient-Centered Outcomes Research Institute (PCORI), contract number RI-OCHIN-01-MC.
Footnotes
Conflicts of interest: authors report none.
Read or post commentaries in response to this article.
Funding support: This work was supported by the National Cancer Institute (NCI) of the National Institutes of Health (grant number P50CA244289). This P50 program was launched by NCI as part of the Cancer Moonshot. The funding source had no role in design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
- Received for publication July 26, 2022.
- Revision received October 20, 2022.
- Accepted for publication November 2, 2022.
- © 2023 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.