
Abstract
PURPOSE Over 29 million Americans have alcohol use disorder (AUD). Though there are effective medications for AUD (MAUD) that can be prescribed within primary care, they are underutilized. We aimed to explore how primary care physicians familiar with MAUD make prescribing decisions and to identify reasons for underuse of MAUD within primary care.
METHODS We conducted semistructured interviews with 19 primary care physicians recruited from a large online database of medical professionals. Physicians had to have started a patient on MAUD within the last 6 months in an outpatient setting. Inductive and deductive thematic analysis was informed by the theory of planned behavior.
RESULTS Physicians endorsed that it is challenging to prescribe MAUD due to several reasons, including: (1) somewhat negative personal beliefs about medication effectiveness and likelihood of patient adherence; (2) competing demands in primary care that make MAUD a lower priority; and, (3) few positive subjective norms around prescribing. To make MAUD prescribing a smaller component of their practice, physicians reported applying various rules of thumb to select patients for MAUD. These included recommending MAUD to the patients who seemed the most motivated to reduce drinking, those with the most severe AUD, and those who were also receiving other treatments for AUD.
CONCLUSIONS There is a challenging implementation context for MAUD due to competing demands within primary care. Future research should explore which strategies for identifying a subset of patients for MAUD are the most appropriate and most likely to improve population health and health equity.
INTRODUCTION
Over 29 million Americans have alcohol use disorder (AUD).1 AUD is responsible for substantial morbidity and mortality.2-4 Yet, only 8.7% of individuals with AUD receive treatment in a given year.2,4 Efficacious medications, including naltrexone, acamprosate, and disulfiram, exist but have been slow to diffuse into practice.5-7
While AUD is commonly treated in specialty behavioral health treatment settings, treatment can be effectively delivered in primary care.8,9 Given that many communities lack specialty behavioral health clinicians, expanding access to medications for AUD (MAUD) in primary care may be a key strategy to increase uptake.10-12 A 2021 literature review of barriers to pharmacotherapy for AUD in outpatient settings found challenges in 3 key domains: (1) lack of physician knowledge, concerns about efficacy, and complexity of prescribing; (2) treatment philosophy and stigma (eg, assumptions that patients with AUD are non-adherent); and (3) medication accessibility, including geographic and socioeconomic barriers.13 Many studies in this review were dated (eg, published before the release of acamprosate in 2004) and focused on clinicians who never or rarely prescribed MAUD. Barriers to MAUD within primary care are likely very different for clinicians who never prescribe MAUD (eg, due to philosophical objections to MAUD or a belief that AUD should be treated by behavioral health specialists) vs for those who have some familiarity with MAUD and express a willingness to prescribe yet do not do so consistently (eg, due to competing demands within primary care).13
Prior studies have used the theory of planned behavior (TPB) to explore prescribing behaviors.14 In this framework, behavioral intention (ie, primary care physician decision to prescribe MAUD) is predicted by 3 variables: attitude toward prescribing, subjective norms, and perceived behavioral control over prescribing.15,16 Relevant attitudes include but are not limited to: familiarity with MAUD, beliefs about MAUD effectiveness/impact on patient outcomes, beliefs about MAUD safety and side effects, and perceptions of how MAUD compare with other AUD treatments.17 Subjective norms relate to an individual’s perceptions of others’ beliefs and practices (eg, perceptions of patient demand for MAUD or of colleagues’ prescribing behaviors) and the desire to conform. Perceived control refers to beliefs about barriers and the difficulty of prescribing MAUD.17 A key strength of the TPB is that it has been shown to predict a diverse set of health behaviors.18-20 It also has some recognized limitations, however, including that it does not fully account for environmental and economic influences21,22 or consider factors like mood and emotions.23
There is a dearth of research on how primary care physicians approach the prescribing of MAUD and strategies that can increase consistent use among those who are open to prescribing. To address this gap, we conducted interviews with primary care physicians who had experience with MAUD. We aimed to apply TPB to explore their decision-making processes and identify reasons for underuse of MAUD in primary care.
METHODS
Study Participants and Sampling Strategy
From June 8 through July 9, 2022, we conducted semistructured interviews with 19 primary care physicians practicing in outpatient settings. To recruit, we worked with a research firm with an online panel of 730,000 physicians. The panel comprises physicians who have joined the platform to access clinical content and continuing medical education activities and has been used in multiple research studies.24-26 We limited our sample to physicians to increase the likelihood that we would obtain saturation with a sample size of 15-25, as clinicians with different training (eg, nurse practitioners, physician assistants) are likely to have different perspectives on prescribing. Further, we limited the sample to physicians who had some experience with MAUD to focus on barriers to assimilation (ie, consistent use of MAUD across all patients who may benefit) rather than the unique barriers among those who have never prescribed (eg, philosophical objections to MAUD).
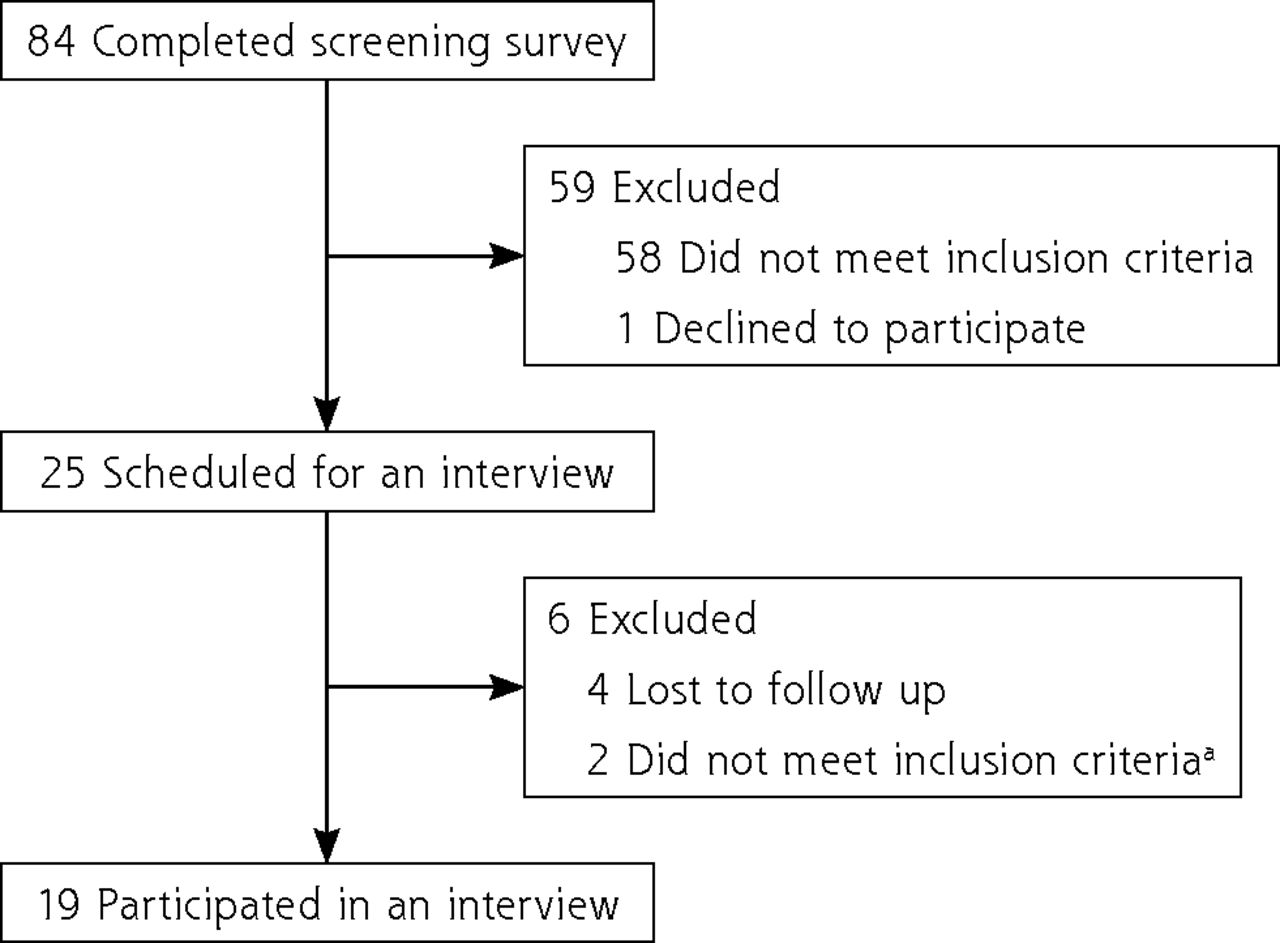
Physicians in the panel were sent a 7-item screening survey to assess eligibility (Supplemental Appendix). Those deemed eligible were invited to participate in a 60-minute videoconferencing interview. Eligible participants included internal medicine and family medicine physicians who treated adults. Further, participants needed to have started at least 1 patient on a Food and Drug Administration-approved MAUD (disulfiram, naltrexone, and/or acamprosate) in the prior 6 months. Moreover, they needed to work in an outpatient setting, providing direct clinical care for 10 or more hours per week. We conducted criterion sampling, but we also sampled for heterogeneity to ensure that the final sample of primary care physicians varied with respect to practice setting and US region. Details on the screening process and how we arrived at our final sample are featured in Figure 1.

Recruitment Flow Diagram
MAUD = medications for alcohol use disorder.
a Several participants reported they had started 1 or more patients on MAUD in the last 6 months in the screening questionnaire but reported, during the interview, that they had not prescribed MAUD in the last 6 months and therefore did not to meet inclusion criteria.
Theory of planned behavior informed both the selection of questions in the interview protocol and the codebook used for the analysis.17 We applied this framework because it is one of the most common frameworks used to describe prescribing behavior, but has seldom been applied to MAUD prescribing.14 Interviews followed a semistructured protocol that incorporated questions related to TPB variables as well as critical incident technique questions.
Critical Incident Technique
We used the critical incident technique to uncover unconscious factors that influence the decision to prescribe MAUD. This method asks participants to reflect on real-life experiences and collects records of specific behaviors. The technique has been used in previous studies to explore prescribing and referral behaviors.27-30 We asked primary care physicians to describe an example of a time that they prescribed MAUD to a patient and felt very good about it and an example of a time they prescribed MAUD and felt uneasy or uncomfortable about it.
Three members of the study team (A.B., J.L.S., L.U-P.), trained in qualitative research, conducted the interviews. Interviews were recorded and transcribed. Participants received a $150 gift card for their participation and provided verbal informed consent.
Data Analysis
We analyzed interview data by using inductive and deductive content analysis.31 We first developed a codebook that incorporated TPB domains. We then added new codes based on themes that emerged from the data. We considered decision-making factors that participants reported consciously considering (ie, when asked directly what factors influence their decisions) and subconscious factors identified by the study team (ie, explored through follow-up questions when participants described their decision-making processes with particular patients). As in prior work, we treated conscious and subconscious factors as equally important and compared findings across the 2 types of responses.32
The senior author (L.U-P.) developed the initial codebook by reviewing 6 transcripts. The codebook was then discussed, refined, and finalized in group meetings (including A.B., L.U-P., and J.L.S.). Both the lead author (A.B.) and senior author (L.U-P.) coded all transcripts. Discrepancies were discussed and resolved through consensus. In developing themes, we used several indicators of salience including the number of different participants who exemplified a particular concept, the time spent or emotion conveyed, and the consistent conceptualization of a concept across participants. This approach is consistent with the robust phenomenological approaches used in qualitative methods.33
Analyses began after 3 interviews had occurred, and saturation was reached (ie, no new themes emerged) after 16 interviews.34 Three additional interviews (total of 19) were conducted to confirm that saturation was reached. The full research team of 8 authors is multi-disciplinary and includes health services researchers, economists, and 2 clinicians (A.B.B., J.L.S.). Our research team began this work with the belief that AUD is under-treated in primary care, and that many patients who are not currently receiving MAUD may benefit from it. Further, we assumed that stigma against patients with problematic alcohol consumption may be playing a role in under-treatment. This study was approved by RAND’s Institutional Review Board.
RESULTS
Nineteen primary care physicians from 13 states in the United States participated (Table 1). The largest group of participants (47%) worked in group practices not affiliated with a hospital, and 26% worked in hospital-based outpatient clinics. Nearly all participants (90%) had experience prescribing naltrexone in the prior 6 months, while a majority had experience prescribing disulfiram (68%) and acamprosate (58%).
Participant Characteristics (N = 19)
Results Overview
A key finding was that participants reported a challenging implementation context for MAUD within primary care. There were 3 distinct themes within this domain, including: (1) somewhat negative personal beliefs about medication effectiveness and likelihood of patient adherence; (2) competing demands in primary care that make MAUD a lower priority; and, (3) lack of subjective norms around prescribing. Although multiple participants reported consistently screening for AUD and discussing MAUD with all patients with AUD, some participants reported strategies to make MAUD prescribing a smaller, more manageable component of their practice because of the challenging implementation context and the fact that AUD is so common. They reported applying various “rules of thumb” to select particular patients to engage for longer discussions about MAUD. These rules typically involved identifying patients with the most severe AUD, patients who were currently in psychotherapy or had tried it in the past, or patients who were perceived to be the most motivated to reduce their drinking.
Challenging Implementation Context
Theme 1: Somewhat Negative Personal Beliefs About Medication Effectiveness and Likelihood of Patient Adherence
While most participants had positive views about the effectiveness of 1 or more MAUD drugs, several shared negative beliefs about MAUD, most of which focused on their perceptions of MAUD’s limited effectiveness in treating addiction and the likelihood of poor patient adherence. These beliefs corresponded to the attitudes about prescribing domain in the TPB. Among the subset of participants with more negative beliefs, there was a general sentiment that MAUD does not work very well as a standalone treatment. A family medicine physician from California explained, “[Medication] really doesn’t change the root cause of why people have addiction, whatever trauma caused them to be addicted to whatever, if they’re anxious, if they’re depressed, whatever that actual issue is…Medication by itself is not the best.” Further, multiple participants explained that although medications can be effective when used as prescribed, patients may not adhere for a variety of reasons (eg, side effects, impact of drinking while on medications, need to take multiple pills per day in the case of acamprosate). According to an internal medicine physician from Ohio, “If they take disulfiram and they drink, they’ll get sick, but they stop the disulfiram, not the alcohol.” Views about disulfiram were particularly negative, even among participants who had favorable views of MAUD in general.
Theme 2: Competing Demands in Primary Care That Make MAUD a Lower Priority
Within the TPB domain of perceived behavioral control, the majority of participants mentioned that treating AUD is time consuming and complex and can divert attention away from other pressing medical needs. They generally reported that prescribing MAUD was a process that required ongoing conversations with patients over many months. Further, a couple of participants suggested that patients with AUD can be particularly difficult to work with due to medication non-adherence, not believing that they have AUD, and/or beliefs that they can handle their addiction without medications.35 Physicians compared AUD patients with those having common illnesses like diabetes and mentioned that in comparison, AUD patients were less likely to acknowledge or accept medication treatment for their illness. Given short appointments and competing demands, multiple participants believed that AUD treatment should be managed by a psychiatrist or someone trained in addiction medicine, rather by the primary care clinician. As a family medicine physician from Massachusetts explained, “AUD is a disease state at the bottom of the list for them [primary care physicians]. But primary care is kind of right now, so overburdened with management of diabetes, hypertension, cholesterol, depression, anxiety disorders, chronic obstructive pulmonary disorder, asthma, migraine. So, if a patient comes in and they have three or four of the above conditions I mentioned, they [those conditions] get the priority.” An internal medicine physician from Ohio said, “A lot of times these are big discussions, the patients talk, and talk, and talk…Then you got to get them taking medication, so you got to go over that, then you’ve got to deal with if they’re taking it or not taking it.”
Theme 3: Few Positive Subjective Norms Around Prescribing
The TPB posits that a physician is more likely to prescribe MAUD if there are strong, positive subjective norms around the behavior. In other words, if physicians believe that their peers prescribe MAUD and that their peers and patients expect them to prescribe, they will be more likely to prescribe. We did not identify examples of positive subjective norms around prescribing MAUD. First, almost all participants, including those who were trained after naltrexone and acamprosate were approved by the FDA, reported that they did not receive formal training or formalized guidelines on MAUD as part of their medical education. Lack of training has several impacts. First, it results in lack of knowledge about MAUD among primary care physicians and reduces comfort in prescribing. Second, it sends the message that primary care physicians do not consider MAUD to be an essential component of primary care practice. Third, several participants spoke about broad resistance to MAUD among certain groups of primary care physicians. A family medicine physician from New York reported, “There is a population where some clinicians are philosophically opposed to these medications or don’t think they work.” Finally, participants mentioned that patients seldom ask about or demand MAUD due to lack of awareness. Multiple participants contrasted MAUD with medications used to treat opioid use disorder and pointed out there is greater demand for medications for opioid use disorder. An internal medicine physician from Ohio explained, “I’ve never heard anybody ask for medication to stop alcohol abuse, no. For opioids, yes.”
It should be noted that participants identified a set of additional miscellaneous barriers to MAUD that did not map to one of the 3 themes above. For example, participants mentioned costs to patients, lack of insurance coverage, and lack of prescribers and resources for complementary services (eg, therapy) in certain communities.
Rules of Thumb
As stated above, we identified 3 rules of thumb that some participants used to identify a subset of patients with AUD who would be good candidates for MAUD. These rules of thumb served to make MAUD prescribing (with its complexities) a more manageable component of their practice.
Theme 4: Recommending MAUD Only to Patients Currently or Previously in Psychotherapy or Self-Help Groups
Multiple participants felt that MAUD was most effective when used in combination with other treatments such as individual psychotherapy or Alcoholics Anonymous. As a family medicine physician from California described, “Obviously the multimodal combination of everything is the most successful. Medication by itself I feel like is the least effective, but if you are able to do both of them together, it’s the highest success rate.” A handful of participants reported only recommending MAUD to patients who were also receiving non-pharmacologic treatments.
Theme 5: Recommending MAUD Only to Patients Perceived as Highly Motivated to Reduce Their Drinking
Some participants reported that they only recommend MAUD to patients who they believe are motivated. However, participants used different indicators of motivation. Participants percieved patients that had been recently hospitalized, had just relapsed after a period of abstinence, were specifically seeking help for AUD, had tried various types of therapies in the past without success, or had strong support networks, as motivated. According to a family medicine physician from Maryland, “Usually if they’re seeking help, they’re more likely to be adherent to a program rather than me just saying, ‘Well, you scored high on this questionnaire.’”
Theme 6: Recommending MAUD Only to Patients With the Most Severe AUD
Some participants mentioned that they assess the level of AUD and only recommend MAUD to patients with the most severe AUD, which they categorized as the heaviest drinkers or those with more advanced medical consequences of AUD. According to an internal medicine physician from Pennsylvania, “I think we kind of see how bad it is. If it’s a mild abuse and it happens once in a while, maybe we can ask them to try without the medication.”
Additional Rules of Thumb
It should be noted that we identified additional rules of thumb that were only mentioned by 1 or 2 participants. For example, a family medicine physician from New York mentioned that they only feel comfortable prescribing MAUD to patients who had been on MAUD in the past, and a family medicine physician from Washington, DC reported that they preferred to prescribe MAUD to patients with whom they had longer-term relationships.
DISCUSSION
Our study revealed a challenging implementation context characterized by somewhat negative beliefs about effectiveness, competing demands, and perceived lack of positive subjective norms for MAUD that led some primary care physicians to implement strategies to make MAUD a smaller component of their practice. Interestingly, our findings showed that primary care physicians who prescribe and have familiarity with MAUD reported many of the same barriers as those who do not prescribe.13 For example, somewhat negative views about the effectiveness of MAUD in general (or about specific AUD medications), lack of training, and discomfort with prescribing MAUD were commonly reported.36,37 Our results suggest that addressing skepticism about effectiveness across these populations of primary care physicians may be important. This could be achieved by setting expectations that medications for AUD can be helpful even if they are unlikely to be a magic bullet. Further, it may be helpful to build integration structures that connect primary care physicians to specialty substance use disorder treatment clinicians, given that primary care physicians often perceive MAUD to be most effective in combination with other treatments that can be difficult to access.
A key contribution of this study is the identification of rules of thumb to guide prescribing decisions. Numerous studies have documented the rules of thumb (heuristics) that clinicians apply to reduce mental strain.38 While heuristics have some value in helping decision makers deal with complexity, they can lead individuals to ignore certain pieces of information and overemphasize others. Given the competing demands in primary care, applying rules of thumb seems to be a sensible response. A 2022 study by Porter et al showed it would take primary care physicians 27 hours per day to provide guideline-recommended care to a hypothetical patient panel.39 Strategies to increase use of MAUD in primary care, such as requiring specific training, address some substantial barriers but do not solve the broader problem. Team-based care and other efforts to distribute labor-intensive counseling tasks to other clinicians may be helpful. But, it is unclear if these types of rules of thumb are applied to other conditions treated within primary care, and whether efforts to contain prescribing to certain patients are a manifestation of stigma against patients with problematic drinking. One key danger of applying rules of thumb is that it could exacerbate disparities in access to treatment across subpopulations with AUD. For example, determining whether a patient is motivated to reduce their drinking is subjective and subject to bias.
Limitations
This study has several limitations. First, we only engaged primary care physicians who had prescribed MAUD within the last 6 months; thus, we do not know if these findings apply to primary care physicians who are not currently prescribing. Further, we did not systematically collect data about the patient populations of primary care physicians in our sample. As a result of this and the sample size, we cannot assess if themes vary by location or patient characteristics (eg, proportion who are low income). Lastly, when applying a model such as the TPB, there is always a risk of overfitting the results to the model.
CONCLUSION
Our study showed that there is a challenging implementation context for MAUD due to competing demands within primary care. These findings help to explain why MAUD is underutilized in primary care settings. Even among primary care physicians who routinely prescribe, we found evidence of lack of assimilation (ie, consistent prescribing with every patient who may benefit). Future research should explore which strategies for identifying a subset of patients for MAUD are the most appropriate and most likely to improve population health and health equity.
Footnotes
Conflicts of interest: authors report none.
Funding support: NIAAA R01AA029267; NIDA P30 DA035772
- Received for publication October 26, 2023.
- Revision received March 31, 2023.
- Accepted for publication April 3, 2023.
- © 2023 Annals of Family Medicine, Inc.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.