
Article Figures & Data
Tables
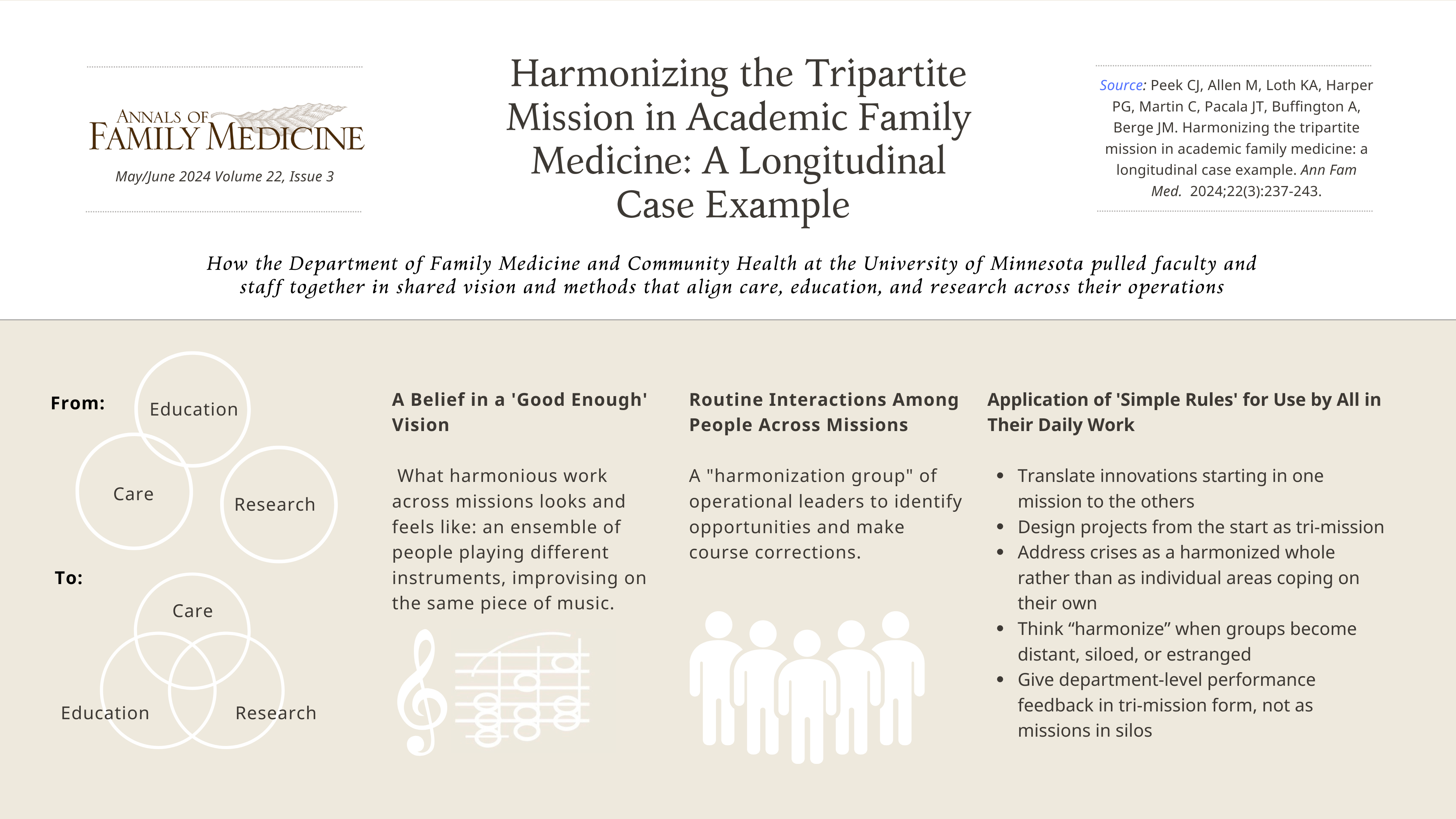
CAS Element Description 1. A good enough vision A general department-level direction or aim. A direction that people can act on locally without telling them exactly what to do or creating complicated plans and coordination. It invites people in all their different roles to act creatively and spontaneously on that shared vision—in their own ways and settings. A “good enough” vision is not to be misunderstood as settling on some modest minimally acceptable goal or compromise. 2. Productive interactions Routine interactions among those working across the missions that produce valuable, new, and unpredictable actions or capabilities unlikely to emerge from any one of them acting within their own role or mission. The whole is greater than the sum of separate parts and is generative of new connections and actions. 3. A few simple rules A small number of agreed-upon guides that inform and drive action and choice among alternatives. These are mutually understood by those persons in routine productive interactions across the missions. The simple rules give coherence to action across disparate actors, settings, and situations and provide a shared basis for creative or novel approaches and actions, even without central direction. CAS = complex adaptive system.
A. Translate an innovation spontaneously arising in any mission area to all mission areas.
Innovations and improvements often arise spontaneously among people doing the work of clinical care, education, and research. Immediately ask “What are the corresponding innovations or improvements for work in the other missions?” For example, how can a change in how care is done quickly affect how residency education is done, and what research questions arise to be answered by those doing the work?B. Design initiatives and projects as tri-mission efforts from the very start.
While many innovations or improvements arise spontaneously, others are deliberately planned initiatives to address a specific issue or make a systemic change. Design these as tri-mission efforts—how the change idea of the initiative plays within each mission area, and what the corresponding actions are in each—a 3-dimensional plan.C. When coping with crisis, use harmonization to stabilize—don’t back off on it.
Habits of harmonization created before a crisis can allow work in all missions to quickly realign to stabilize and work through a crisis. Address crises as a harmonized whole rather than go with a temptation to fragment into areas coping just on their own.D. Think “harmonize” when groups become distant, siloed, or estranged.
Faculty, residents, and staff in different parts of a department can become so distant they misunderstand each other’s actions or motivations. The cause is less likely personal than a system of work susceptible to disconnects and misunderstandings. In short, lack of harmonization. Ask first how well (or not) their work is harmonized—mutually understood and aligned as different parts of a common purpose.E. Give department-level performance feedback in tri-mission form, not missions in silos.
People appreciate knowing “how well we are doing.” Give department-level feedback across the 3 missions in 1 accessible informational format, but not as a judgment or exhortation, so people can take satisfaction (or not) and see for themselves where course corrections are needed. Include a metric or story for “harmonizing” itself in this dashboard.Medication-Assisted Treatment With Integrated Behavioral Health for Opioid Use Disorder Care A community-based residency program responded to the local and national OUD epidemic by developing and implementing a MAT program that included medications for opioid use disorder coupled with integrated behavioral health. The need was great, with high prevalence of OUD among the patient population and community. Education MAT was implemented as a standard part of residency training, qualifying all residents to do MAT after graduation. Onsite behavioral health services complementing MAT were integrated, in keeping with goals to provide care and education within an integrated behavioral health model. Research/scholarship Lead clinicians applied for and received a state innovation and evaluation grant, harmonizing the clinical and educational innovation with the research mission, resulting in 4 publications by faculty and resident co-authors, plus resident quality improvement projects. BIPOC = Black, Indigenous, people of color; MAT = medication-assisted treatment (which includes medications for OUD (MOUD) coupled with behavioral health therapies or support); OUD = opioid use disorder.
Result: This innovation resulted in readily accessible MAT for clinic patients, 25% of whom are BIPOC, with high retention rates (75% for 3 months; 50% for 1 year). All or most graduating residents received the waiver necessary to provide MAT at their post-graduation jobs. Published implementation and evaluation created an evidence base to guide for other residency programs.34-37
Healthy Lifestyles for Kids—the “5-2-1-0” Protocol Research/scholarship Driven by the research mission and “to practice what we know,” this proven intervention was based in a motivational interviewing framework. The 5-2-1-0 protocol brings child health promotion messages to well-child visits. “5” or more fruits or vegetables; “2” or less hours of screen time; “1” or more hour(s) of physical activity; and “0” sugar-sweetened beverages per day. Education Residents were first taught motivational interviewing skills for the 5-2-1-0 intervention and how to apply in well-child visits that include goal setting. Care Residents (and faculty) used the 5-2-1-0 intervention in well-child visits (aged 2-18 years) that included goal setting with parent and child around one of the 5-2-1-0 recommendations. This intervention was tracked in the electronic health record, indicating the parent/child goal, progress on the goal in follow-up visits, and child anthropometry. Result: This intervention was implemented simultaneously by 4 of the department’s residency clinics, stimulating mutual learning, care improvement, and coalescing findings for more robust results. Medical record evidence supported 2 published papers and multiple presentations on a population-level approach to child health promotion.38,39
Clinic as Curriculum (Often Known as “Clinic First”) Education Resident experience in clinic was often seen as unsatisfying compared with the hospital experience,40 attributed to lack of patient and team continuity from erratic clinic schedules pieced together after prioritizing hospital service and rotations. In response, educational leaders launched Clinic as Curriculum across 4 residency clinics with a goal to rebalance resident schedules to (1) make the clinic-based portion reflect more accurately the clinical work they will engage in following graduation and (2) improve faculty and resident well-being. Care Resident education scheduling was inextricably bound to clinic operations and workflow—how care is delivered. And because “Clinic First” literature revealed not only core actions to take,41 but the need for local tailoring of core “building block” ideas,42,43 the 4 residency programs entered a facilitated change process using a common data and evaluation framework to track changes in education and patient care. Research/scholarship Mixed-methods evaluation continuously collected and shared data for iterative improvements across those “building blocks.” Interventions have documented continuity and changes in it, producing insights about perceived importance of continuity and good clinic experience for residents; with practical challenges for balancing complex schedules involving rotations, electives, other duties, and time off. Result: Promising ways to approach scheduling have been piloted—showing effects on continuity and patient and clinician satisfaction as well as feasibility. Computer modeling by an industrial engineer has deepened the work. Two publications have resulted so far.44,45
Pillar Examples: Progress With Diversity, Inclusion, or Equity Care delivery and health Quality metrics stratified by clinic-specific race, ethnicity, language, and insurance status to better address health disparities clinic by clinic Workforce recruitment and retention JEDI climate surveys and root cause analysis leading to changes in faculty recruitment processes Learner recruitment and training Resident recruitment season with explicit training and guidance in recognizing and reducing implicit bias in interviewing Research participation and trust Significant community-engaged research with community collaboration on jointly conceived projects EDI = equity, diversity, and inclusion; JEDI = justice, equity, diversity, and inclusion.
Result: These and other examples across missions have involved interaction between people working in different areas and with different driving interests in JEDI; a whole department journey and “dashboard,”46,47 not separate mission by mission.
Additional Files
SUPPLEMENTAL MATERIALS IN PDF FILE BELOW
- PeekSupp.pdf -
PDF FILE
- PeekSupp.pdf -
VISUAL ABSTRACT IN PNG FILE BELOW
- PeekVisualAbstract.png -
PNG FILE
- PeekVisualAbstract.png -




{kind=link}