
Article Figures & Data
Figures
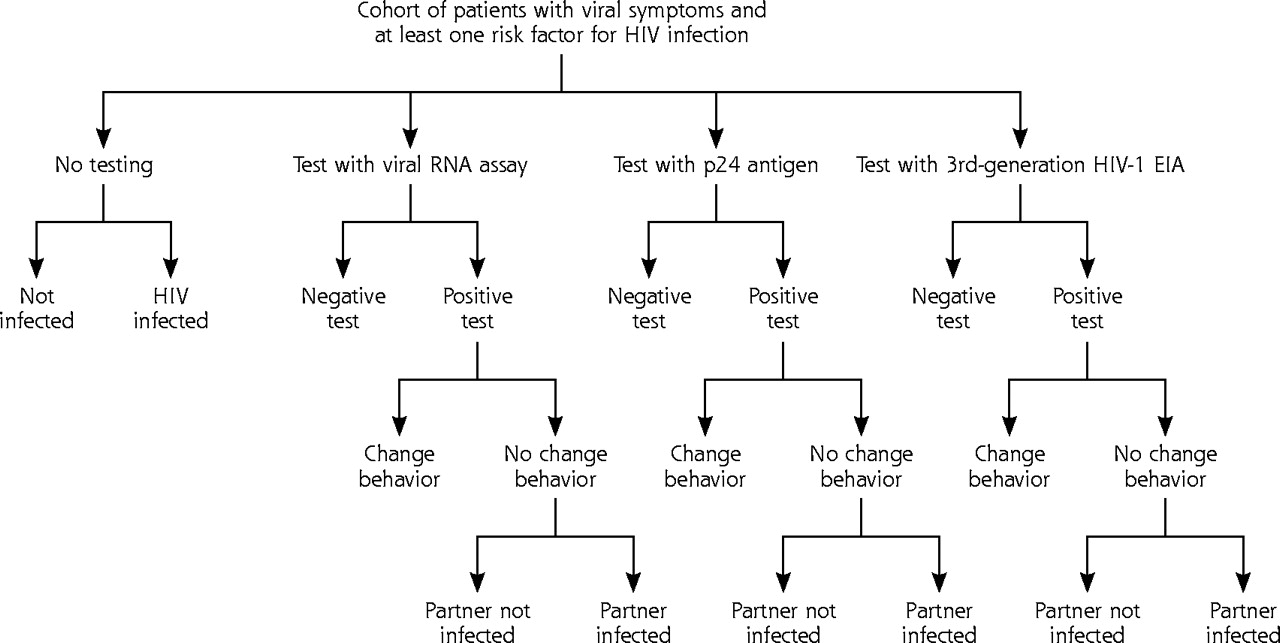
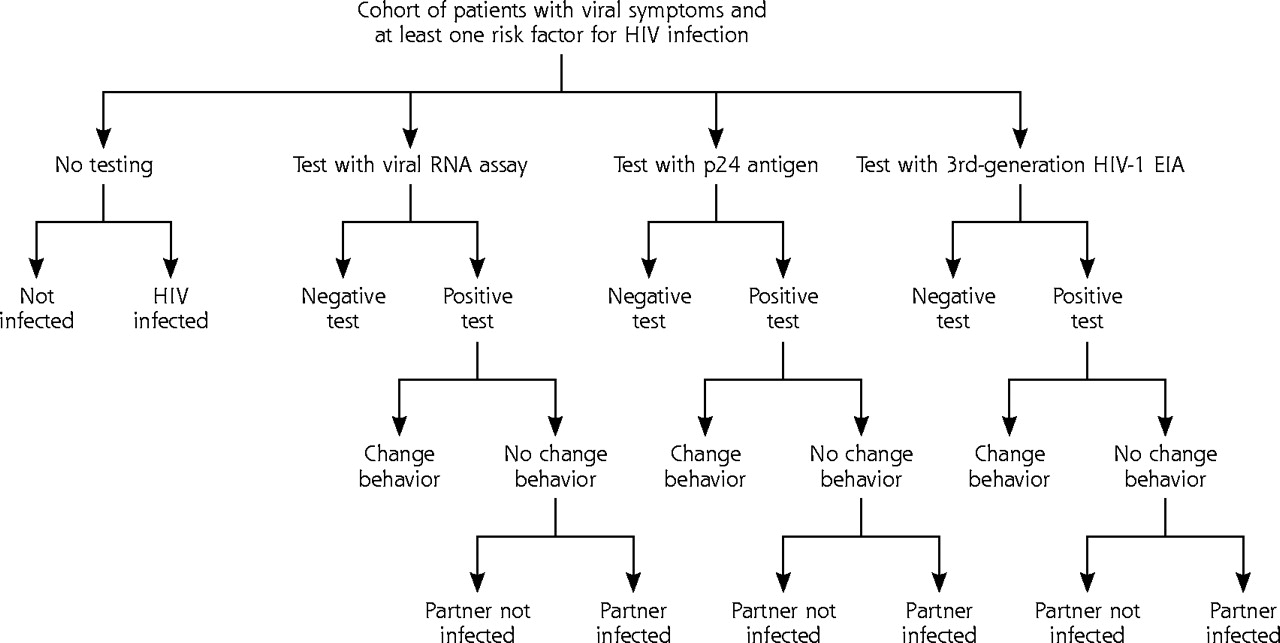
- Figure 1.
Decision tree for cost-effectiveness of expanded testing for primary human immunodeficiency virus (HIV) infection showing outcomes for patients and partners.
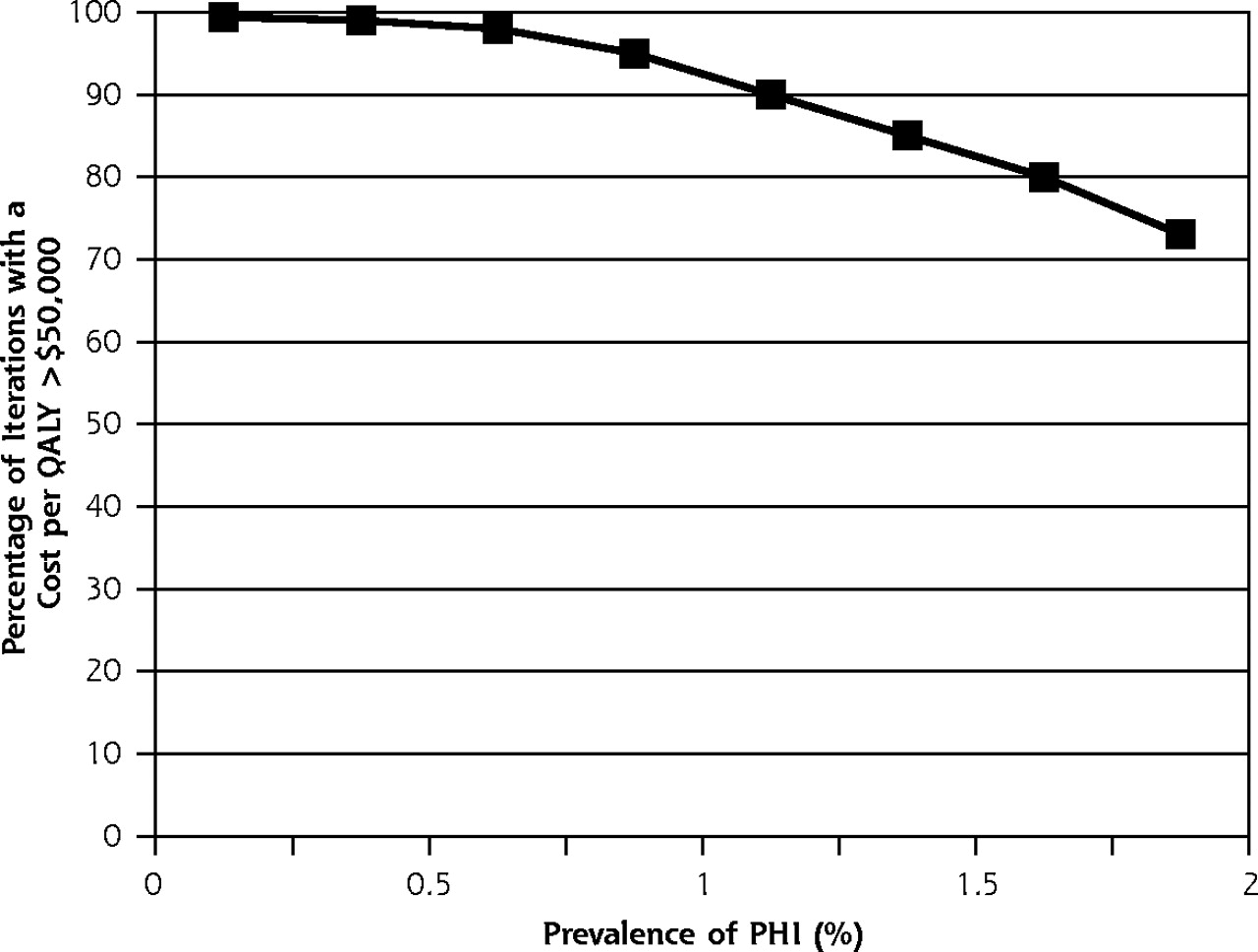
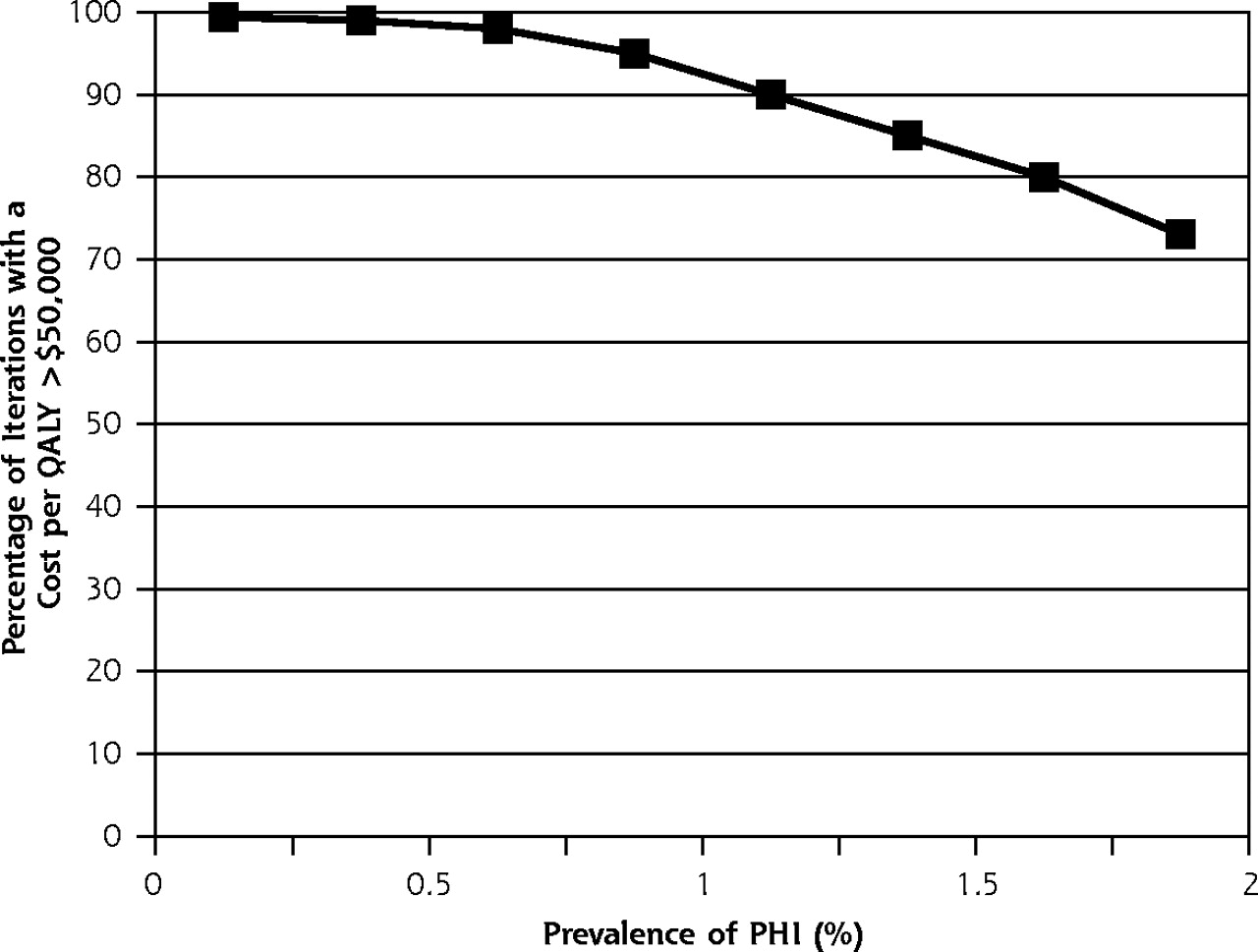
- Figure 2.
Probabilistic sensitivity analysis, p24 antigen EIA compared with no testing.
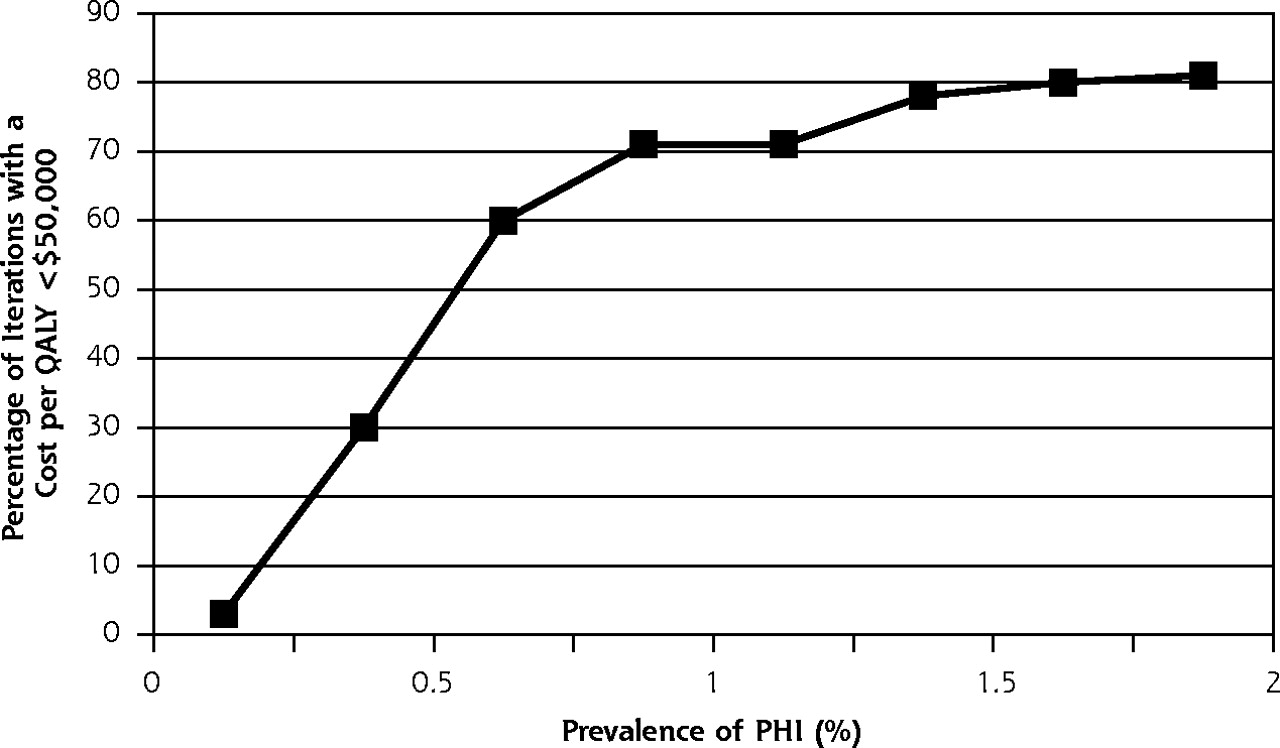
- Figure 3.
Probabilistic sensitivity analysis, HIV-1 RNA assay compared with p24 antigen EIA.

Tables
Variable Baseline Estimate Range Used in Sensitivity Analysis Source EIA = enzyme immunosorbent assay; HIV = human immunodeficiency virus; PHI = primary HIV infection; CBC = complete blood count; G6PD = glucose-6-phosphate dehydrogenase; CMV = cytomegalovirus; RPR = rapid plasma reagin; PPD = purified protein derivative (tuberculin); NAAT = nucleic acid amplification test. * Initial battery of laboratory tests includes: CBC, chemistry panel, G6PD assay, toxoplasmosis titer, CMV titer, RPR, PPD skin test, viral hepatitis panel, lipid panel, urinalysis, chest radiograph, urine NAAT for gonorrhea and chlamydia. Costs ($) p24 antigen EIA 24.65 12.33–49.30 Medicare fee schedule HIV-1 RNA assay 118.89 59.45–237.78 Medicare fee schedule Third-generation HIV-1 EIA 19.17 9.59–38.34 Medicare fee schedule Western blot assay 27.05 13.53–54.10 Medicare fee schedule CD4 cell count per microliter 90 45–180 Medicare fee schedule Initial battery of laboratorys tests (new diagnosis)* 254 200–614 Medicare fee schedule Expanded testing program costs 101.47 51–203 MMWR20 Discounted lifetime medical costs (diagnosed with PHI and antiretroviral therapy started at CD4 cell count of 350/μL) 95,800 47,900–191,600 Freedberg et al23 Discounted lifetime medical costs (PHI not diagnosed and antiretroviral therapy started when HIV diagnosed) 88,100 44,050–176,200 Freedberg et al23 Return visit 52.53 40–67.86 Kaplan & Anderson24 Test characteristics p24 antigen EIA, sensitivity 0.887 0.770–0.957 Hecht et al,8 Daar et al9 Specificity 0.9996 0.9950–0.9999 Hecht et al,8 Daar et al9 HIV-1 RNA, sensitivity 1.000 — Hecht et al,8 Daar et al9 Specificity 0.980 0.950–0.999 Hecht et al,8 Daar et al9 Third-generation HIV-1 EIA, sensitivity 0.790 0.600–0.920 Hecht et al8 Specificity 0.970 0.930–0.990 Hecht et al8 Probability of indeterminate Western blot 0.000004 — Kleinman et al22 Prevalence factors (%) Patients lost to follow-up 31 16–62 MMWR21 Prevalence in screened population 0.66 0.53–0.92 Coco & Kleinhans16 Sexual transmission factors Patients who change behavior to avoid infecting sexual partner 50 0–96 MMWR6 Patients that are sexually active 50 25–85 MMWR6 Infectivity (probability of sexual transmission during PHI period) 15 0–30 Yerly et al,25 Pilcher et al26 Utilities Asymptomatic HIV infection 0.937 0.926–0.949 Schackman et al27 Anxiety while waiting for confirmatory test results for patients with a positive screen 0.682 0.400–0.800 Kaplan & Anderson24 Quality-adjusted life-expectancy (discounted), years No PHI 24 — NCHS15 Positive screening result, no PHI 23.9735 23.950–23.983 NCHS,15 Kaplan & Anderson24 PHI diagnosed at screening with follow-up care and antiretroviral treatment started at CD4 cell count of 350/μL 11.9 11.832–11.952 Freedberg et al23 PHI not diagnosed at screening or lost to care with antiretroviral treatment started when HIV diagnosed 11 — Freedberg et al23 - Table 2.
Cost, Effectiveness, and Incremental Cost-Effectiveness of Expanded Testing for Primary HIV Infection of 3,030,303 Hypothetical Patients at a Prevalence of 0.66% With Third-Generation HIV-1 EIA, p24 Antigen EIA, and HIV-1 RNA Assay
Variable No Testing Third-Generation HIV-1 EIA p24 Antigen EIA HIV-1 RNA Assay Note: each column is compared with the one to the left. HIV = human immunodeficiency virus; EIA = enzyme immunosorbent assay; QALYs = quality-adjusted life-years. * Dominated means this option cost more and was less effective than other options. Cost (millions), $ 1,762.1 2,233.6 2,258.2 2,561.8 Incremental cost (millions), $ — 471.5 24.6 303.6 Effectiveness (thousands) QALYs 69,710.0 69,720.8 69,726.1 69,725.8 Incremental effectiveness, QALYs — 10,800 5,300 (300) Effectiveness, No. Primary HIV infection cases diagnosed — 15,803 17,054 20,000 Primary HIV infection cases lost to care (31% of those diagnosed) 20,000 4,899 5,287 6,200 False-positive diagnoses — 90,257 1,127 59,169 False-negative diagnoses — 2,924 3,012 0 Cases avoided per behavior change 403 435 501 Cost-effectiveness, $ Testing cost per case identified — 29,836 29,090 39.985 Incremental cost per quality-adjusted year of life gained — Dominated* 30,800 Dominated* - Table 3.
Changes in Incremental Cost per Quality-Adjusted Life-Year in Key 1-Way Sensitivity Analyses
EIA = enzyme immunosorbent assay; HIV = human immunodeficiency virus; PHI = primary HIV infection. -
Doubling the cost of lifetime medical care for patients being observed to CD4 cell counts of 350/μL or seeking care at later stages of infection ($88,100/$95,800 to $176,050/$191,600) increased the cost of expanded testing with the p24 antigen EIA from $30,800 to $34,100 compared with no testing
-
Doubling the expanded testing and counseling enrollment program costs ($101.47 to $203), increased the cost of the p24 antigen EIA testing option to $49,800 compared with no testing
-
Increasing the specificity of the HIV-1 RNA assay (0.98 to 0.999) decreased the cost of the HIV-1 RNA assay option to $142,000 compared with the p24 antigen EIA option
-
Assuming no benefit to sexual partners of patients with PHI, ie, no cases avoided through changes in behavior, increased the cost of the p24 antigen EIA to $50,600 when compared with no testing
-
The Article in Brief
The Prevalence of Primary HIV Infection in Symptomatic Ambulatory Patients
By Andrew Coco, M.D., and colleague
Background: Approximately 40,000 new cases of HIV infection are identified each year in the United States. Primary HIV infection refers to the early, flu-like symptoms associated with HIV disease. Diagnosis of Primary HIV is an opportunity to help prevent the disease from being transmitted. This study set out to estimate how many patients visiting the doctor�s office, emergency department, or hospital clinic for fever, rash, or sore throat have primary HIV infection.
What this study found: Based on data from a large national survey, the study estimates that primary HIV infection would be found in 0.66 percent of patients complaining of fever, 0.56 percent of patients with rash, and 0.13 percent of patients with sore throat.
Implications
� This is the first study to estimate the rate of primary HIV infection.
� The study results can help policy makers develop national guidelines for HIV testing.




{kind=link}
{kind=link}
{kind=link}