
Article Figures & Data
Figures
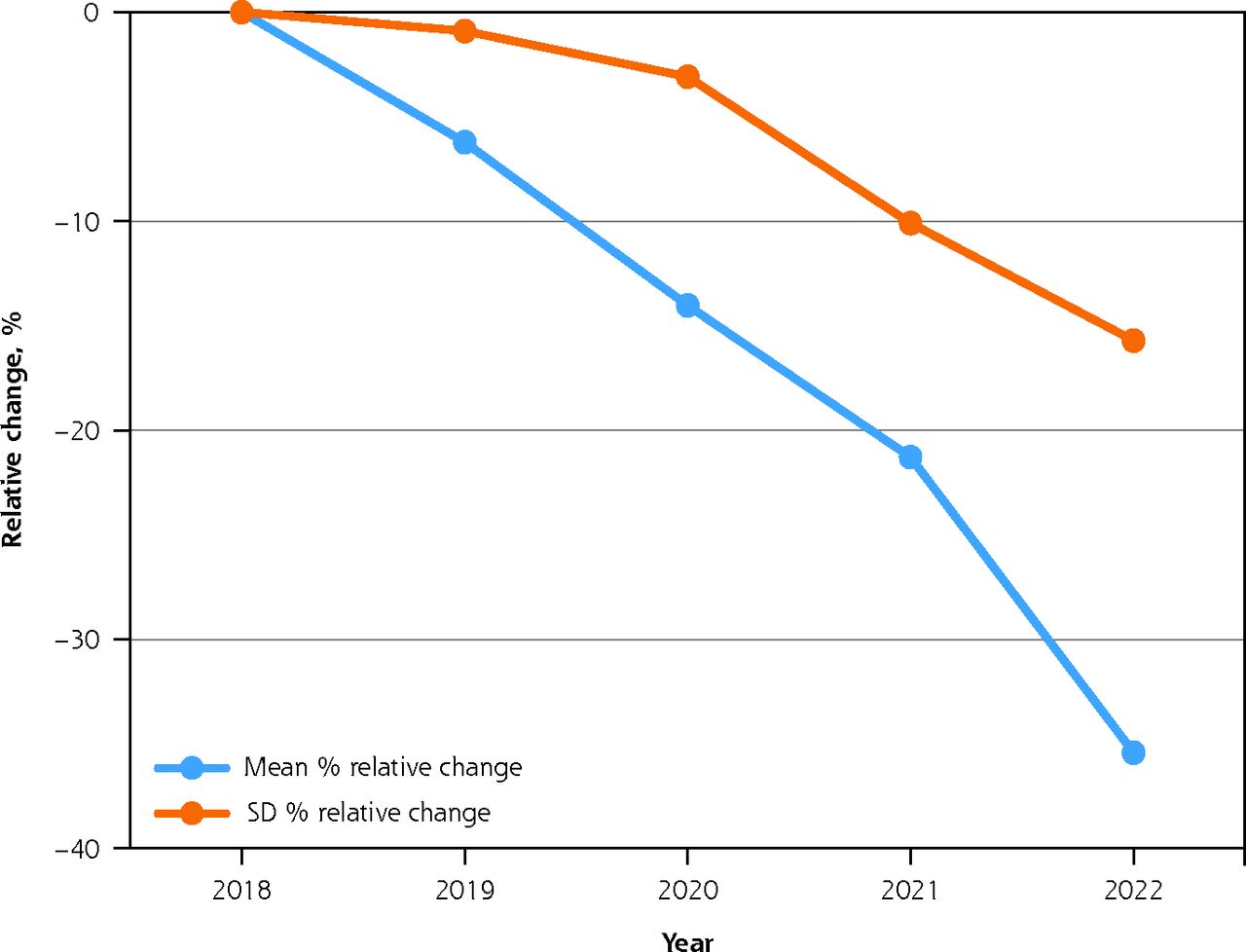
- Figure 1.
Relative changes in English practices’ longitudinal continuity of care, 2018-2022.
GP = general practitioner; LCoC = longitudinal continuity of care.
Notes: Figure shows relative change in percentage of practice patients reporting LCoC. LCoC was calculated as 100 × (percentage of patients with preferred GP × percentage of patients able to see preferred GP).
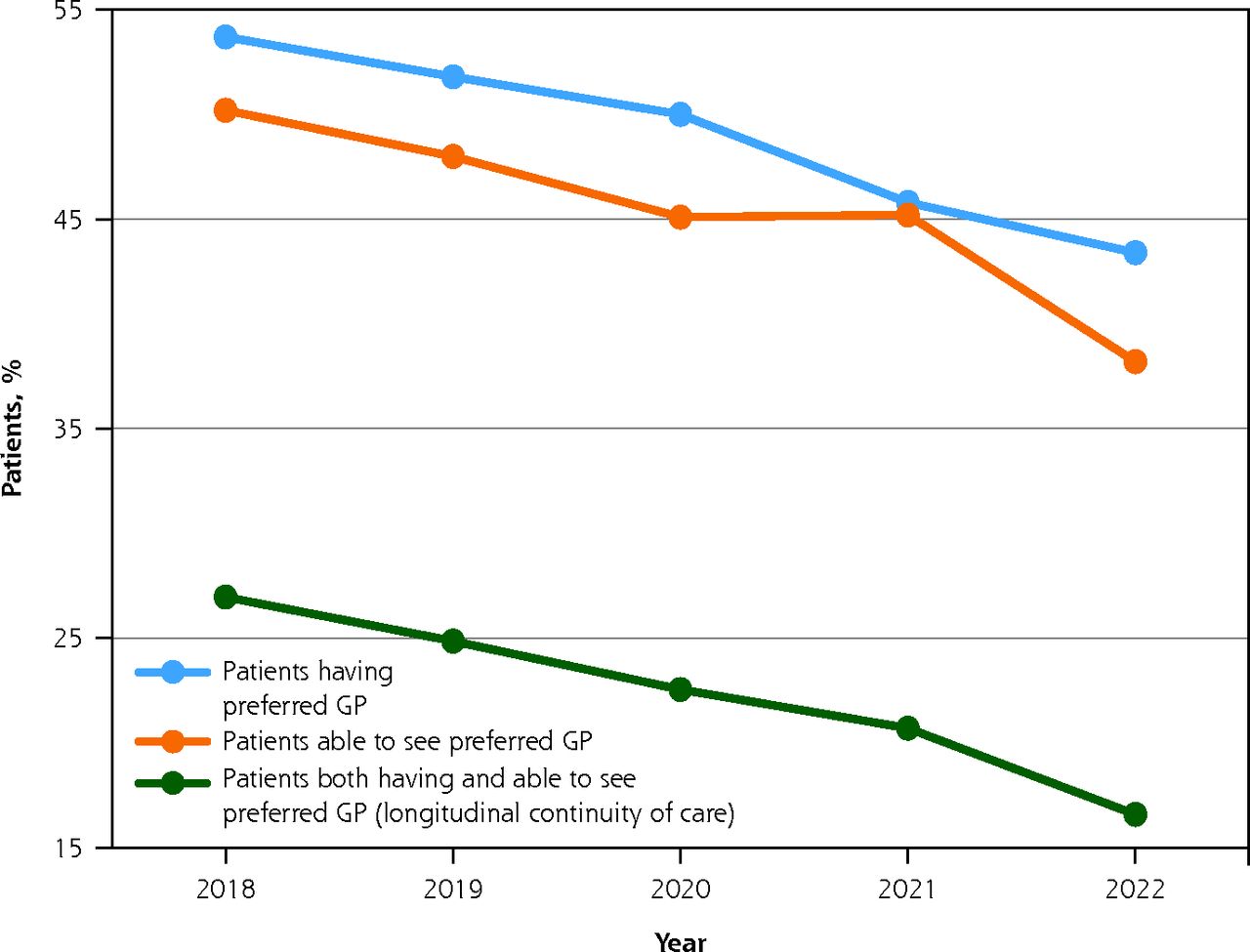
- Figure 2.
Practice-level continuity of care measures as reported by patients on the GPPS, 2018-2022.
GP = general practitioner; GPPS = General Practice Patient Survey.
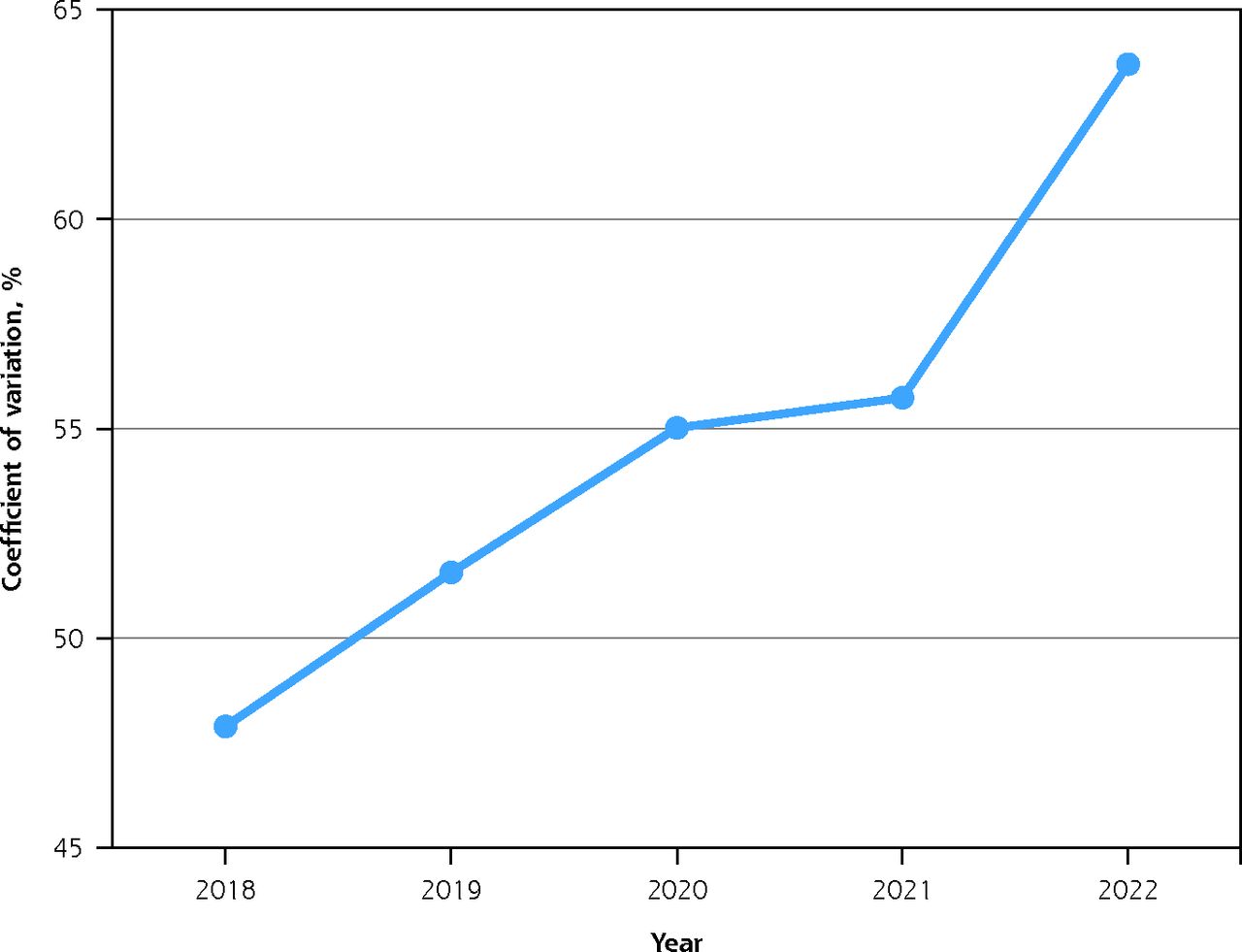
- Figure 3.
Variation across practices in longitudinal continuity of care, 2018-2022.
Note: Coefficient of variation is calculated as the SD divided by the mean. Exact values are 48.1% (2018), 51.0% (2019), 54.5% (2020), 55.4% (2021), and 63.6% (2022).



Tables
Variable 2018
Median (IQR)2019
Median (IQR)2020
Median (IQR)2021
Median (IQR)2022
Median (IQR)Dependent variable Patients reporting LCoC, % 27.5 (18.6-38.0) 25.5 (16.9-36.1) 22.9 (14.9-33.7) 21.0 (13.6-30.5) 16.66 (10.1-25.2) Independent variables IMD scorea … 21.2 (14.0-30.4) … … … White patients, % 92.8 (75.9-97.8) 92.4 (75.8-97.6) 92.1 (74.9-97.5) 91.2 (72.3-97.0) 90.3 (71.0-96.8) List size 7,711 (4,996-11,110) 7,907 (5,165-11,394) 8,052 (5,299-11,685) 8,147 (5,378-11,825) 8,308 (5,475-12,028) NHS payments per patient, £b … 146.40 (131.79-167.55) 146.52 (132.33-166.76) 149.66 (134.34-171.44) 152.85 (136.97-173.84) GPs per 1,000 patients 0.53 (0.40-0.69) 0.53 (0.40-0.70) 0.54 (0.40-0.71) 0.54 (0.39-0.73) 0.55 (0.39-0.74) Nurses per 1,000 patients 0.24 (0.16-0.33) 0.24 (0.16-0.34) 0.24 (0.16-0.35) 0.23 (0.15-0.34) 0.23 (0.15-0.34) Patients seen on same day, % 30.1 (22.0-41.6) 30.3 (21.7-41.3) 30.2 (21.9-40.7) 34.2 (25.2-43.7) 32.2 (22.6-43.7) GP = general practitioner; GPPS = General Practice Patient Survey; IMD = Index of Multiple Deprivation; IQR = interquartile range; LCoC = longitudinal continuity of care (based on GPPS); NHS = National Health Service.
Note: Only medians and IQRs are shown here, as the majority of variables were not normally distributed. More detailed statistics, including means, SDs, and missing values for these variables, are provided in Supplemental Table 5.
↵a The lowest IMD score was 3.4 and the highest was 68.7. Higher values denote higher levels of deprivation. Value for 2019 was used for all years.
↵b The 2018 data were not used because method of calculating payments changed in 2018-2019.
Variable Practices, No. (%) NHS region London 1,127 (18.4) South West 521 (8.5) South East 783 (12.8) Midlands 1,212 (19.7) East of England 631 (10.3) North West 920 (15.0) North East and Yorks 944 (15.4) Unknown 1 (<0.1) Location Urban 5,109 (83.2) Rural 1,030 (16.8) Contract type in 2020 GMS 4,409 (71.8) PMS 1,598 (26.0) APMS 132 (2.2) APMS = Alternative Provider Medical Services; GMS = General Medical Services; NHS = National Health Service; PMS = Personal Medical Services.
Predictor Coefficient (95% CI) P Value Intercept (coefficient of time) 0.18 (−0.32 to 0.68) .48 Baseline LCoC (2018) −0.08 (−0.09 to −0.07) <.001 Index of Multiple Deprivation score −0.007 (−0.011 to 0.003) .07 Region (ref = London) South West −0.26 (−0.58 to 0.06) .11 South East −0.32 (−0.60 to −0.04) .02 Midlands −0.59 (−0.84 to −0.33) <.001 East of England −0.41 (−0.70 to −0.11) .007 North West −0.57 (−0.85 to −0.28) <.001 North East and Yorks −0.24 (−0.52 to 0.05) .10 Location: rural (ref = urban) −0.01 (−0.24 to 0.23) .96 White patients −0.012 (−0.014 to −0.010) <.001 List size (thousands) 0.003 (−0.01 to 0.02) .68 GPs per 1,000 patients 0.38 (0.11 to 0.65) .005 Nurses per 1,000 patients 0.45 (−0.10 to 0.99) .11 Contract type in 2020 (ref = GMS) APMS 0.25 (−0.29 to 0.80) .36 PMS 0.21 (0.05 to 0.38) .01 NHS payment per patient (per £10s) 0.01 (−0.01 to 0.03) .38 Patients seen same day 0.008 (0.005 to 0.011) .003 APMS = Alternative Provider Medical Services; GMS = General Medical Services; GP = general practitioner; LCoC = longitudinal continuity of care; PMS = Personal Medical Services; ref = reference.
Notes: Multilevel mixed-effects model with time interactions. Dependent variable (outcome) was the percentage of practice patients reporting LCoC, calculated as 100 × (percentage of patients with preferred GP × percentage of patients able to see preferred GP). A positive coefficient indicates a slower rate of decline over time, whereas a negative coefficient indicates a faster rate of decline over time. For example, a coefficient value of 0.38 for GPs per 1,000 patients means that for each 1-unit increase in the number of GPs/1,000, the slope of the decline in the outcome (continuity) would have been 38% better (or less steep in this context) over the study period, after adjusting for all the other predictors. A coefficient value of −0.08 for baseline continuity (in 2018) means that for each 1-unit (% in this case) increase in baseline continuity, the slope of the decline would have been 8% worse (or steeper in this context) over the study period, after adjustment. Model is based on 6,010 practices and 21,565 observations. The intraclass correlation coefficient is 0.51. The conditional R2 is 0.83. The full output of the model, including fixed effects without time interactions, is provided in Supplemental Table 7.
SUPPLEMENTAL MATERIALS IN PDF FILE BELOW
- Levene-Supp.pdf -
PDF FILE
- Levene-Supp.pdf -
VISUAL ABSTRACT IN PNG FILE BELOW
- Levene_VA.png -
PNG FILE
- Levene_VA.png -
PLAIN-LANGUAGE ARTICLE SUMMARY
Original Research
Pandemic Lockdown Exacerbated Ongoing Declines in Continuity of Care
Within English General Practices
Background and Goal: Longitudinal continuity of care is the repeated contact between an individual and the same general practitioner (GP). This type of continuity of care is widely regarded as a cornerstone of primary care. Higher levels of longitudinal continuity of care are associated with better health outcomes, greater patient satisfaction, and more cost-effective use of health care resources. This study aimed to describe more recent variations between practices in the slopes of longitudinal continuity of care levels across the COVID-19 pandemic. The study also set out to determine if practice-related factors predicted these variations.
Study Approach: Researchers used the General Practice Patient Survey for the period of 2018- 2022 to analyze data from English general practices with longitudinal continuity of care information. The study included only active practices with at least 750 registered patients. The outcome was the percentage of each practice’s patients who had both a preferred GP and the ability to see that GP repeatedly. The study examined eleven population and practice related factors as potential independent predictors of longitudinal continuity of care variation. Factors included baseline longitudinal continuity of care (in 2018), English National Health Service (NHS) region (London, South East, South West, East of England, Midlands, North East and Yorkshire, or North West), deprivation score, rurality (urban or rural), percentage of White patients and numbers of general practitioners and nurses per 10,000 patients.
Main Results:
-
Overall Decline in Continuity: In 2018-2022, the mean of longitudinal continuity of care levels across 6,010 practices decreased markedly from 29.3% to 19.0% of patients.
-
Steeper Decline Post-COVID-19 Lockdown: This decline steepened in 2021- 2022, following the COVID-19 lockdown.
-
Increasing Variations in Continuity: The coefficient of variation (a measure of relative variability) increased from 48.1% to 63.6% in 2018-2022, indicating progressively widening differences between practices.
-
Predictors of Variations in Decline of Continuity:
-
More general practitioners and higher percentages of patients seen on the same day as booking predicted slower declines.
-
Higher baseline longitudinal continuity of care, living in four of the six regions outside London, and higher percentages of White ethnicity predicted faster declines.
Why It Matters:The findings suggest that factors linked to greater appointment availability predicted slower declines in longitudinal continuity of care levels in English general practices. To prevent the further loss of continuity, the researchers urge immediate nationwide action to improve appointment availability.
Visual Abstract:
-





{kind=link}
{kind=link}
{kind=link}
{kind=link}