
Abstract
PURPOSE Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) are the 2 most frequently reported notifiable sexually transmitted infections (STIs) in the United States, and Trichomonas vaginalis (TV), although not a notifiable disease, is the most common curable non-viral STI worldwide. Women bear a disproportionate burden of these infections and testing is necessary to identify infections. Although vaginal swabs are the recommended sample type, the specimen most often used among women is urine. The objective of this meta-analysis was to assess the diagnostic sensitivity of commercially available assays for vaginal swabs vs urine specimens from women.
METHODS A systematic search of multiple databases from 1995 through 2021 identified studies that (1) evaluated commercially available assays, (2) presented data for women, (3) included data obtained from the same assay on both a urine specimen and a vaginal swab from the same patient, (4) used a reference standard, and (5) were published in English. We calculated pooled estimates for sensitivity and the corresponding 95% CIs for each pathogen as well as odds ratios for any difference in performance.
RESULTS We identified 28 eligible articles with 30 comparisons for CT, 16 comparisons for NG, and 9 comparisons for TV. Pooled sensitivity estimates for vaginal swabs and urine, respectively, were 94.1% and 86.9% for CT, 96.5% and 90.7% for NG, and 98.0% and 95.1% for TV (all P values <.001).
CONCLUSIONS Evidence from this analysis supports the Centers for Disease Control and Prevention’s recommendation that vaginal swabs are the optimal sample type for women being tested for chlamydia, gonorrhea, and/or trichomoniasis.
INTRODUCTION
Effective screening for sexually transmitted infections (STIs) and adherence to recommended laboratory testing practices is essential to STI surveillance, control, and prevention. Endocervical, vaginal, and urine specimens from women have been cleared by the United States Food and Drug Administration as genital sample types for use with most nucleic acid amplification tests (NAATs) for Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG), and Trichomonas vaginalis (TV). Since 2009, the Centers for Disease Control and Prevention (CDC) has recommended use of vaginal swabs as ideal.1 Current laboratory-based screening of women for CT, NG, and TV, however, often relies on urine specimens.2,3 Of even greater concern is the common practice of using remnant, clean-catch urine left after pregnancy testing, urinalysis, or other on-site testing. This sample type is less sensitive than first-catch urine,4,5 which is specified in intended use statements for every NAAT with a urine claim. All clinical studies that develop sensitivity estimates used in assay package inserts are based on use of first-catch urine since that is where the target material is most likely present. These infections are not typically located in the female urethra, so urine is only useful for diagnostics only if cervical or vaginal material has dripped into the urine, which occurs at the onset of micturition. The cleansing prior to a clean-catch urine sample reduces the possibility of capturing this material. Among samples from women, the organism load is highest in cervical swabs, less in vaginal swabs, and lowest in urine specimens.6-8 While the CDC recommendations suggest that first-catch urine is acceptable for women, it may detect up to 10% fewer infections compared with vaginal swabs.7,9,10
Systematic reviews related to this topic have focused on the comparing the performance of assays for both genital and extragenital sample types for men and women, but there is a lack of reviews specifically examining diagnostic sensitivity head-to-head for the noninvasive genital sample collection of urine compared with vaginal swabs among women. Therefore, the objective of this meta-analysis is to provide a synthesis of the evidence on the diagnostic assay sensitivity for female vaginal swabs vs urine samples among commercial assays for CT, NG, and TV. The results from our analyses may have the potential to advance screening and detection of CT, NG, and TV leading to subsequent enhancement of women’s quality of care and improvements in pregnancy and reproductive outcomes.
METHODS
Search Strategy
We based our review strategy on published frameworks, including the PRISMA and QUORUM guidelines for systematic reviews and meta-analysis of diagnostic tests and reporting.11-13 We also used the software tool, Covidence (Veritas Health Innovation),14 to assist in screening and data management. We searched PubMed, EBSCO, Cochrane Central Register of Controlled Trials (CENTRAL), and Scopus for articles published from January 1, 1995 through December 31, 2021. We specifically sought articles that contained the terms women, vaginal swab, urine, and chlamydia or gonorrhea or trichomoniasis in abstracts, titles, and key words. In addition, we evaluated whether the title, abstract, key words, or text included the terms nucleic acid amplification test, polymerase chain reaction, strand displacement, transcription-mediated, ligase-chain reaction, or diagnostic assay. Additional articles were identified through references of relevant articles and a hand search through 4 journals in which articles on these topics most commonly appear (Journal of Clinical Microbiology, Sexually Transmitted Diseases, Sexually Transmitted Infections, and Journal of Infectious Diseases).
Eligibility Criteria
We included studies that (1) evaluated commercially available NAATs for CT, NG, and TV since these assays have the strongest available performance data; (2) presented data for adolescent and/or adult women (pediatric use was excluded); (3) included sensitivity data obtained from the same assay on both a urine specimen and a vaginal swab; (4) used a reference standard other than the test being evaluated; and (5) were published in English. We created criteria for a reference quality standard to minimize sensitivity estimate bias. These criteria required that studies estimated sensitivity compared with at least 1 alternate target NAAT, or to culture, or other methods accepted as standards at the time (wet mount microscopy, ELISA, direct fluorescent antibody assays, laboratory developed tests).
Data Extraction
The titles and abstracts of studies identified by the search were screened by all authors and studies that did not meet eligibility criteria were removed. Abstracts had to describe a population of sexually active adolescent or adult women and a relevant commercially based assay for CT, NG, or TV to be considered further. The full-text reports of all potentially relevant studies were obtained and assessed independently for eligibility, based on the defined inclusion criteria, by K.J.A., S.G., A.F., and B.VDP. Standardized data extraction forms were used; data were extracted by a single reviewer (K.J.A.) and checked by a second reviewer (S.G., A.F., or B.VDP.). Any disagreement was resolved by discussion.
Data Analysis
We calculated sensitivity estimates and corresponding 95% CIs, as well as odds ratios (ORs) of any differences, and generated forest plots with R software (R Foundation for Statistical Computing) using the meta package.15 We used fixed-effects models to compare the difference between the 2 specimen types for CT and NG because in both cases the heterogeneity measure, I2, was less than 50%, and because we believe the difference between performance of urine and vaginal swabs represents a global observation across studies. For TV, however, we used the random effects model as I2, which was 66%, indicating moderate to high heterogeneity.16
RESULTS
Publication Characteristics
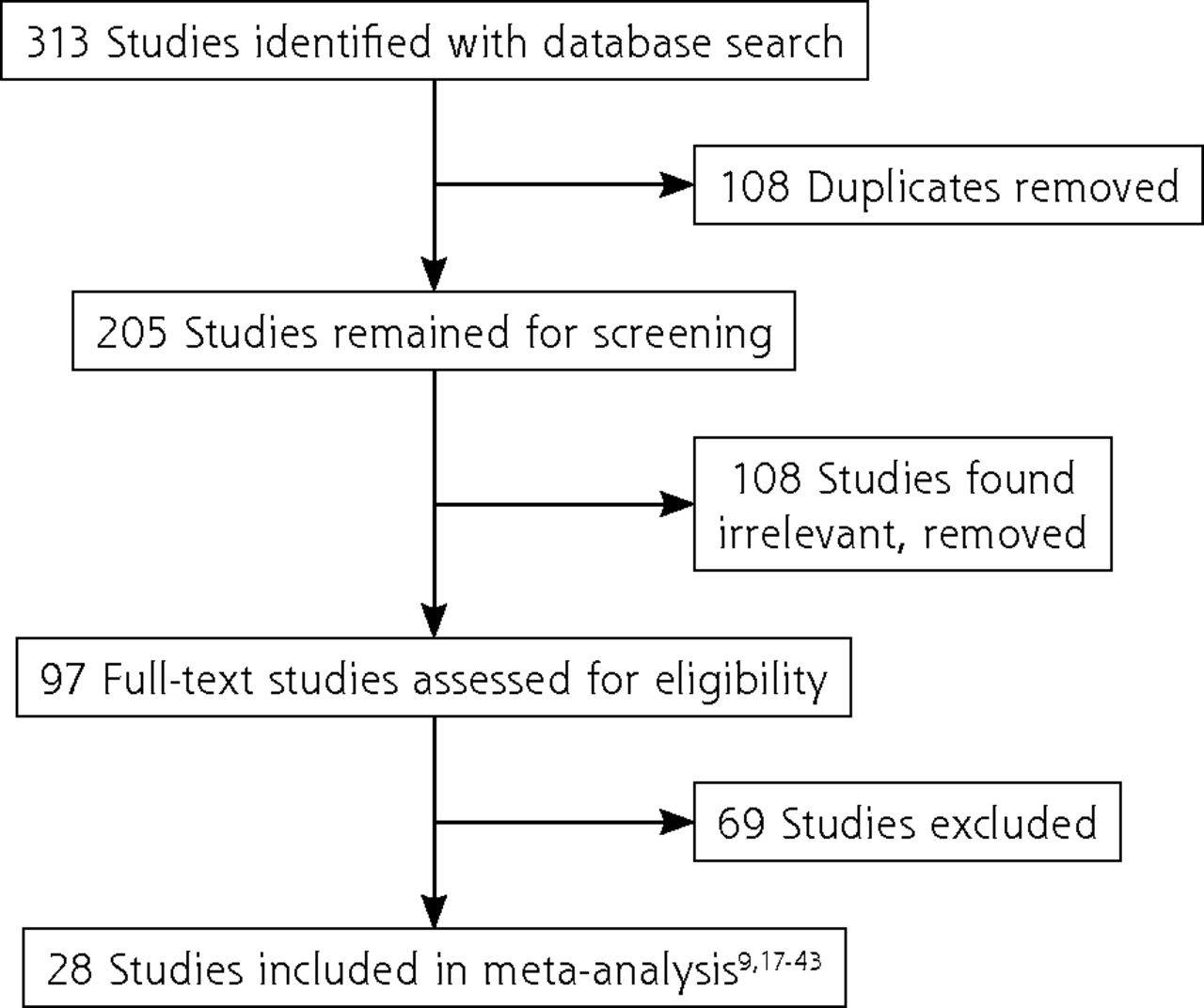
We found 313 studies in our initial search of the databases. After removal of 108 duplicates, 205 studies remained for screening. Of those screened, 108 studies were considered irrelevant according to review criteria leaving 97 full-text studies to assess for eligibility. From the review of full text, 69 studies were excluded. Reasons for exclusion included: (1) the format was a conference abstract, editorial, review, or a workshop proceeding; (2) vaginal swabs and urine were not compared head-to-head, or there was not an appropriate reference quality standard; (3) assay(s) were not commercially available; and (4) the sensitivity was not discernible from the data presented. We identified 28 eligible articles as outlined in Figure 1.9,17-43

Prisma flowchart of included articles.
Studies included a mixture of symptomatic and asymptomatic women seeking evaluation at primary care settings, community health organizations, and clinics specializing in sexually transmitted disease, obstetrics and gynecology, or family planning. Assays in the analysis include: ligase chain reaction and RealTime CT/NG polymerase chain reaction (PCR) assay (Abbott Laboratories); Amplicor PCR assay, and cobas PCR assay (Roche Diagnostics); transcription-mediated amplification and hybridization protection assay (Hologic); ProbeTec strand displacement amplification, MAX CTGCTV, and CTGCTV2 real-time PCR assays (Becton, Dickenson and Company); Dx CT/NG/MG real-time PCR assay (Bio-Rad Laboratories, Inc); CT/NG Xpert Rapid real-time PCR and Xpert TV PCR (Cepheid); AmpliSens N. gonorrhoeae / C. trachomatis / M. genitalium / T. vaginalis-MULTIPRIME-FRT PCR kit (Ecoli Dx); and Solana Trichomonas Assay using helicase-dependent amplification (Quidel Corp). Characteristics of each study, including the year of publication, the included population, organism studied, index assay, and quality reference standard, are presented in Table 1.
Characteristics of Studies Included in the Meta-Analysis
Chlamydia trachomatis
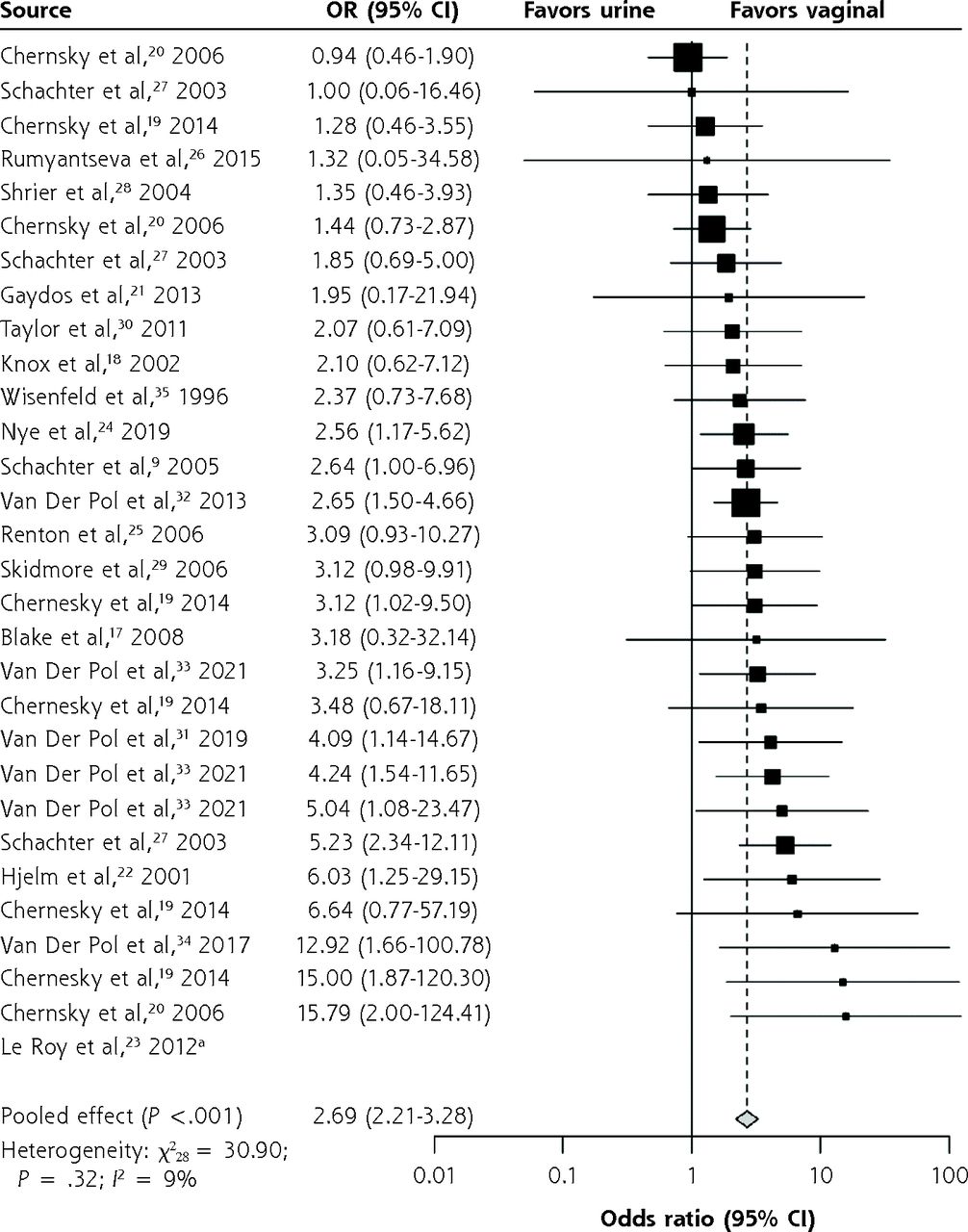
Since some studies presented vaginal swab and urine data from multiple assays (eg, vaginal swabs and urine samples from the same patient were tested, and contributed to data for more than 1 assay), those studies contributed more than a single comparison because each assay could be compared individually. Thus, 20 studies contributed 30 comparisons of CT detection. Pooled sensitivity estimates from the studies were 94.1% (95% CI, 93.2%-94.9%) for vaginal swabs and 86.9% (95% CI, 85.6%-88.0%) for urine specimens (P <.001). The OR that the difference was in favor of vaginal swabs was 2.69 (95% CI, 2.21-3.28), P <.001 for CT (Figure 2).

Difference in assay sensitivity between vaginal swabs and urine in the detection of Chlamydia trachomatis.
OR = odds ratio.
a Non-calculable due to 100% sensitivity.
Neisseria gonorrhoeae
For NG, 10 studies contributed 16 comparisons. The pooled sensitivity estimates were 96.5% (95% CI, 94.8%-97.7%) for vaginal swabs and 90.7% (95% CI, 88.4%-92.5%) for urine specimens (P <.001). The OR that vaginal swabs were more sensitive than urine for detection of NG was 3.68 (95% CI, 2.19-6.18), P <.001 (Figure 3).

Difference in assay sensitivity between vaginal swabs and urine in the detection of Neisseria gonorrhoeae.
OR = odds ratio.
Trichomonas vaginalis
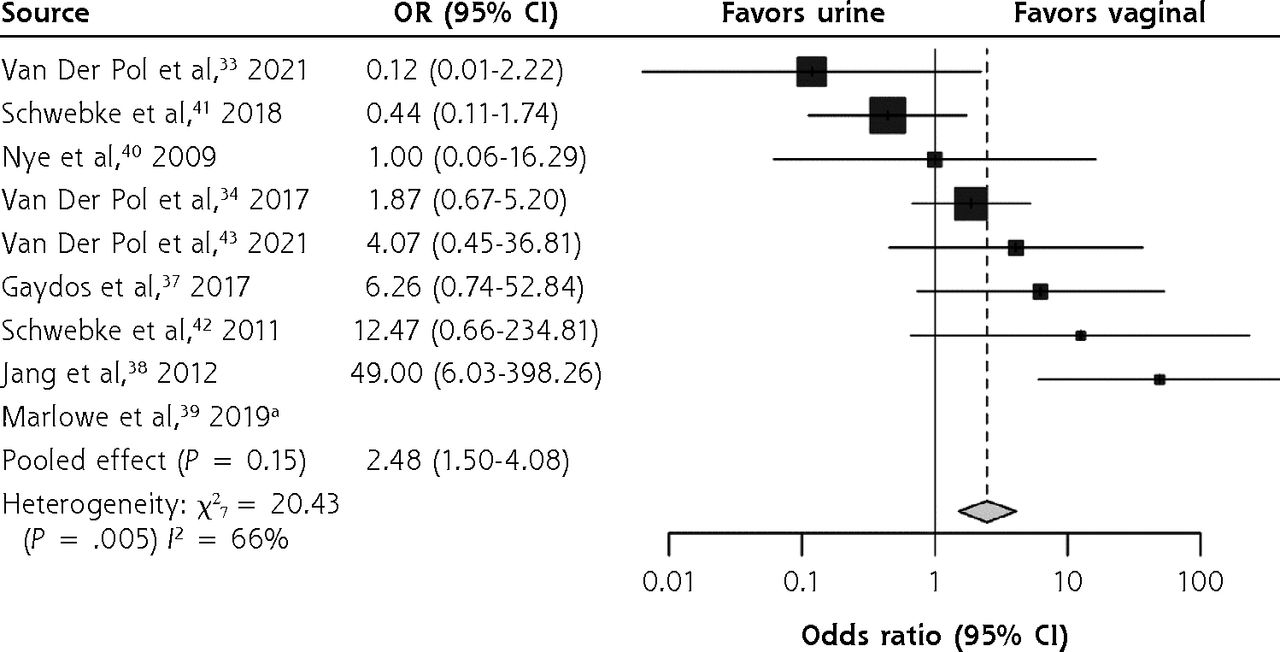
Nine studies contributed 9 comparisons of TV performance with vaginal swabs and urine. Pooled sensitivity estimates were 98.0% (95% CI, 97.0%-98.7%) for vaginal swabs and 95.1% (95% CI, 93.6%-96.3%) for urine specimens (P <.001). The difference in sensitivity for the 2 sample types for TV was not statistically significant with an OR of 2.48 (95% CI, 1.50-4.08), P = .15 (Figure 4).

Difference in assay sensitivity between vaginal swabs and urine in the detection of Trichomonas vaginalis.
OR = odds ratio.
a Non-calculable due to 100% sensitivity.
DISCUSSION
Areas of Uncertainty
The results from this meta-analysis indicate that vaginal swabs are more sensitive than urine for CT and NG. There is still some uncertainty about the noninvasive genital sample of choice for TV as more studies are needed. Public health laboratories have a key role in STI screening and testing.2 Although vaginal swabs are the recommended specimen type, the primary specimen type tested by public health laboratories for CT and NG among women was urine.2,44 Fewer than 10% of public health laboratories received vaginal swabs more frequently than other sample types.2,44 A study comparing US clinical laboratory chlamydia and gonorrhea testing practices before and after the 2014 CDC testing recommendations found minimal acceptance of preferred specimen types for CT and NG.3 Based on our estimates of a more than 6% lower sensitivity, and the CDC estimates of roughly 7 million cases per year of CT, NG, and TV,45 reliance on urine as a sample type for women could result in missing more than 400,000 infections. Furthermore, it should be noted that, when screening asymptomatic women, in compliance with annual recommendations, the organism load may be lower in these women and the most sensitive test is clearly called for. What will it take to convince health care clinicians to change their STI testing patterns? Implementation research is needed to address this question.
Guidelines
For female screening, the CDC has recommended vaginal swabs as the optimal specimen type for both CT and NG NAATs since 2014.1 Our data support and reinforce that recommendation by adding analyses of numerous publications since the evidence for the CDC recommendations was generated. While testing urine specimens is clearly better than no testing at all, there are few barriers to adoption of vaginal swabs, particularly given that assays have claims for patient-obtained vaginal swabs which can be collected before the provider exam. In those settings where NAAT point-of-care testing has been adopted, clinical programs have shown that “Sample First” collection immediately after registration allows improved clinic flow and can facilitate same day test-and-treat strategies.46
CONCLUSION
The pooled sensitivity for vaginal swabs was consistently greater than that of urine; however, for TV, the OR that vaginal swabs were more sensitive than urine did not reach statistical significance. Since TV had a small sample size and moderate to high heterogeneity,16 we were conservative in using a random effects model; however, if a fixed effects model was used, the OR that vaginal swabs were more sensitive than urine was statistically significant.
We must mention the lack of data available for transgender individuals; however, one can posit that among transgender and gender diverse people who participate in receptive vaginal sex, the organism load is most likely higher in the vaginal or neovaginal space if compared with urine; however, this is an area in need of further research. An additional limitation is that too few studies provided sufficient data to allow us to make separate estimates for symptomatic vs asymptomatic women, but it is reasonable to postulate that the sensitivity differential might be greater among asymptomatic women because of lower organism load. Since this meta-analysis combines symptomatic and asymptomatic patients, meaning for some it is a diagnostic test and others a screening test, this would result in a difference in pretest probability and would alter the predictive value. This could potentially alter a clinician’s calculus between accuracy and patient comfort; so, stratification by symptom status should be included in future research. Further, most of these data are from clinical studies assessing the performance of the assays and thus ensuring appropriate collection of urine (first-catch with no urination in the previous hour). One of the few studies4,5 that has evaluated mid-stream, clean-catch urine, compared with first-catch urine showed sensitivities of 86.2% and 89.8% (relative to vaginal swabs), respectively.5
A thorough sexual history by clinicians is essential in weighing the comfort level of a patient and the risks and benefits of using either self-collected or provider-collected vaginal swabs for screening and diagnostic testing. Self-collected vaginal swabs may be preferred, especially for patients with a trauma history as the patient may become upset if a provider performs the procedure. Many studies have demonstrated the acceptability and feasibility of self-obtained vaginal swabs; the data strongly support their use and have for decades.47-52 Collection of samples can, and should, be tailored to individual needs so that patients for whom vaginal sample collection may be a triggering experience can opt to provide urine. However, based on the large number of studies demonstrating a preference for self-obtained vaginal sampling, and the data shown here, vaginal sampling should be the initial choice offered to patients. Routine use of urine for screening women for CT and NG represents a disservice that may result in downstream consequences from false-negative results and untreated infections. We cannot continue to justify the use of urine except for women for whom collection of a vaginal sample is not acceptable. We strongly encourage clinicians to use the genital sample type for women recommended by the CDC and supported by the evidence in this review for laboratory testing for the sexually transmitted infections CT, NG, and TV.
Footnotes
Conflicts of interest: B. VDP. receives research support, consulting fees and/or honorarium from the following: Abbott Molecular, BD Diagnostics, BioFire Diagnostics, Hologic, Rheonix, Cepheid, Roche, and Visby. The other authors report none.
Read or post commentaries in response to this article.
- Received for publication August 29, 2022.
- Revision received November 6, 2022.
- Accepted for publication November 21, 2022.
- © 2023 Annals of Family Medicine, Inc.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Home-based self-collection of biological samples, including vaginal swabs: a mixed methods study for Britains fourth National Survey of Sexual Attitudes and Lifestyles (Natsal-4)
- Sexually Transmitted Infections: Update on Screening and Follow-Up Recommendations
- Risk factors for curable sexually transmitted infections among youth: findings from the STICH population survey in Zimbabwe
- At-home specimen self-collection as an additional testing strategy for chlamydia and gonorrhoea: a systematic literature review and meta-analysis
- Growing Evidence Supports an Implementation Shift Toward Vaginal Sampling for Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis Screening