
Abstract
PURPOSE Family physicians rapidly shifted to using virtual care during the COVID-19 pandemic, yet it is largely unknown if this change has impacted their workplace motivation. A better understanding of this matter is essential for optimizing the integration of virtual care into standard practice and for supporting family physician well-being. Using a self-determination theory lens, we examined if family physicians experienced autonomous (vs controlled) motivation toward using virtual care, how this related to their subjective well-being, and whether satisfaction (vs frustration) of their basic psychological needs at work mediated that relationship.
METHODS Using cross-sectional survey methodology, quantitative data was collected from 156 family physicians in Alberta, Canada. The questionnaire contained validated scales for measuring motivational quality, workplace need fulfillment, and subjective well-being. Descriptive, correlational, and mediation analyses were performed.
RESULTS Family physicians varied significantly in their quality of motivation towards using virtual care. Controlled motivation toward using virtual care was associated with lower well-being, and workplace need frustration fully mediated that relationship. Conversely, workplace need satisfaction, but not autonomous motivation toward using virtual care, was associated with higher well-being.
CONCLUSIONS In line with self-determination theory, findings suggest that when family physicians’ motivation toward using virtual care is less self-determined, it will lead to poorer subjective well-being, because of basic psychological need frustration. Potential implications of the findings are discussed within the contexts of virtual health and primary care.
INTRODUCTION
Meeting patient needs is a timely topic, given the disruptions that COVID-19 and virtual care have caused. As we strive to optimize the integration of virtual technology into standard practice, however, we must also consider the needs of health care workers. Self-determination theory (SDT) posits that autonomy, competence, and relatedness are universal human needs, and that their hindrance will constrain people’s motivation, health, and well-being.1 This study tests this proposition in a virtual health care context, and it investigates family physicians’ motivation toward using virtual care and how that relates to their need fulfillment and well-being at work.
Self-determination theory is a leading theory in human motivation and well-being.1 It posits that people will naturally seek to self-govern, connect, and grow, but that to flourish, they require support for 3 basic psychological needs: autonomy (ie, volition), competence (ie, mastery), and relatedness (ie, connectedness).1 Self-determination theory proposes that need satisfaction facilitates internalization and thus autonomous motivation (eg, based on perceived importance and value) and well-being, whereas need frustration triggers controlled motivation (eg, based on perceived pressures) and ill-being. Self-determination theory therefore distinguishes between different types of motivation, ranging from fully externally motivated (least self-determined) to fully internally motivated (most self-determined).2
The concept of basic psychological needs is key in primary care.3,4 Virtual care, however, presents barriers to need satisfaction for family physicians. For some, shifting to virtual care may signal the loss of human contact and the style of medicine they prefer.5 Virtual care may also bring concerns about governance of compensation, and how commercial third-party health care companies that offer walk-in style virtual medicine are jeopardizing continuity of care.6 Although virtual care was instrumental in providing care during the COVID-19 pandemic,7 there is an undeniable sentiment among physicians that it is less fulfilling than standard patient care.8,9 As others have explained, this is why we need to look beyond the practical elements of virtual care, to the psychological values and views of stakeholders who are being asked to adopt it.8 Research on this is underway, but how virtual care impacts physician motivation, behavior, and well-being is still unclear.9
Interestingly, Keenan et al8 found that while virtual care supported patients’ basic psychological needs, physicians perceived more opportunities for it to thwart those needs for patients. They linked this discord to the challenge physicians face when trying to balance their patients’ goals and expectations with their own.8 Through interviewing health care professionals, Kozikowski et al10 identified themes with virtual care and basic psychological needs: pros and cons of scaling, impact of technology on staff autonomy and clinical competence, and quality of patient-health care professional relationship. They emphasized the importance of considering medical professionals’ perceived benefits and concerns with virtual care to optimize its integration. In another study examining the health care climate, patients rated virtual (vs standard) visits with their family physician as less autonomy-supportive.11 The authors emphasized that going “virtual” may hinder motivation within the patient-doctor relationship.
Current Study
Empirical evidence has implicated basic psychological needs in patients’ motivations to engage in virtual care.6,11,12 Yet, less is known about what factors influence health care clinicians’ motivation toward using virtual care.8,13,14 Studies have also focused more on patient-physician dynamics within the telerehabilitation sphere,15 and less in other domains, such as pediatrics,16 psychiatry,17 and family medicine.18 A better grasp of how virtual care is impacting family physicians’ motivation and well-being is thus essential, particularly in view of our reliance on primary care practitioners and the potential for virtual care to negatively affect them. The present study addresses this gap in the literature by investigating how family physicians’ motivation toward using virtual care impacts their well-being, and whether their workplace need fulfillment mediates that relationship. Grounded in SDT, our hypotheses were:
Family physicians’ quality of motivation toward using virtual care will vary substantially.
Autonomous motivation toward using virtual care will positively relate to subjective well-being and workplace need satisfaction will mediate that relationship.
Controlled motivation toward using virtual care will negatively relate to subjective well-being and workplace need frustration will mediate that relationship.
METHODS
Participants and Procedure
A cross-section of family physicians in Alberta, Canada, was invited to complete an anonymous online survey containing demographic questions and 3 common and freely available questionnaires (see Measures, below, for descriptions, and Supplemental Appendix 1 and Supplemental Appendix 2 for items). Based on the rule of 20 cases per predictor variable (5 in this study), we calculated a minimum sample requirement of 100 physicians. Invitations were sent via listservs, academic newsletters, Alberta Medical Association primary care networks, and the Alberta College of Family Physicians and Well Doc Alberta websites. Invitations contained a consent form with study information and a link to the survey. Participation was voluntary and all were assured that confidentiality would be maintained. This research was approved by the Human Research Ethics Boards at the University of Calgary (#21-1440) and University of Alberta (#Pro00120804).
Measures
Motivation Toward Using Virtual Care
We used the 24-item Comprehensive Relative Autonomy Index (CRAI), which measures a person’s quality of motivation toward engaging in some activity along SDT’s autonomy continuum.19 Its psychometric properties, including its 2 main subscales (controlled and autonomous motivation), have been rigorously tested and validated among various populations.2,19,20 In this study, the CRAI was used to measure how autonomously motivated family physicians were toward using virtual care. Participants answered questions about why they engage in this activity, on a Likert scale from 1 (not true at all) to 7 (very true). Higher subscale scores indicate stronger motivation, either controlled or autonomous.
Workplace Need Fulfillment
We used the 24-item Basic Psychological Need Satisfaction and Frustration Scale–Work Domain (BPNSFS),21 which measures people’s autonomy, competence, and relatedness satisfaction/frustration at work, over the past 4 weeks. It is a widely used measure that has been shown to have strong psychometric properties.21 The BPNSFS has 2 main subscales and participants rate their agreement with items corresponding to each need, on a scale from 1 (strongly disagree) to 7 (strongly agree). Higher subscale scores indicate higher need satisfaction or frustration.
Well-Being
We used the 24-item BBC Subjective Well-Being Scale (BBC-SWB), which measures a person’s experiences across various well-being domains (psychological, physical health, and relationships). It is considered valid and reliable, based on a large-scale study published in 2013.22 The BBC-SWB contains 3 subscales and participants indicate their agreement with the statements as they apply to their lives, using a 5-point Likert scale from 1 (not at all) to 5 (extremely). Higher scores indicate higher well-being.
Statistical Analyses
Qualtrics (Qualtrics International Inc) and SPSS 25.0 (IBM Corp) were used for our survey and analyses. We addressed the issue of missing data, which occurred to a small degree in approximately 30% of surveys, by imputing sample mean scores.23 First, we aggregated the CRAI factors into the controlled and autonomous subscales,19,20 and the need subscales into mean scores for overall need satisfaction or frustration.24,25 Then, because the 3 BBC-SWB factors tend to be highly correlated, we combined them to form a total subjective well-being score.22 All variables were standardized and univariate normality was confirmed by examining skewness and kurtosis. Descriptive statistics, Pearson correlation coefficients, and internal consistency coefficients (Cronbach α) were then computed for the study variables. These results informed the subsequent mediation analysis, which we carried out according to Baron and Kenny.26 The indirect effects of significant mediations were tested via a bootstrap estimation approach with 10,000 samples.27
RESULTS
Sample Characteristics
In total, 156 family physicians participated in this study. The sample was diverse in demographic background and use of virtual care (Table 1).
Sample Characteristics (N = 156)
Variable Relationships
Table 2 shows the results of the statistical analyses for the main variables. The strength of relationships was weak to moderate, and the directions as expected, based on SDT. Controlled motivation toward using virtual care positively related to workplace need frustration, and both of these factors negatively related to subjective well-being. Conversely, workplace need satisfaction positively related to subjective well-being. Autonomous motivation toward using virtual care was not a significant correlate of workplace need satisfaction or subjective well-being. With respect to demographics, virtual care use (r = −0.17, P = .04) and being female (r = −0.19, P = .02) both negatively related to workplace need satisfaction, while years in practice positively related to autonomous motivation toward using virtual care (r = 0.25, P <.01). There were no other significant correlations between the demographic and motivation variables.
Descriptive Statistics and Correlations Between Study Variables
Workplace Need Satisfaction
The correlational results indicated no relation between autonomous motivation toward using virtual care and workplace need satisfaction or subjective well-being. We thus performed a simple regression to assess how workplace need satisfaction predicted well-being, controlling for the significant demographic factors: virtual care use, gender, and years in practice. As hypothesized, the overall regression was statistically significant (R2 = 0.07, F (1,155) = 2.78, P = .03), and workplace need satisfaction positively related to subjective well-being (β = 0.26, P <.01).
Workplace Need Frustration
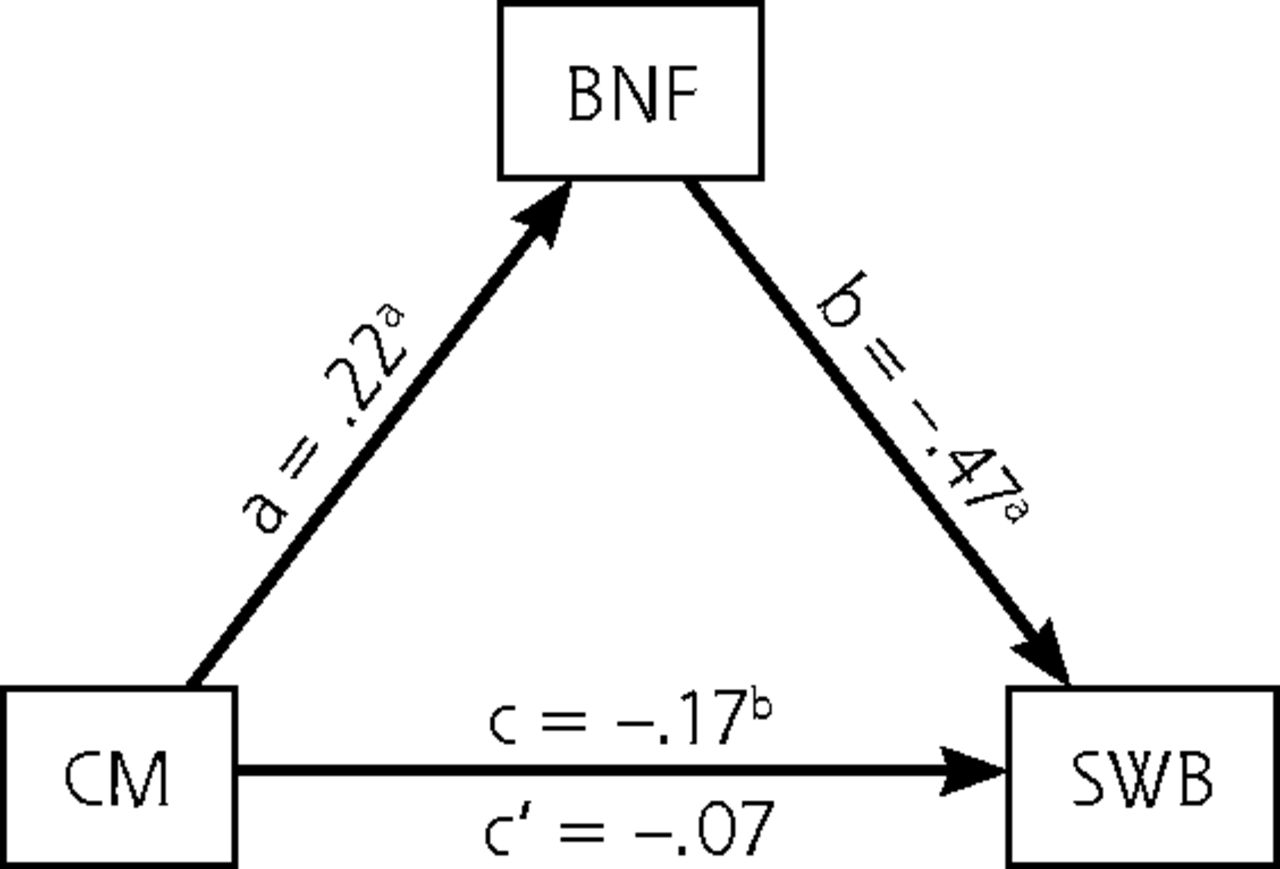
Next, we tested the hypothesized relationship between controlled motivation toward using virtual care, workplace need frustration, and subjective well-being, controlling for the same demographic factors as above. As seen in Figure 1, controlled motivation toward using virtual care significantly correlated with workplace need frustration (path a), and both variables were significant correlates of subjective well-being (paths b and c). Although the initial path (c) between controlled motivation and subjective well-being was significant, controlled motivation was no longer a significant correlate of subjective well-being after controlling for the mediator, workplace need frustration (path c′). These results were consistent with a full mediation. Approximately 21% of the variance in subjective well-being was accounted for by controlled motivation toward using virtual care (8%) and workplace need frustration (13%). Results of the bootstrap estimation approach with 10,000 samples indicated that the indirect coefficient for workplace need frustration was significant (β = −0.14, SE = 0.07, P <.01, 95% CI, −0.30 to −0.03). The negative coefficient indicated that each point increase in controlled motivation toward using virtual care was associated with approximately 0.15 points lower subjective well-being, as mediated by workplace need frustration.

Relationship between controlled motivation towards using virtual care and subjective well-being as mediated by workplace need frustration, controlling for virtual care use, gender, and years in practice.
a = effect of predictor on mediator; b = effect of mediator on criterion; BNF = basic psychological need frustration at work; c = total effect in the unmediated model; c′ = direct effect in the mediated model; CM = controlled motivation towards using virtual care; SWB = subjective well-being.
a P <.005 standardized regression coefficient.
b P <.05 standardized regression coefficient.
DISCUSSION
Using SDT as a lens, this study investigated how autonomously motivated family physicians were toward using virtual care in relation to their subjective well-being, and how their sense of workplace need fulfillment mediated that relationship. The following section discusses our findings and their implications within the virtual health and primary care context.
In this study, the sample was composed of family physicians with a variety of demographic backgrounds and levels of virtual care use (Table 1). There were more females (71%) than males (26%), with few identifying as non-binary (2%), and most identifying as White (65%) or Asian (24%). A 2019 Canadian Medical Association report showed a similar percent distribution of family physicians by age, except that the group aged 30-40 years was slightly over-represented, and the male group was slightly under-represented.28 Based on this national data, this study’s sample is fairly representative of the family physician population in Canada.
With respect to motivation, the family physicians endorsed relatively higher need satisfaction than frustration at work, but similar levels of autonomous vs controlled motivation toward using virtual care. As hypothesized, controlled motivation toward using virtual care related to lower subjective well-being, and workplace need frustration fully mediated that relationship. It surprised us to observe, however, that autonomous motivation toward using virtual care did not relate to workplace need satisfaction or subjective well-being. This may be because identifying with virtual care is not sufficient to satisfy one’s basic psychological needs in the way that feeling forced or disinterested in it might thwart them. This seems especially likely during the COVID-19 pandemic, given its global impact on physician burnout.29
Our findings align with SDT and suggest several key concepts. First, family physicians appear to vary considerably in their motivation toward using virtual care. Second, physician well-being in the digital era will partly stem from how well they can meet their basic psychological needs at work and how fully they internalize and integrate the value of virtual care, in that context. This mechanism helps explain the tension others have discussed, concerning patients’ and physicians’ unique goals when using virtual care.7,8,10,30 Our findings also extend prior work on how the COVID-19 pandemic and virtual care are impacting physician well-being.31,32 Constraints on meeting basic psychological needs seem to be a key consideration here, and that family physicians who sense that adopting virtual care is more of a “must” than a “want” may be introjecting societal pressures to adopt it in their practices and struggling, psychologically, as a result.
Theoretical and Practical Implications for Supporting Family Physicians
In SDT, internalization (the process of transforming values from external to internal) depends on autonomy support, which bolsters basic psychological needs and well-being, whereas controlling social contexts hinder need satisfaction and provoke ill-being.33 Hence, it follows that family physicians who are pressured to adopt virtual care would benefit from autonomy support at work. Self-determination theory outlines 3 main actions for supporting people’s autonomy: providing a meaningful rationale, acknowledging behaver feelings, and conveying a sense of choice.33 To us, acknowledgment of feelings is most important, because physician-representing organizations and professional associations often focus on incentives and similar solutions with virtual care, without necessarily addressing stakeholder emotions. It is also important, when assessing physician attitudes toward virtual care, that we move away from general satisfaction surveys. These types of measures are rarely psychometrically sound or theory based, which limits our understanding of, and our ability to properly support, physicians’ needs for well-being in the digital era.
Limitations and Future Directions
This study has several limitations. First, the data were from self-report measures collected via surveys, including physician’s estimated (vs objectively measured) use of virtual care. Thus, actual use of virtual care may have been over or underestimated. That said, this research did not concern physicians’ actual use of virtual care but rather their motivation toward using virtual care and its influence on their psychological needs and occupational well-being. Additionally, results are based on data from a single Canadian province, and though consistent with survey response rates in the health professions, there was a relatively small sample size.34 These limitations preclude causal conclusions and potentially limit generalizability. The BPNSFS also captures general levels of workplace need fulfillment and not specificially how fulfilling virtual care is. Finally, our analyses indicated some potential for demographics to influence physicians’ motivation toward using telehealth. Beyond controlling for these factors, however, exploring them (or other demographic factors) in further detail was beyond the scope of this study. Future research may therefore consider these aspects.
We attempted to mitigate these limitations by using well-established scales with strong psychometric properties, and by collecting data from a diverse sample of family physicians in Alberta. We also employed statistical methods that are considered robust, particularly with smaller sample sizes.26 Finally, findings aligned with a priori and theory-based hypotheses, and the family physicians’ workplace need fulfillment scores were comparable to others reported in the health professions education literature.35 These aspects support the validity and generalizability of our findings.
CONCLUSIONS
This study advances the discussion on the psychological impacts of virtual care in family medicine. Findings align with SDT and suggest that when family physicians are less autonomously motivated toward using virtual care, it will impede their integration of virtual care and undermine their sense of well-being. By extension, our results suggest that support for family physicians’ basic psychological needs will help mitigate this problem and promote a higher quality of motivation and sense of well-being at work. This study thereby provides new directions for research and interventions that aim to optimize the integration of virtual care into standard practice.
Acknowledgments
The authors wish to thank the Alberta Medical Association, Alberta College of Family Physicians, and Well Doc Alberta.
Footnotes
Conflicts of interest: authors report none.
Author contributions: All authors contributed to this study’s conception, ethical approval, and data collection. Data analysis and writing of the first draft of the manuscript were done by Adam Neufeld. All authors reviewed previous versions and approved the final version of the manuscript.
- Received for publication August 31, 2022.
- Revision received June 5, 2023.
- Accepted for publication July 25, 2023.
- © 2023 Annals of Family Medicine, Inc.
REFERENCES




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.